
Abstract
Background
Bipolar affective disorder (BPAD) is a chronic, episodic illness that can create problems and disruptions in the social, occupational, and family functioning of a client. Families are frequently most affected by their bipolar member and have a sense of helplessness to fix bipolar symptoms. The current study aimed to assess the effectiveness of Family-focused Nursing Interventions (FFNI) on functional improvement in the sample of symptomatic bipolar affective disorder clients.
Method
In this experimental study, 149 patients with BPAD were interviewed along with family members through the consecutive sampling technique from the inpatient ward. Varying block randomization was used to allocate the patients to the control and experimental groups. After obtaining ethical clearance, the study was registered under the Clinical trail registry India (CTRI). Baseline sociodemographic and clinical variables, and the functional levels, were assessed using Longitudinal Interval Follow-up Evaluation-Range of Impaired Functioning Tool and Functional Assessment Short Test. The control group (74) received routine treatment; the experimental group (75) received routine treatment along with FFNI in seven sessions, and posttest was conducted at discharge, one-month, and at two-month follow-up at OPD. The collected data were analyzed using SPSS 20 (IBM Corp. Released 2011. IBM SPSS Statistics for Windows Version 20.0, Armonk, NY: IBM Corp.), independent sample t-test, analysis of variance, and Pearson correlation used. A P-value of less than 0.05 was considered as a statistically significant result.
Results
At the end of the study, 149 clients completed the treatment and follow-up. Both the groups were comparable at baseline in demography as well as clinical variables. There was significant improvement in the functional level after FFNI. The total score of LIFE-RIFT and the Functional Assessment Short Test score were significantly lower in the experimental group than the control group with P = 0.001.
Conclusion
The current study concluded that adjuvant to routine treatment FFNI will improve the functional ability of the client along with routine psychiatric treatment for BPAD.
Nurses play a vital role in connecting patients families and therapeutic team in planning treatment. Indian setting nursing led clinics and intervention are novel one. FFNI is one of its kind of intervention for the improvement of functional level of bipolar clients.Key Message
Bipolar affective disorder (BPAD) is a common serious mental disorder affecting approximately 1% to 2% of the total adult population in the world. 1 It begins in early adulthood in all societies at about the same rate, regardless of color, class, religion, or culture. 2
BPAD causes substantial psychosocial morbidity that frequently affects the patient’s marriage, children, occupation, and other aspects of life. 3 It exacts a heavy toll on the economy and time, and the quality of life as well as functioning, and it increases morbidity, comorbidity, and mortality.2, 4 Unlike the earlier studies, recent studies point out a significant degree of psychosocial dysfunction even when the patients are euthymic.5, 6
The treatment success rate with mood stabilizers, antipsychotic medications, and psychosocial therapy can be as high as 60% 1 with appropriate drug treatment. Forty percent of the patients who recover will suffer relapses. 7 Psychosocial interventions such as cognitive behavior therapy, family focused therapy (FFT), and interpersonal and social rhythm therapy and group psychoeducation, in conjunction with medication, have been shown to improve outcomes in BPAD. 7
FFT is an individualized intervention that is developed to facilitate patient and family coping through planed personal visits, improving communication, and involving patients and family for patient care activities, support, and counseling. 7
Nurses play a unique role in inpatient care and patients’ family support by advocating between the health team and the patient’s family. Long-term episodic illnesses like BPAD need home monitoring and care by family members. Miklowitz et al.8–10 have pioneered family-focused psychoeducational treatments for BPAD.
Family-focused nursing intervention (FFNI) is a method that respects the pivotal role of the family.11, 12 In FFNI, nurses’ foremost duty is to address family emotions and prepare them for FFT, which is a powerful tool for fostering stability within the family unit by involving them in inpatient care and educating them about the role of life events in the patient’s illness and how communication can improve the patient’s condition. 13
An international study conducted in patients with BPAD across different mood states highlighted the importance and need to develop psychosocial interventions targeting functional improvement. 14 Furthermore, a study conducted in Germany, Austria, and Switzerland found that only less than 2% of family members received psychoeducation. 15 Data regarding psychosocial interventions for BPAD patients’ functional improvement is very scanty in India. Keeping the vital role of the nurse in the inpatient care, the importance of the family in the long-term follow-up, and the dearth of studies on nurse-led psychosocial intervention at tertiary care hospitals, we felt the need for researching this area.
Objectives and Hypothesis
This study aimed to assess the effectiveness of FFNI on the functional improvement of bipolar clients at a tertiary care hospital. Research hypothesis was that there will be a significant difference in the improvement of the functional level of patients with BPAD between the experimental group and the control group.
Material and Method
This randomized controlled trial (RCT) study was conducted in psychiatric wards at a tertiary care center in South India. Data collection was done from November 2015 to July 2018. The research study proposal was approved by the Institute Scientific Advisory Committee. Ethical clearance was accorded by the Institute Ethics Committee (JIP/IEC/2015/19/699). The study was registered under CTRI- (CTRI/2017/09/009860 retrospectively).
