
Abstract
Background:
Several government schemes exist for the welfare of families having children with intellectual and developmental disorders (IDDs) in India. However, these schemes are often not utilized. An understanding of the barriers to access these social welfare benefits, especially in rural areas of India, can aid in planning social action toward the implementation of these schemes.
Methods:
A situation analysis of the resources and potential barriers to access social welfare benefits for families of children with IDD was conducted in a rural community. Stakeholder interviews were conducted with families of children with IDD (n = 20), government officials responsible for implementing education at the state level (n = 5), local officials responsible for facilitating social welfare benefits (n = 5), and nongovernmental organization (
Results:
Barriers encountered by families of children with IDD, local officials, and NGOs included lack of awareness about the available welfare schemes, unavailability of social welfare facilities in the local areas, lack of social auditing in the provision of social welfare schemes to the needy, and stringent process of application and regulation for financial aid under the National Trust schemes.
Conclusion:
There are multiple barriers to access social welfare benefits for families having children with IDD in rural Karnataka. There is a strong need to empower families, sensitize local officials, and advocate for social policies to effectively implement National Trust schemes in rural areas of Karnataka.
Keywords
In India, several government schemes exist for the welfare of the persons with IDD, but they are not utilized. Needs of families of children with IDD were provision for special schools, daycare centers, and social welfare schemes. Barriers in accessing social welfare schemes included lack of awareness, lack of social welfare facilities, lack of social auditing, and stringent process of application.Key Messages:
There is a strong need to empower families, sensitize local officials, and advocate for social policy change. Children with intellectual and developmental disabilities (IDDs) are vulnerable to exclusion from health services and community resources. 1 Family caregivers face challenges in planning for the future of these children due to (a) lack of services, which includes special school, trained teachers, physiotherapist, aids, and appliances, (b) financial challenges, (c) reluctance from the family members, (d) lack of time, (e) emotional nature of future planning, (f) inertia, and (g) absence of family members for providing care for the children with IDD. 2 In such conditions, the families of children with IDD face significant financial, social, and psychological burden in the process of providing care.
Many families of children with IDD depend on government social welfare schemes, which leads to limited access to care and poor health outcomes. 1 In India, several government schemes exist for the welfare of the persons with IDD, but are not utilized due to the lack of awareness and red-tapism. 2 Some schemes given in the National Trust Act (1999), 3 such as Disha (early intervention and school readiness), Vikaas (daycare), Niramaya (health insurance), Sambhav (aids and assistive devices), Sahayogi (caregiver training), Prerna (marketing assistance), Gyan Prabha (educational support), Gharaunda (group home for adults), and Badthe Kadam (awareness and community interaction), cannot be utilized by the person with IDD directly. A nonprofit organization can facilitate the provision of government programs, such as education and short-stay and long-stay homes. However, there is a significant difference in the availability and implementation of the above-mentioned government schemes in rural and urban areas as the majority of the nongovernmental organizations (NGOs) working for children with IDD and their families are located in the urban areas. 4
Understanding the barriers to access social welfare benefits (rural or urban) using the methodology of situation analysis can aid in planning suitable social action toward the implementation of these schemes. Situation analysis is a method of analysis primarily used in management practice or the development sector. Off late, it has been used in health research and policymaking. It comprises different methods (SWOT analysis, situational mapping, etc.) to understand the point of analysis (organization/policy/service delivery) from its macro- and microenvironment. 5 A situation analysis is the second and critical step based on which the objectives, budget, strategy, execution, and evaluation of service delivery or action research or social policy are developed. It helps in understanding social policy barriers related to opinions and experiences of stakeholders to detect the gaps between the current state and the desired state. This process helps in defining the nature and scope of a problem and creates the best course of action to take during the program. 6
For this population, there have been no studies or situational analysis conducted in India to understand the barriers to access healthcare services, social policy, and social welfare benefits, either in the urban or rural settings. In this context, the research team conducted a situation analysis of the resources and potential barriers to access social welfare benefits for families of children with IDD in a rural community of Karnataka.
