
Abstract
Background:
Cognitive training (CT) for illness-linked neuropsychological deficits has been attempted in psychiatric disorders and, more recently, in obsessive-compulsive disorder (OCD). However, studies are few and far between, with a limited understanding of factors contributing to efficacy. This article aims to provide a comprehensive critical review of studies employing CT in OCD.
Methods:
This systematic review follows the Preferred Reporting of Items for Systematic Review and Meta-Analyses Protocols. Empirical studies that used any form of CT/remediation in individuals with OCD were included.
Results:
Eight articles met the criteria for inclusion, of which five were randomized controlled trials, two were case series, and one was an open-label trial. The studies have predominantly demonstrated improved trained cognitive functions, with only two showing generalization to untrained domains like clinical symptoms and socio-occupational functioning.
Conclusion:
There are few controlled trials of CT in OCD, which limits conclusions of efficacy. Given the sparse research in the area, the review summarizes the current status of research and examines important methodological considerations that may inform future studies.
Keywords
Neuropsychological/cognitive deficits in obsessive-compulsive disorder (OCD) are significant, and multiple reviews and meta-analyses have established deficits in executive functions (response inhibition, cognitive flexibility, planning, and decision-making) and non-verbal memory.1–4. In OCD, neuropsychological deficits may persist despite clinical remission5,6 and may predict treatment outcomes.7–9 The neuropsychological findings are linked to the underlying pathophysiology involving the cortico-striatal-thalamo-cortical circuit10–12 that is posited to underpin the clinical symptoms of OCD.13–15 Studies linking functional outcomes with neuropsychological deficits in OCD are scarce. 16 However, research in other psychiatric disorders has established that neuropsychological deficits predict not only clinical outcomes like symptom reduction, remission, response to treatment, adherence to medication, and outcome in psychotherapy but also functional and vocational outcomes like the ability to acquire, retain, or relearn skills necessary for real-world functioning, such as forming relationships and undertaking employment.17–20 Since evidence-based treatments do not fully address neuropsychological deficits, several authors have called for the targeted treatment of cognition to improve functioning in psychiatric disorders. 20 This is particularly true of OCD, where functional impairments are common16,21,22 and only approximately half of all patients respond to pharmacotherapy or cognitive- behavioral therapy.1,23 This highlights the critical need for cognitive training (CT) to address neuropsychological deficits.
CT (also called cognitive remediation/retraining/neuropsychological rehabilitation in the context of brain injuries) 24 “uses specifically designed, behaviorally constrained cognitive or socio-affective learning events delivered in a scalable and reproducible manner to improve neural system operations potentially”. 25 CT uses mechanisms of neuroplasticity to restore optimal functioning or to compensate for cognitive deficits. 26 An additional premise in psychiatric disorders is that if dysfunctional brain circuits are etiological to the disorder, then restoring the circuits’ normal functioning through CT must reduce the symptoms. 25 CT has been applied across affective, psychotic, and addictive disorders to improve long-term functioning in daily life, including reintegration into work and social environments, with varying levels of success.27–37 A key criterion of the success of CT has been emphasized as generalization (or “broad transfer of training”) to untrained domains and distal outcomes, such as symptomatic improvement, community and social functioning, and quality of life. However, such success has not often been demonstrated in existing studies.38,39 While some research, particularly in schizophrenia, documents improvements in cognitive functions, underlying brain changes, and durability of improvements over follow-up, 37 many other studies have failed to find significant effects of CT. 40 It is likely that methodological considerations highlighted in large-scale reviews and evidence-based recommendations41–44 of CT may shed light on factors contributing to the success of CT.
CT has been scantily tried in OCD and understanding is lacking regarding how it affects clinical, neuropsychological, and functional improvements in OCD. In this context, we systematically review the research on CT in OCD and its efficacy in improving neuropsychological, clinical, and socio-occupational functioning.
Methods
Protocol Registration
A systematic review protocol was developed and registered within the International Prospective Register of Systematic Reviews (PROSPERO; registration number CRD42022378062).
This systematic review follows the Preferred Reporting Items for Systematic Review and Meta-analysis Protocols: PRISMA 2020. 45
Sources and Search Strategy
To find all published studies, time specifiers were not set. Figure 1 depicts the process by which the relevant articles were extracted. For this review, electronic databases including PubMed, ScienceDirect, ProQuest dissertations and theses, Google Scholar, Scopus, and The Cochrane Central Register of Controlled Trials (CENTRAL) were searched for keywords “neurocognitive,” “neuropsychological,” “cognitive” combined with “training,” “retraining,” “rehabilitation” as well as combinations with “psychiatric disorders;” “OCD,” “obsessions” or “compulsions;” “anxiety” and appropriate Boolean operators and wildcard symbols. Studies in English relevant to the focus of the review were included, tabulated, and critically reviewed by all authors.