Patients admitted to the adult psychiatric wards were assessed for eligibility on their first day of admission and then enrolled for the study. Adequate information about the study was provided in oral and written format in a vernacular language. Participants signed (after acute phase management) the written informed consent. One of the family members also signed the legally authorized representative (LAR) consent, since the study involved vulnerable psychiatric clients, after being explained about the risk and benefits of the study. Confidentiality and anonymity were maintained during and after the study
Sample Size
The sample size was estimated using the statistical formula for comparing two means with equal standard deviations at a 5% level of significance and 80% power (N = 2 × (1.96 + 0.845)/1.6) 2 × 3.2 2 = 63). A previous RCT 10 reported the mean difference Longitudinal Interval Follow-up Evaluation-Range of Impaired Functioning Tool (LIFE-RIFT) as 1.6 between the groups after the intensive psychosocial intervention. We considered this difference as the minimum expected difference for estimating the sample size for the present study. The expected difference in the mean level of functioning LIFE-RIFT between the groups was 1.6, with an standard deviation (SD) of 3.2. The estimated sample size was 63. The sample size was further modified, expecting a dropout of 20% during follow-up. Thus, the final sample size chosen was 75 in each group.
Inclusion Criteria
The patient has at least one primary caregiver (a blood relative or a person whom the patient stays with for more than a year) who is willing to participate and is interested in taking care of the patient.
The patient was diagnosed with BPAD as per International Classification of Diseases (ICD) 10 criteria and admitted to the adult psychiatric ward for treatment.
Patients enrolled for any other psychological therapy, such as family therapy and supportive therapy, were excluded. Primary caregivers with mental illness or cognitive impairment were excluded too.
Randomization Details
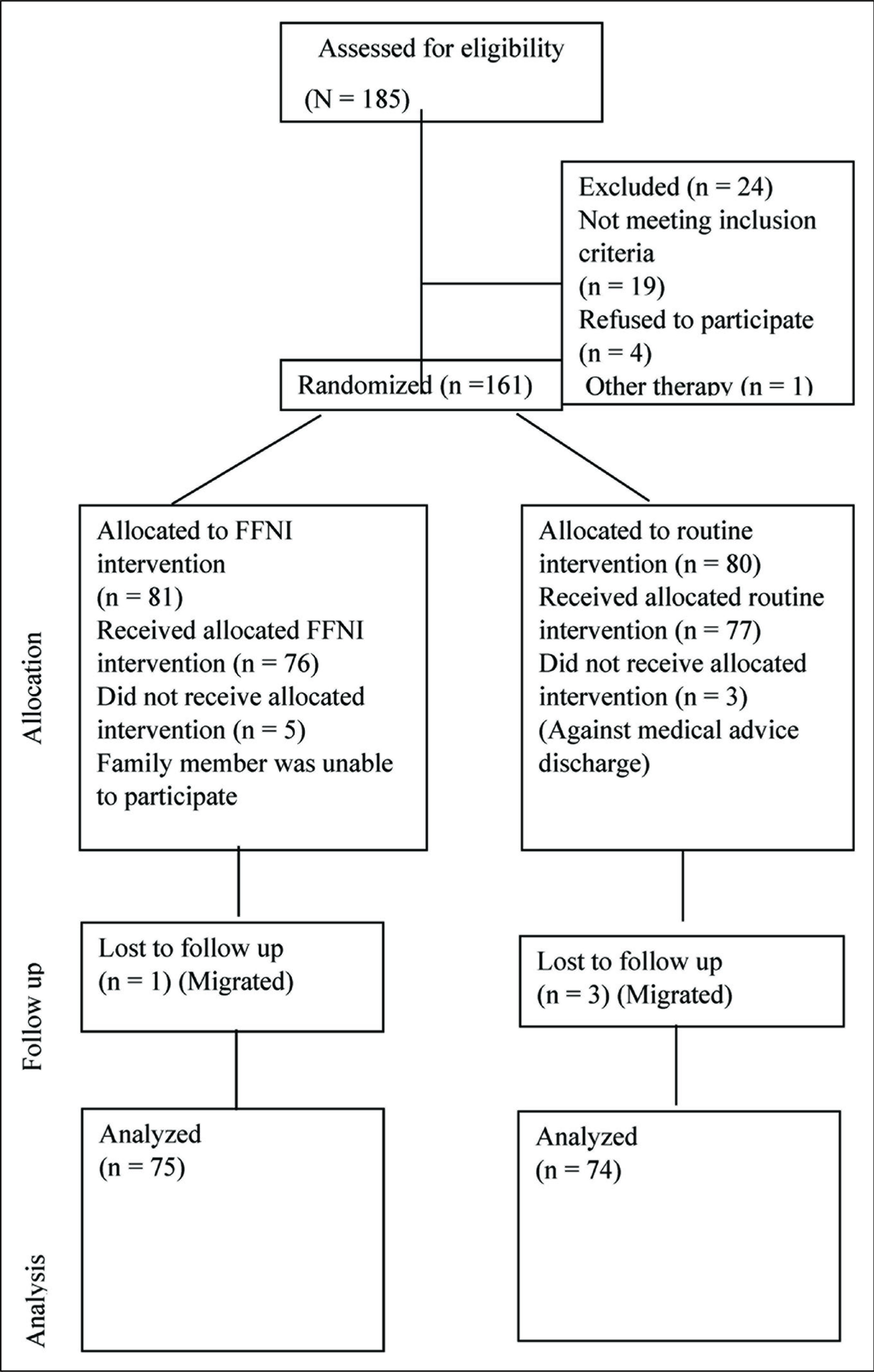
The patients were randomly assigned to the control group and experimental group using varying block randomization techniques. Using randomization software, 25 blocks were prepared. The randomization scheme consisted of a sequence of blocks such that each block contained a prespecified number of treatment assignments in random order (block consisted of 4, 6, and 8). Computer-prepared sequences were made by a statistician, and they were sealed in an opaque envelope. When the researchers received any patient in the ward, the covers were opened and the patient was allotted to each arm according to the group written on the cover. Eighty-one patients were randomized to the experimental group, and 80 to the control group.