Materials and Methods
The Institute Ethics Committee of National Institute of Mental Health and Neurosciences (NIMHANS) approved the study. An inductive qualitative method was adopted for this study. Data were collected from the users and other stakeholders between November 2017 and November 2018.
Setting
Thirthalli taluk, in Shimoga, Karnataka state, India, was the universe of the study. The reason for selecting Thirthalli was that there was already a mental health project in this area for the persons with mentally ill. Furthermore, several families in the village were asking for help in procuring welfare benefits for the disabled. Out of the eight primary health centers (PHCs) in Thirthalli taluk, one PHC in the Konandur locality was selected using a simple random sampling design (chit-chat method). According to the population census of 2011, 7 the Konandur locality has 996 families, with a population of 3973. An area within a 5-km radius from Konandur town was selected for the study. A social worker was trained to identify children with IDD (below the age of 18 years, according to the Juvenile Justice Act 2015).
Sample and Design
The research team contacted 200 households in the area in liaison with the Accredited Social Health Activist workers and auxiliary nurse midwife from the local PHC and local leaders. The social worker identified 20 families of children with IDD through a door-to-door survey and snowball sampling technique. We used a clinical interview method and verifications of the child’s health records. Two families cooperated for data collection, but refused the help of the research team in getting social welfare benefits.
Situational mapping was used 6 to map all stakeholders’ viewpoints through the technique of qualitative interviews and observation.
Assessments and Process as the Study
The social worker collected sociodemographic details and burden from 20 families, 8 and assessments were done to understand the requirements for taking care of their children with IDD. The economic status of the family was assessed by checking if the family possessed a government food and civil supplies below poverty line card. The burden of the family was assessed using the Burden Assessment Schedule,7,8 which assesses both objective and subjective burden experienced by the primary caregivers of chronic patients with mental disorders. The qualitative needs assessment schedule, which was developed by the research team, elicited the needs of the family members in taking care of their children with IDD, especially in the areas of education and social welfare benefits. The Interview Schedule (see the appendix) was developed through qualitative interviews with six mental health professionals (two psychiatrists, three psychiatric social workers, and one NGO professional) who had worked in the area of psychosocial rehabilitation of persons with IDD (Table 1). It takes around 30–45 min to administer, and the steps involved in interviewing the family include rapport building with the family, asking about their basic sociodemographic details, eliciting their needs, and understanding the barriers faced by them in procuring welfare benefits and services. The interview was ended by providing details of the welfare benefits that the families could avail from contact details of nearest PHC and Manochaitanya camp (mental health clinic at the district level as part of District Mental Health Programme, Government of Karnataka).
Interview Questions Asked to Various Stakeholders
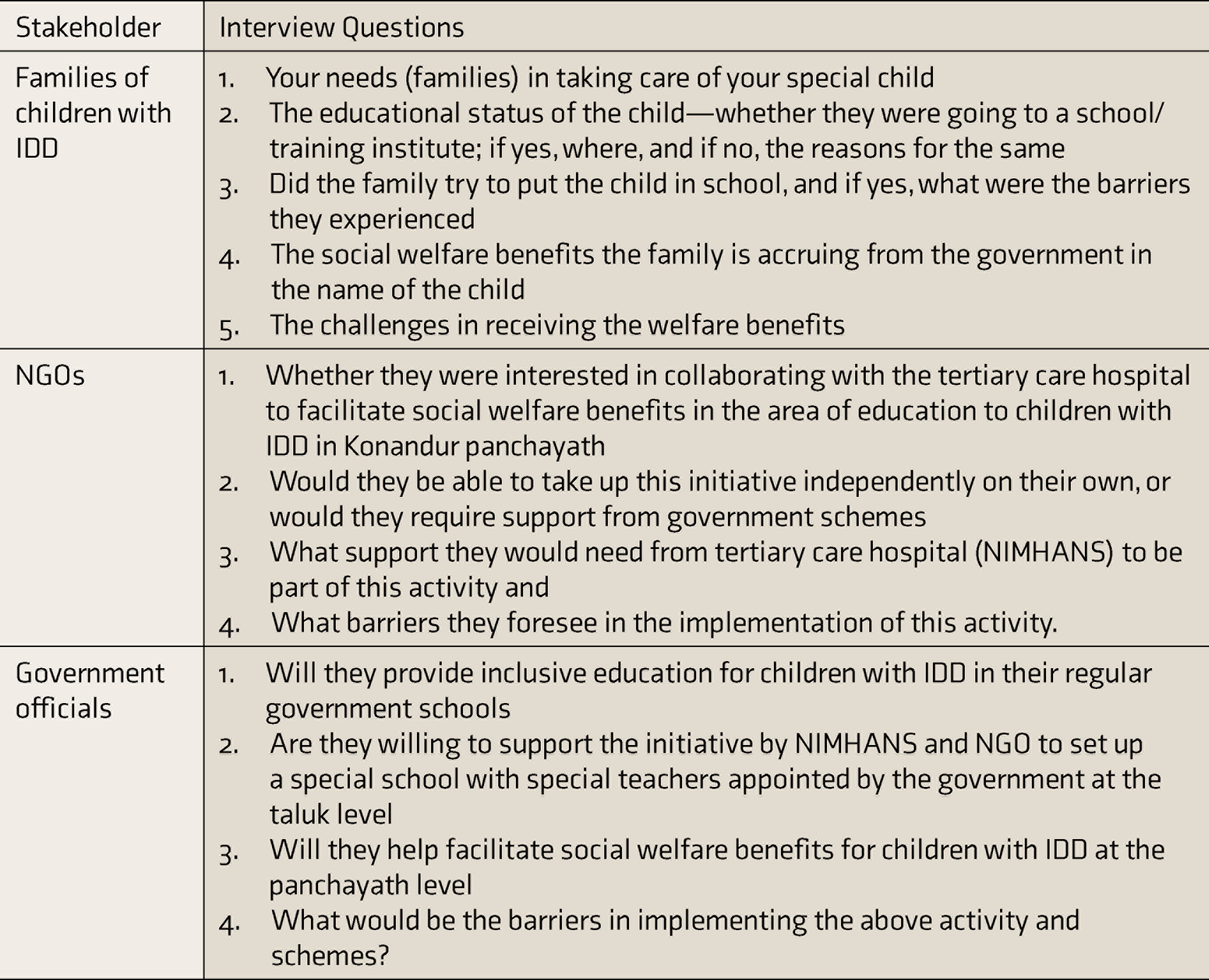
Discussions with NGOs (n = 3) interested in working in the area were conducted (Table 1). As there were no NGOs registered under the National Trust Act 1999 in Shimoga district, two NGOs from other districts (Chikkamagalur and Chikkaballapur) were contacted from the list of registered NGOs under the National Trust Act 1999. The NGOs work with children with intellectual and developmental disorders (IDDs), and the second organization is located in Chikkaballapur district, Karnataka, and runs a daycare center for children with IDD. A third NGO from Bengaluru urban district was approached to partner in this initiative. This NGO was working for children with IDD and was successfully running a daycare center. However, as this NGO too was not registered under the National Trust Act 1999, they were unable to collaborate in this initiative.
The government officials responsible for implementing education at the state level (n = 5) and the local officials responsible for facilitating social welfare benefits (n = 5; village accountant, panchayath development officer, and treasurer, tehsildhar (Chief administrative officer at the local community level)) were mapped and interviewed to complete the situational analysis (Table 1).