Data Collection Tools and Methods
Patients and primary caregivers were interviewed to collect various demographic profiles. After collecting the demographic profile, a pretest assessment was done for patients using LIFE-RIFT 16 and Functional Assessment Short Test (FAST). 17
LIFE-RIFT had been validated previously on Indian samples14, 18, 19 of individuals with unipolar and bipolar disorder, with adequate internal consistency and interrater agreement. The internal consistency reliability of the scale was supported with alpha coefficients ranging from 0.81 to 0.83. The inter-rater reliability intraclass correlation coefficient (ICC) was 0.94. The predictive validity of the tool showed that impairment was positively associated with subsequent recurrence and negatively associated with subsequent recovery. A lower score indicates a better functional level. The cut-off for functional impairment is eight.
The validity and reliability of FAST were tested by the researchers using a pilot study. The pilot study was conducted among 45 BPAD patients. ICC was performed to assess test-retest reliability, and internal validity Cronbach’s alpha of FAST was 0.909. The test- retest reliability analysis showed a strong correlation between the two measures carried out one week apart (ICC = 0.98; P = 0.001). The higher the score, the more functional impairment the client has. The impairment cut-off for FAST was 12.
The control group received routine psychiatric treatment such as medicine and standard ward routines. The experimental group received FFNI in seven sessions, along with routine psychiatric treatment. FFNI was given to the patient and one of the family members who was the primary caregiver.
In initial sessions, only the family members participated. Patients were included after the acute phase management and when they were able to sit for the sessions, keeping in mind that psychoeducation should be delivered as soon as possible in the illness course, supporting the idea of early intervention. The researchers ensured that all FFNI sessions were attended by patients and family members in an individual session or a family session (Table 1). Separate session attendance was maintained to avoid overlapping of information and contamination of information. Strict instruction was given to patients and family members not to discuss the treatment with other patients, to avoid contamination.
FFNI Sessions Prepared and Administered by Researchers
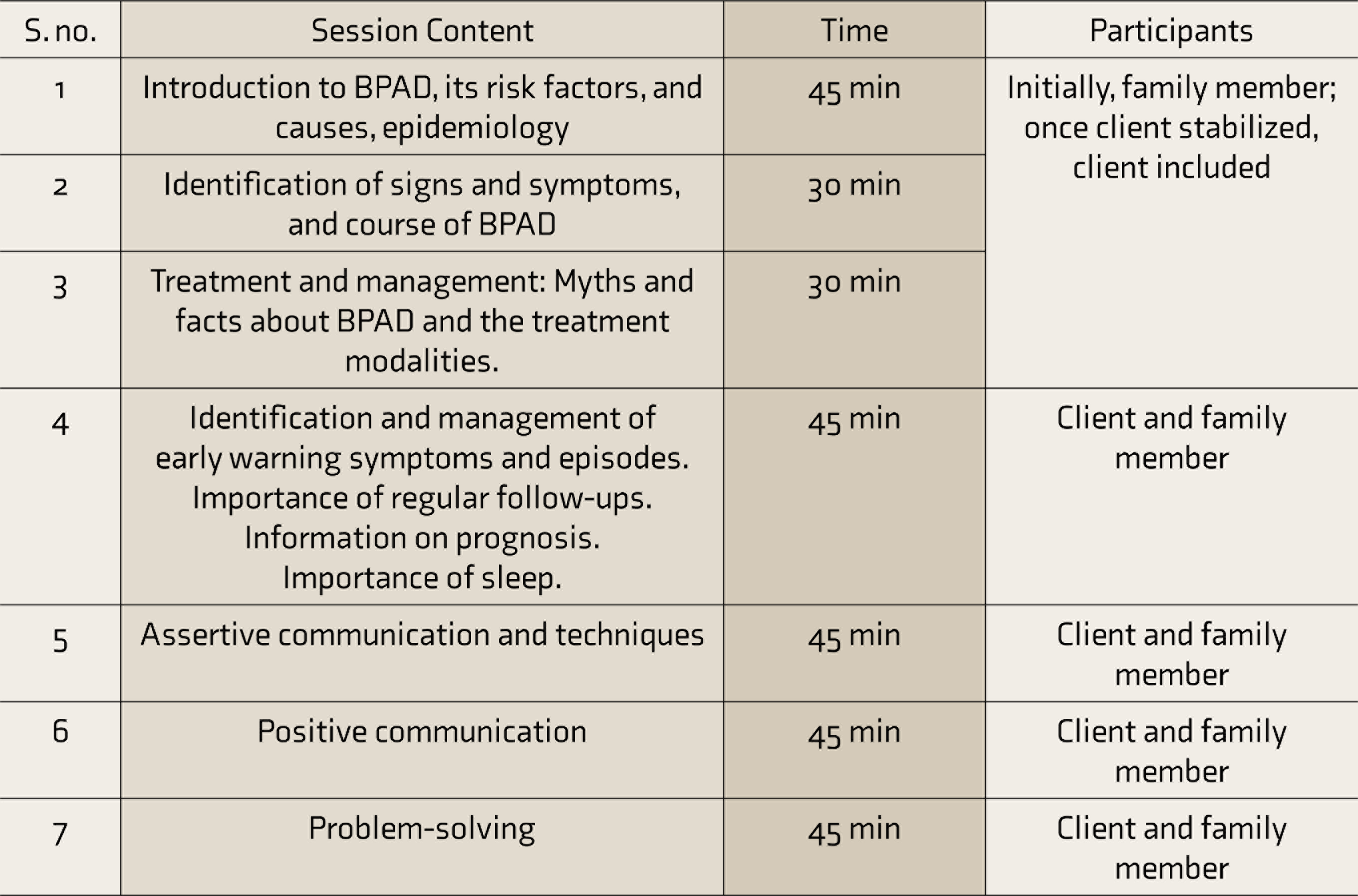
FFNI - Family-focused nursing intervention.
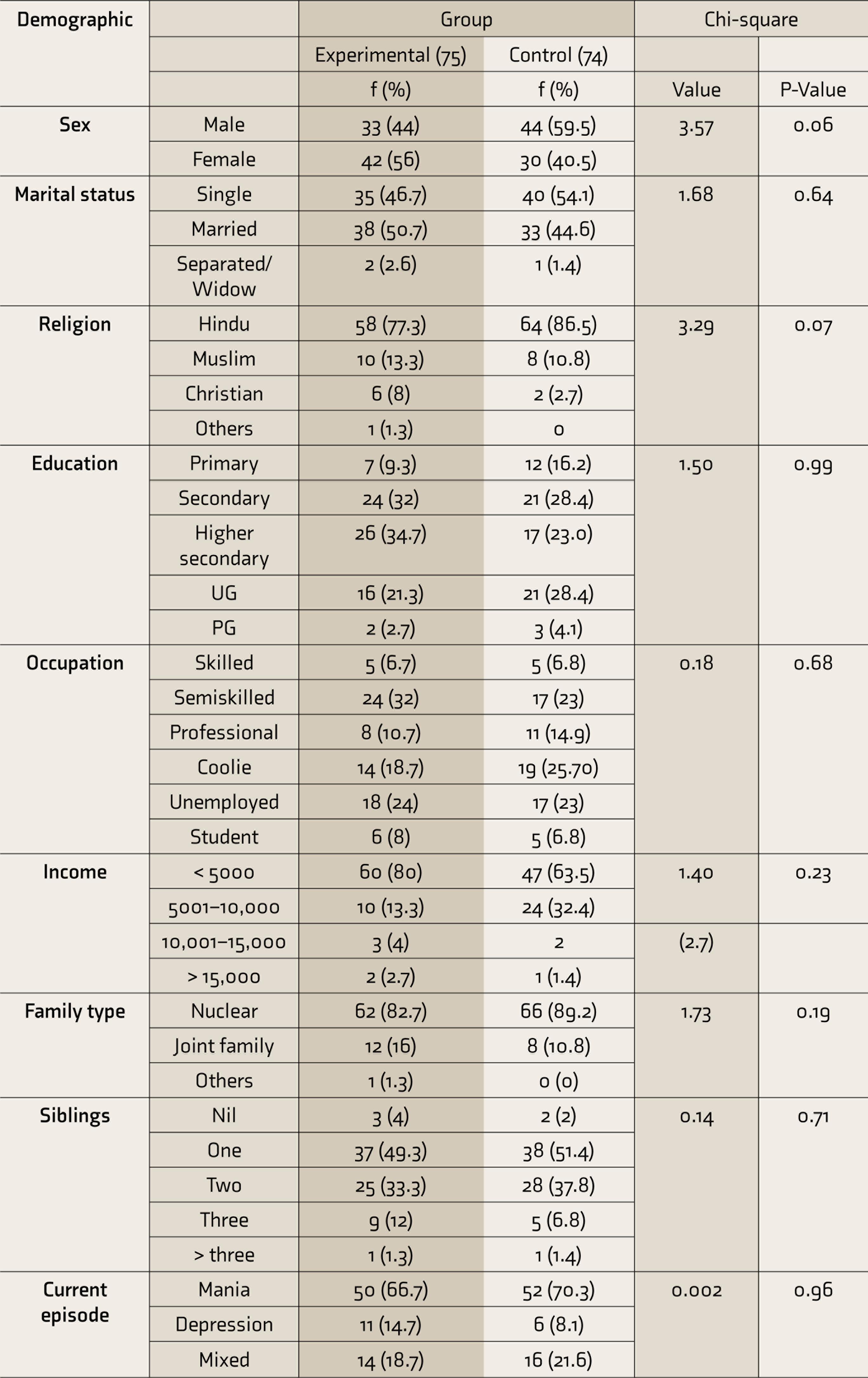
Group-wise Distribution of Demographic Profile of Patients (N = 149)
Posttest was done at three intervals for both the groups, using LIFE-RIFT and FAST. The first posttest was done at discharge from the inpatient ward, the second was done at a one-month follow-up at psychiatric Out Patient Department (OPD), and the third was done on the second-month follow-up at psychiatric OPD. During follow-up, from the experimental group, one left because of relocation, while in the control group, three were lost because of relocation.