The qualitative data collected in this study are considered to be trustworthy as the procedure of data generation and management has been transparent and explicitly explained. The credibility of the data can be considered good as adequate descriptions of the context of the study have been made, which can be recognizable to people who share the experience (families) and those who care for or treat them (mental health professionals). Furthermore, triangulation of the data generated from the families, officials, and experiential account of barriers encountered in facilitating welfare benefits adds to the credibility of the data. Although the applicability of this data generated can be low as it may not be generalizable to the larger group of families of IDD from other socioeconomic backgrounds, such as urban cities, the fact that all households in Konandur town were surveyed and their needs were elicited shows that it is representative of the people staying in this panchayath . Similar patterns of data could be found if this study was conducted in other rural panchayaths, detailing its moderate consistency value. 9
Analysis
A mixed-method analysis was used to understand the results of the situation analysis. The quantitative data were recorded in datasheets, the qualitative data was manually recorded during the interview, and the social worker transcribed the postinterview information. A six-step approach to thematic analysis, by Braun and Clarke, 10 was used in order to provide a rationale for the decisions made. They included (a) familiarity with recorded data by reading and rereading transcripts and making important notes about the data while listening to the recordings; (b) generating initial codes by open semantic codes and refining them through discussions; (c) searching for themes in reference to the codes for the purpose of understanding the needs and barriers of the families separately; (d) reviewing the themes to cluster them based on unifying features; (e) defining and naming themes in relation to the research question and in keeping with the essence of the data collected from the experts; and (f) two components (i) needs of families and (ii) barriers to procuring welfare benefits. 