Consort Flowchart
Development of Intervention
FFNI was prepared by the researchers based on their review of the previous literature, the client’s needs, family concerns, and standardized therapies for BPAD. FFT, Fallon model of family group education, Barcelona group psychoeducation program for BPAD by Colom and Vieta, and Rea et al.’s family- focused education are the standardized interventions for BPAD. After reviewing the aforementioned interventions, the researchers prepared a culture-specific FFNI for BPAD, based on the guidance, suggestions, and opinions of mental health experts. FFNI has been validated by the experts and by pilot testing. The final version had 100% consensuses between the experts. Experts were from the fields of nursing, psychology, social work, and psychiatry.
The tool and intervention package were translated into the local language Tamil and then translated back to English. Tamil validation was taken from Tamil literature teachers as well as from experts to ensure the standardization of the Tamil content before the ethical clearance. After the pilot testing, the protocol didn’t need any modification.
At the end of the study, group educational sessions were organized for the control group participants, and a booklet regarding BPAD was distributed as a part of study. Once the desired sample size was achieved, the trial was stopped for analysis.
Method of Data Analysis and Presentation
The distribution of categorical variables such as sex, clinical characteristics, treatment factors, etc. is expressed as frequency and percentage. The distribution of data on responses in the different items in the LIFE-RIFT scale and FAST scale are expressed as frequency and percentage. The Shapiro–Wilk test was used to check the normality. The changes in LIFE-RIFT score and FAST score in each group over time were carried out using one-way repeated measures of analysis of variance (ANOVA), and the changes over time between the groups were carried out using two-way repeated- measures ANOVA.
All statistical analyses were done using IBM SPSS 21 and were carried out at a 5% level of significance, and the P-value < 0.05 was considered significant.
Results
Out of 161 randomized patients, 149 were included for analysis after excluding dropouts. In the experimental and control groups, mean ages were 29.6 ± 8.4 and 31 ± 8.7, respectively, with the range of 17 to 58 and 18 to 58.
The clients’ illness days in the past year ranged from 0 to 90 in both groups. In terms of the total number of manic episodes in the past, the control group had zero to six episodes, while the experimental group had zero to eight episodes. Experimental group caregivers’ mean age in years was 47.5 ± 11, with a range of 18 to 69. The corresponding values for the control group were 50 ± 12 and 16 to 75.
Clinical Characteristics
A chi-square test was used to compare the baseline demographic details. Sixty in the experimental group (80%) and forty-five in the control group (60.8%) were not having any history of alcohol or smoking habits. This difference was statistically significant (P = 0.021). Thus, both the group participants’ habits were not comparable.
The majority in the experimental and control groups had 1 to 2 admissions: 26 (34.7%) and 28 (37.8%), respectively. In the experimental group, 12 (16%) and 7 (9.5%) in the control group were never admitted before to the hospital.
The total duration of illness in the experimental and control groups was 2 years to 5 years. In the experimental group, 14 (18.7%) had less than a year of illness, and in the control group, 7 (9.5%) had less than a year of illness.
In both groups, mania was the major subtype. In the experimental group, 50 (66.7 %) had mania, while in the control group, 52 (70.3%) had mania.
Except for the habit of drugs, none of the other variables such as number of previous admissions, current episode, number of previous episodes, duration of illness, or family history significantly varied between the groups.
Demographic Details of Caregivers
The majority of the caregivers were married. Concerning the occupation status, the majority in the experimental and control groups were semi-skilled: 42 (56%) and 32 (43.2%), respectively. In the experimental group, the majority had primary (34 [45.3%]) or secondary
(21 [28%]) education. In the control group, 47 (63.5%) had primary education.