6 The thematic analysis was carried out mainly by the first and second authors. The fifth author was involved in deciding if there were any contentious differences in thematic analysis between the first two authors. Triangulation of the qualitative data collected from the families, officials, and discussions with NGOs was conducted to arrive at the final themes.
Results
The demographic details of the 20 children with IDD and their caregivers who were contacted for assessing the needs are provided in Table 2. The mean (SD) age of the children with IDD was 9.7 (3.18) years, and the mean burden score of the families with children with IDD was 67.3 (7.66), indicating moderate burden experienced.
Sociodemographic Profile of Children and Families With IDD (n=20)
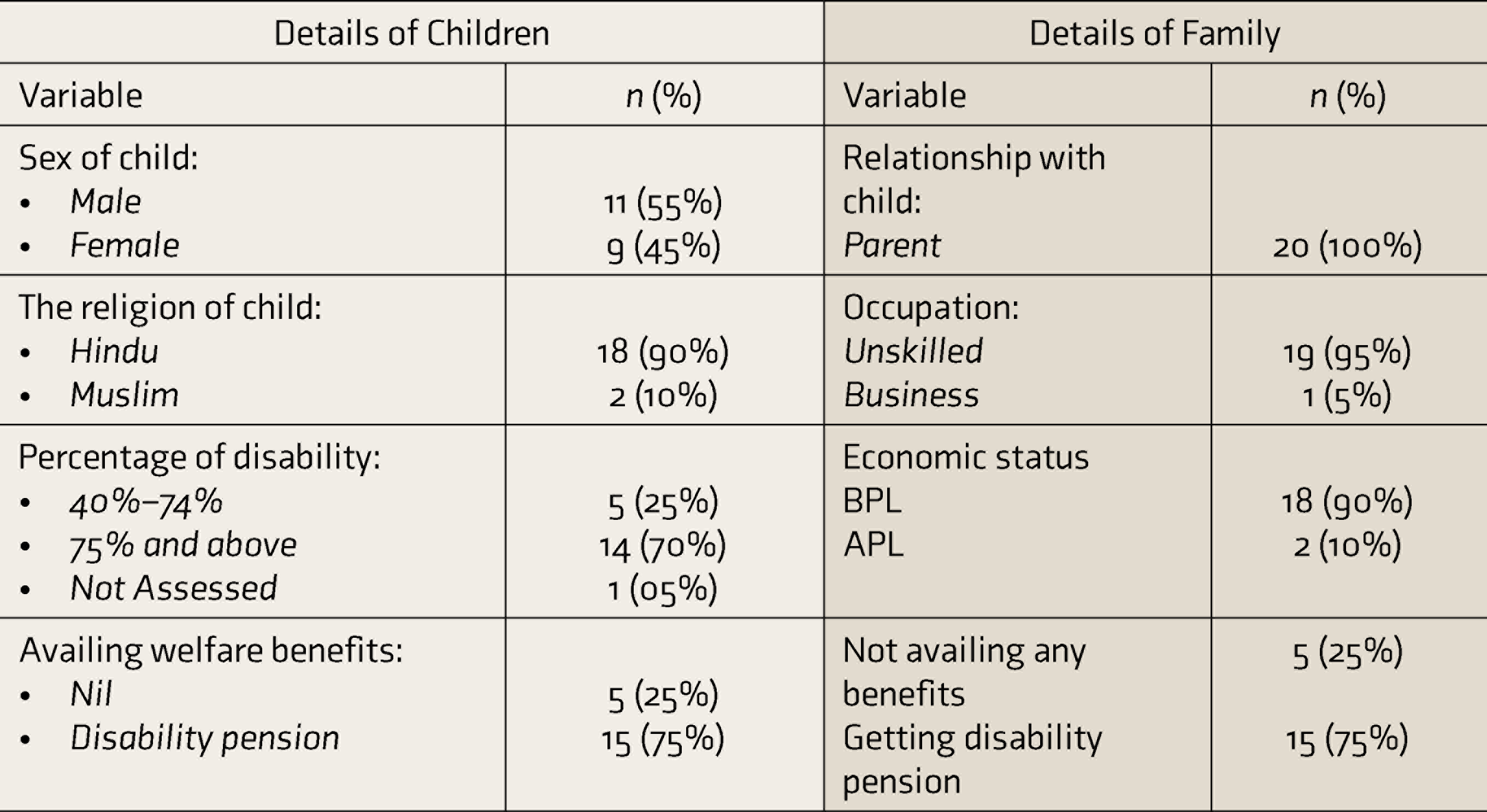
BPL: below poverty line, APL: above poverty line; IDD: intellectual and developmental disorders.
Situational Analysis of the Families of Children Individuals With IDD and Their Needs and Barriers in Accessing the Social Welfare Benefits
The “needs of the families of children with IDD” were as follows: (a) provision for special schools; (b) provision for daycare centers; and (c) facilitation of social security schemes for housing, pension, and medications (Table 3).The “barriers encountered by families in accessing social welfare benefits” included (a) lack of awareness about the types of schemes and process of procuring the benefits; (b) lack of availability of health and welfare services; (c) red-tapism and bureaucratic hurdles; (d) logistic problems to procure benefits; (e) stigma of revealing the disability of their child; and (f) high position in the society (Table 4).
Needs of Families of Children With IDD
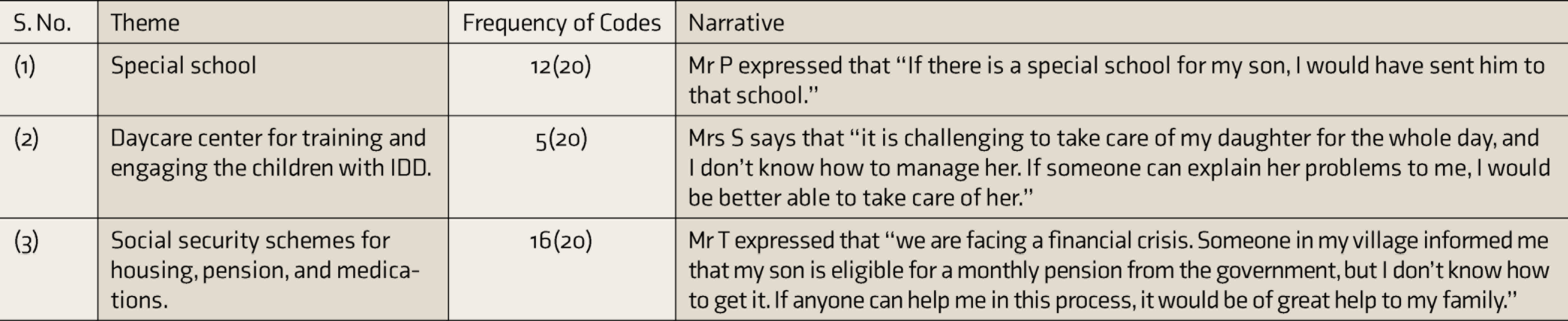
IDD: intellectual and developmental disorders.
Barriers Encountered by Families of Children With IDD in Accessing Social Welfare Benefits
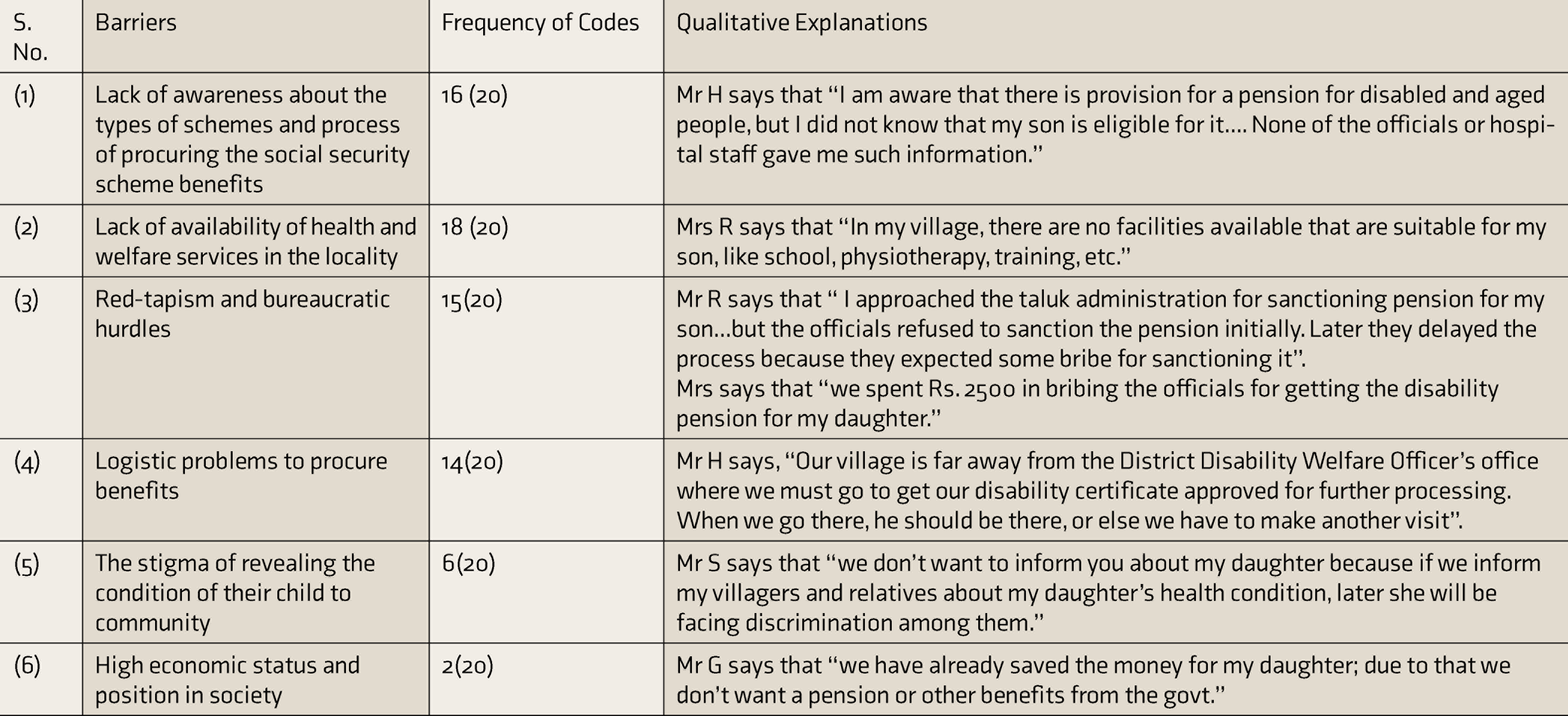
IDD: intellectual and developmental disorders.