The majority in both groups had parents as the primary caregiver. Variables such as caregivers’ sex, educational status, occupation, and relationship to the client were not statistically significantly different between the groups.
LIFE-RIFT and FAST scales showed that the baseline functional scores were comparable for the groups with P = 0.32 and 0.08, respectively. Both the groups had a noticeable functional deficit. This shows that patients with BPAD had poor overall functional levels and even poor domain-wise functional levels.
Functional Level After Intervention
The significant effect of FFNI on the functional improvement was seen as a decrease in the mean score from admission to the end of the study period. In the experimental group, employment scores (9.2–4.3), interpersonal scores (10.9–5.0), recreation scores (4.1–1.7), and satisfaction scores (4.17–1.71) showed a reduction. Employment score (9.2–5.2), interpersonal score (11.3–6.0), recreation score (4.2–2.2), and satisfaction score (4.2–2.2) of the control group also followed the same pattern, but the decrease in the mean score in the experimental group was much lower.
Repeated measures ANOVA was used to assess the functional improvement at the domain level between the control group and experimental group, which was significant with P < 0.05 (F value: 240.3).
Based on the FAST scale, functional level domain wise in the experimental group mean score of autonomy (10.3–1.2), occupation (13.3–5), cognitive (12.6–2.4), finance (4.6–0.52), Interpersonal relationship (IPR) (14.5–2), and leisure (4.6–0.99) was lower from pretest to end of the study. In the control group also, a similar pattern existed for autonomy (10.4–2.3), occupation (13.5–6.3), cognitive (12.6–4.0), finance (4.8–1.1), IPR (14.8–3.6), and leisure (4.9–1.49). Repeated measures ANOVA was used for variation. It showed that the decrease in mean score was significantly lower in the experimental group than in the control group, with P < 0.001 (F value: 282.7). The domain-wise score was significantly lower in the experimental group than in the control group, with P < 0.001 in both scales.
The total score of LIFE-RIFT and the FAST score was significantly lower in the experimental group than the control group, from pretest to posttest.
Interaction Effect
In terms of LIFE-RIFT functional assessment (Figure 2), both groups had a significant reduction in the functional score, indicating significant improvement in the functional level, with P < 0.001.
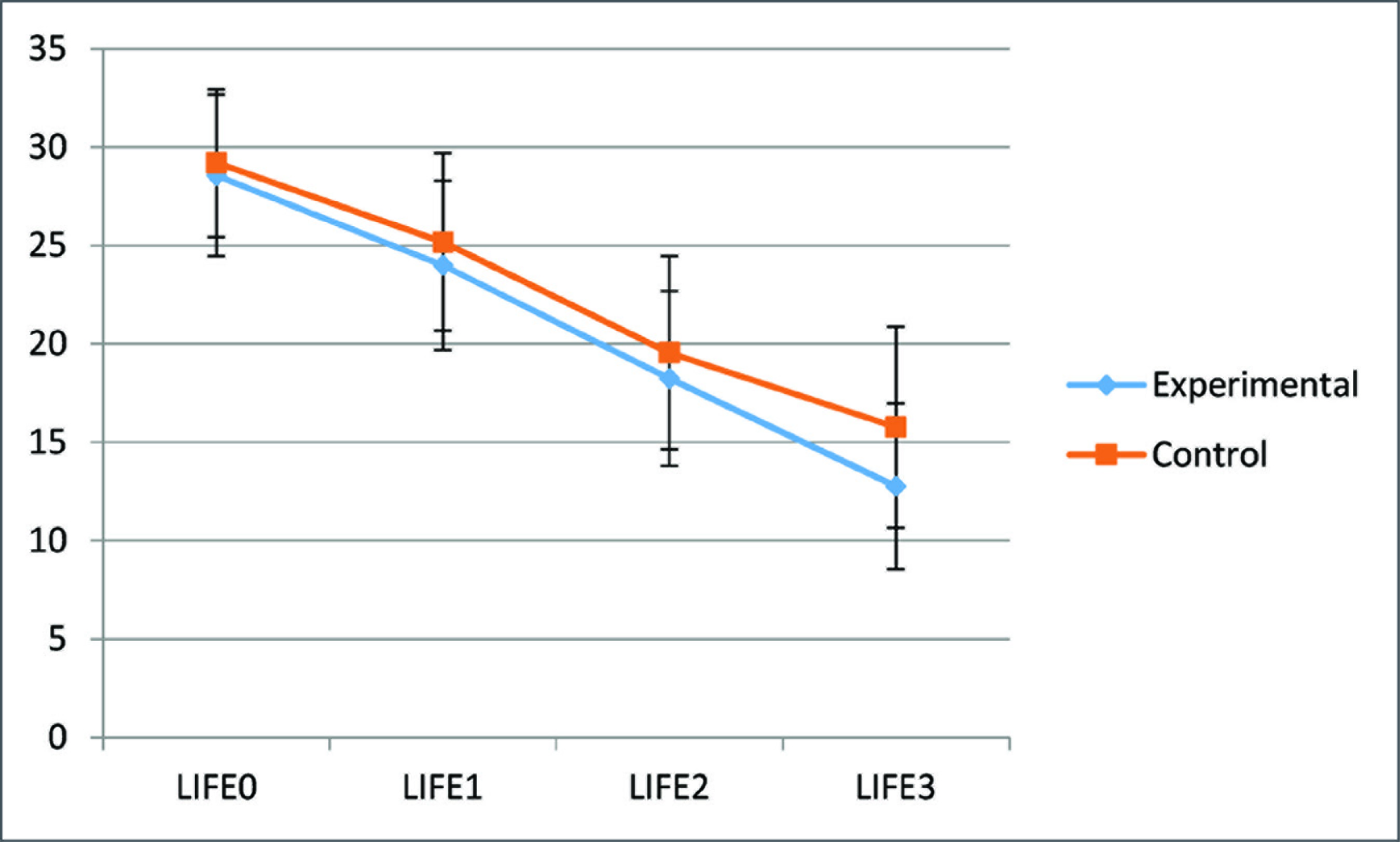
LIFE-RIFT - Longitudinal Interval Followup Evaluation-Range of Impaired Functioning Tool.
Even in terms of FAST, in the control group, the initial score was 61.43 ± 8.73, and the score at the end of the third month was 19.04 ± 11.42 (Figure 3), which was also a statistically significant reduction (P < 0.001). But, compared to the experimental group, the mean score of the control group was slightly high, which indicates that the experimental group had a better outcome.
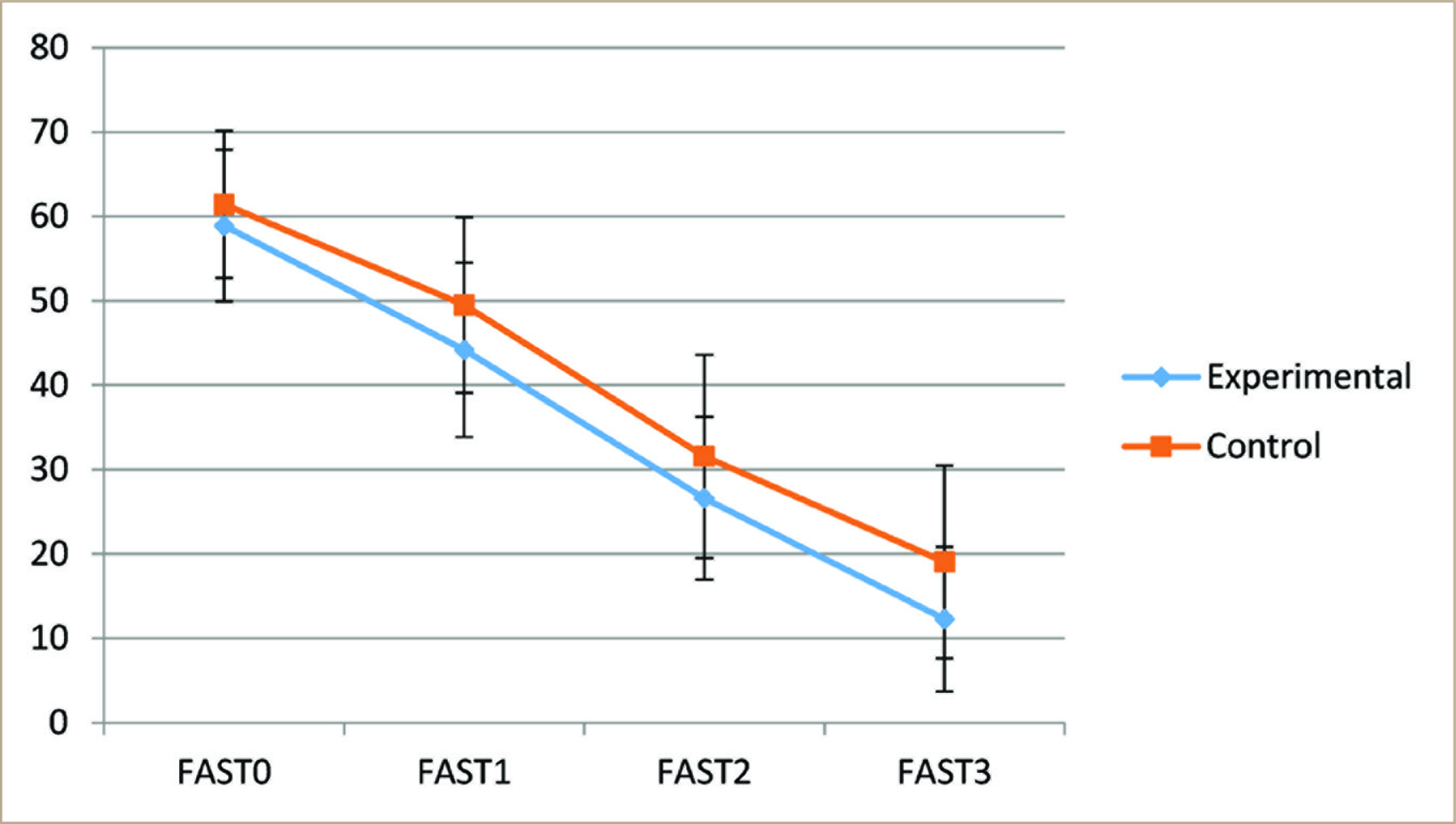
FAST - Functional Assessment Short Test.