Situation Analysis of NGOs
Various NGOs were approached to collaborate with the tertiary care hospital (NIMHANS) in fulfilling the needs of the families of persons with IDD. The first two NGOs that were approached were aware of the plan to start a special school in Konandur taluk and were willing to support this and the hospital’s other initiatives for the families of persons with IDD. However, they expected NIMHANS to provide technical support and training to their staff in providing services to address the needs of the families of persons with IDD; especially starting a special school/daycare services for persons with IDD. The process of applying for permission and finances under the National Trust Act 1999 was found to be very tedious. Furthermore, the NGO seemed unprepared in the context of human resources and finances to start the school in Konandur panchayath with its own resources and hence refused to continue partnering in this initiative. A third NGO from Bengaluru (urban area) that approached for this initiative was ready to begin implementing the program in collaboration with the tertiary care center (NIMHANS). However, as they had not run a special school for 3 years in a rural area, they did not fulfill the National Trust criteria and could not partner in this initiative.
Situation Analysis of the Community
The discussions held with the local leaders, including the headmasters of the government schools of Konandur, local doctors, merchants, and gram panchayath officials, brought out the fact that they were willing to support NIMHANS initiative to cater to the needs of families of persons with IDD; the foremost being starting of a special school in Konandur taluk. Out of the three government-run schools in Konandur panchayath that were approached by the NIMHANS team, the headmaster of one of the schools was supportive of providing infrastructure (one room) within the regular school for running the special school for children with IDD. Permission for the same was obtained from the Block Education Officer and Deputy Director of Public Instruction, who were the administrative heads for getting permission. The local officials responsible for facilitating social welfare benefits agreed to help families of children with IDD acquire monthly pension, construct subsidized homes (Ashraya Scheme), and provide free medications from the panchayath disability fund.
The barriers in accessing social welfare benefits as mentioned by the officials included: (a) lack of awareness about welfare schemes for children with IDD; (b) lack of demand from the families in procuring the social welfare benefits due to lack of awareness; and (c) lack of social audit to check if the welfare benefits have been provided rightfully to needy families with children with IDD.
As an outcome of the situation analysis, an awareness program was conducted at Konandur PHC to educate the caregivers of IDD children and all concerned stakeholders about the benefits available to them through the National Trust Act. Seventy-five members, including family members and local stakeholders, attended the program. Details about the local benefits available to persons with a disability, such as bus pass, train concessions, wheelchair, and education, were explained. The details regarding the process of enrolment in the Nirmaya Health Insurance Scheme under the National Trust was also given. This program helped to bring all the stakeholders together on one platform to help agree on implementing social welfare programs for families of children with IDD in the community.
Discussion
The current study helped in identifying 20 children with IDD in the area, assessing their needs and barriers, and liaising with community stakeholders. The main needs of the family members were to start a special school, daycare center, or training center and the provision of welfare benefits. Vocational and engagement-related needs were the main needs of families with children with IDD, apart from managing the user’s sexual needs and the costs for managing children with IDD, as observed in other studies. 11 The barriers included the lack of availability of health and welfare services in the locality. This could be mainly attributed to the fact that despite Karnataka implementing the District Mental Health Program (DMHP) successfully in 30 districts, the money allocated for mental health, especially rehabilitation services, is very little. Due to the outcome of this study, we were able to lobby with the Department of Health and Family Welfare, Government of Karnataka, to appoint ten psychiatric social workers at the Taluk level. These Psychiatric Social Workers were trained in providing rehabilitation services and welfare benefits to the clients and family as part of a collaborative project of Karnataka state holistic empowering program for mental ailments (KSHEMA) funded by Government of Karnataka under the National Health Mission.