The mean global functional score based on LIFE-RIFT was 28.56, 23.99, 18.24, and 12.77 at pretest, posttest one, posttest two, and posttest three, respectively (Figure 2). One-way ANOVA repeated test has been applied to compare the earlier given four mean values. Similarly, the mean global functional score based on LIFE-RIFT was 29.2, 25.8, 19.55, 19.55, and 15.77 at pretest, posttest one, posttest two, and posttest three, respectively, for the control group. There were changes over time between the groups using two-way repeated-measures ANOVA. The significant P-value indicates the mean global functional scores have been different for the four assessments. The significant P-value indicates that the changes that occur between pretest, posttest one, posttest two, and posttest three are statistically different for the two groups. (F value 96.12 with P = 0.007).
Even with the FAST Scale assessment, the changes over time between the groups using two-way repeated measures ANOVA (Figure 3). The mean global functional score was found to be 58.91, 44.17, 26.60, and 12.28 at pretest, posttest one, posttest two, and posttest three, respectively, in the experimental group, and the mean score in control group was 61.43, 49.4, 31.55, and 19.04 at pretest, posttest one, posttest two, and posttest three, respectively.
The significant P-value indicates that the changes that occur between pretest, posttest one, posttest two, and posttest three are statistically different for the two groups (F value: 2.66, with P = 0.045).
The significant P-value of the comparisons between the two groups indicates that the increase in the mean score was statistically higher in the experimental group than in the control group.
Discussion
In the current study, the LIFE-RIFT scale and FAST brought out similar results at baseline and were comparable. After the FFNI, the patient’s functional level significantly improved. At the pretest level, the LIFE-RIFT score was high, indicating more impairment. At the end of the third month, the score was reduced. The FAST score was high at the start of the study, and at the end of the study, it was reduced. The control group received routine treatment. Even in the control group, reductions in the functional score were observed in both scales. The significant P-value of the comparisons between the two groups indicates that the decrease in the mean score was statistically higher in the experimental group than in the control group. Similarly, between-group, within-group changes from pretest to posttest at three intervals significantly varied each time between the group with P < 0.001. Using skill-based psychoeducation and involving the family in therapeutic intervention and medication improve the overall function and BPAD symptoms. 20
A large, randomized trial by Miklowitz et al.21, 22 indicated that FFT effectively improved the course of BPAD in multiple domains when used as an early intervention.
Even domain-wise score reduction was seen in the current study in both the groups significantly. Western studies reported that after the intensive intervention, interpersonal and life satisfaction functions had significant improvement.23, 24 But the US study 23 contradicted the current study findings that the intensive interventions had no role in work and role functions. Similarly, another study too brought out the same results. 25 Patients had better total functioning, relationship functioning, and life satisfaction scores over nine months. A systematic review on psychosocial outcomes on the functioning of BPAD patients concluded that combined therapies with psychoeducation improve symptoms and social-occupational functioning. 26
The current study showed improvement in global functioning as well as domain-wise functioning. Similarly, a nursing study conducted in Turkey that assessed the effect of psychoeducation on the functioning level of patients with BPAD got the same result (P < 0.05). 27
The experimental group had a better functional improvement. Self-management, communication, and problem-solving strategies have significantly improved after the family-focused psychosocial intervention. Hence the research hypothesis has been accepted. Our study also emphasizes that the family-focused intervention (FFI), along with routine psychiatric treatment, significantly improved the functional level of patients with BPAD.
Overall, nurse-led FFI to improve the functional level of patients with BPAD is an accepted intervention. In India, studies about psychosocial interventions for functional improvement in BPAD are scanty. Current study findings showed that medication intervention combined with psychoeducation, communication, and problem-solving is better than routine psychiatric treatment for BPAD patients’ functional improvement. None of the patients or families had any adverse/ advent events during the trial.
The study has some limitations. Since the study was conducted in a single center, contamination could not be avoided. Only three months follow-was done. Because of two follow-up assessments on an outpatient basis, attrition was unavoidable. FFNI was given in seven sessions during the inpatient stay, but, because of time factor, the patients had only three posttest evaluations in month interval for functional assessments.
Conclusion
Nurses can successfully implement FFI to patients and their families to reduce functional impairment. For the patient, to achieve a better role in society, it is important to have a fully functional level. Functional impairment has been noted not only in the acute period but also during remission. So, this nurse-led intervention can improve the functional level during the hospital stay that can continue even at home.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.