Family-related barriers, such as logistic problems in procuring benefits, were also observed, as some of the caregivers were staying far away from the PHC 12 that provided health services. Accessing these health services was also seen as a stigma13—that such acts could affect their high position in the society.
As the National Trust Act 1999 does not permit government organizations to register to seek funds for implementing its schemes, NIMHANS as a tertiary care hospital sought the collaboration of NGOs to help implement the National Trust schemes in the rural area. In this collaboration, the role of NIMHANS would be to provide technical support and training of grassroots level staff in implementing the social welfare schemes in the rural area. Furthermore, with the appointment of the taluk-level psychiatric social workers under the KSHEMA project of the Government of Karnataka with NIMHANS, we plan to train the social workers to conduct home visits and provide Care at Doorstep services to those who find it difficult to reach a PHC due to logistic issues or stigma.
The lessons learned from this situational analysis was that facilitation of social welfare benefits requires a case management approach, as each family’s needs are different. This is time consuming, mainly because the social worker needs to first educate the families about the available social welfare benefits and, next, empower them to access these benefits. In this process, networking and partnering with key stakeholders, especially local officials, is essential for the success of this course of action. Unfortunately, the researchers observed that the caregivers in the project area were not aware of their rights and hence did not create any pressure group to advocate for provision of social welfare benefits. Due to the lack of awareness and pressure groups, the local administrators, too, had not taken any initiative in facilitating the social welfare benefits for the needy families.
The limitations of this study were that it was conducted only in one panchayath of Thirthalli taluk of Karnataka, which was a rural and lower socioeconomic status area. The needs of families with children with IDD could vary according to the services available in their area and their economic background, for example, there could be different needs and barriers in cities compared to rural areas, based on the socioeconomic status of the population. Future multicentric studies in different taluks from different socioeconomic backgrounds could give us an idea of the overall needs and barriers faced by families of persons with IDD, for better generalizability.
The situation analysis also brought forth the difficulties of implementing the National Trust schemes in rural areas, where the need is high. The National Trust schemes were developed by the Government of India so that it would reach the needy ones—majority of them staying in rural areas of India. However, this study seems to depict that implementing the National Trust scheme in the rural areas could be incredibly challenging unless some of the rules are relaxed for funding these schemes. For example: (a) The National Trust stipulates that to run a special school, the recruited teachers should have a qualification in special education that is recognized by the Rehabilitation Council of India. However, the National Trust does not provide a competitive salary for these teachers, who prefer working in urban areas for logistic reasons. Furthermore, those teachers who are ready to work in rural areas are not provided with any additional allowance as encouragement. (b) If an NGO did not have experience running a special school, it is not eligible to apply for grants under the National Trust schemes. However, this rule is like the chicken and egg problem where without financial support, the NGO cannot run the school; without a pre-existing school, the NGO cannot get grants. National Trust schemes should provide incentives, not administrative hurdles, to NGOs willing to start services in rural areas. The above-mentioned practical problems are the bottlenecks for the low take-up of the program in the entire country. For example, in the Karnataka state where this situation analysis was conducted, only six programs funded by the Disha Scheme and two programs funded by the Vikas Schemes were found to be currently running. 3
Conclusions
The needs of families of children with IDD include engaging the child in special education, daycare center, and accessing social welfare benefits. The barriers to access these social welfare benefits in rural India include lack of awareness among the stakeholders, unavailability of health and welfare services, red-tapism, bureaucratic hurdles, logistic problems to procure benefits, and stigma. There is a strong need to empower families, sensitize local officials, and advocate for social policy change to bring about effective implementation and suitable modifications in the social welfare schemes, such as the National Trust schemes. This would help in broadening its reach to the unreached in rural India.
Footnotes
Acknowledgements
The authors acknowledge the Mane Manasa Fund, Dept. of Psychiatry, NIMHANS, and Dr Bino Thomas, Associate Professor of Department of Psychiatric Social Work, NIMHANS, for editorial guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was funded by Mane Manasa Fund, Dept of Psychiatry, NIMHANS, Bengaluru.