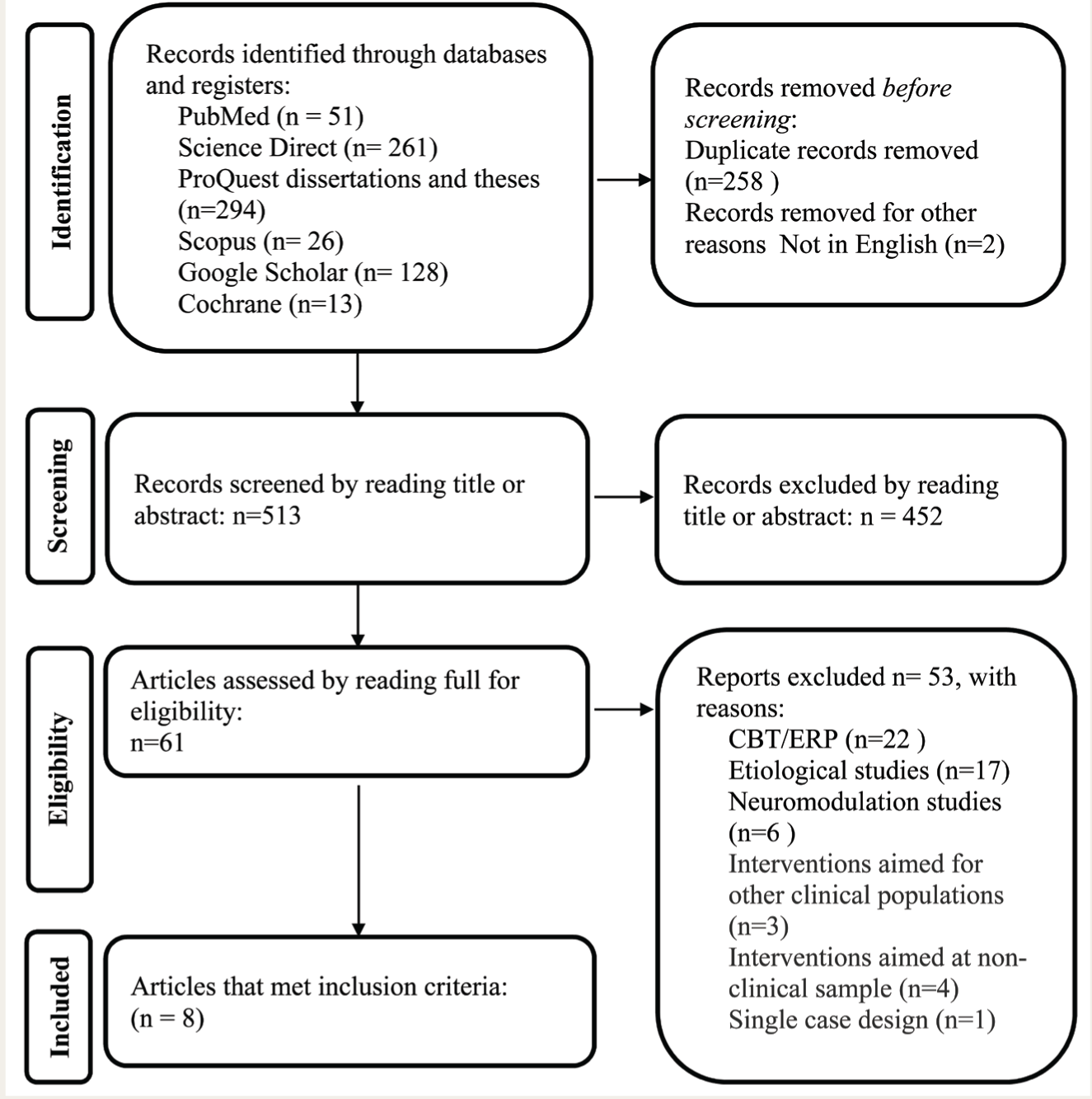
CBT-Cognitive Behaviour Therapy, ERP-Exposure and Response Prevention.
Eligibility Criteria and Selection Process
Studies were included if they (1) described any kind of CT, operationally defined for this review as any form of intervention that aims to maintain or improve a particular aspect of cognitive functioning (e.g., memory, attention, executive function) through guided practice carried out individually or in a group; 46 (3) used any computer- or non-computer-based tasks for cognitive stimulation; (3) included an intervention group of people with OCD (4) reported pre-post assessment of symptoms; and (4) were written in English. Studies excluded through manual review and filtering were (1) studies on interventions exclusively aimed at non-clinical samples; (2) studies on interventions aimed at other clinical conditions; (3) studies referring to cognitive behavior therapy and exposure-based techniques as they were clearly outside the scope of this review; (4) single-case studies; (5) studies reporting only neuromodulation techniques like transcranial direct stimulation and transcranial magnetic stimulation or neurofeedback methods; and (6) review articles, abstracts of conference proceedings, and editorials. Although standardized pre-post neuropsychological measures were important to assess outcomes, we did not exclude studies based on this because the transfer to distal outcomes (symptoms and real-world functioning) was of interest to this review.
Data Collection Process and Items
Two reviewers (first and second authors) independently selected articles based on the titles and abstracts. The reviewers then screened and reviewed the studies manually by reading the full texts to check the eligibility criteria. For the final articles, the following variables were collected: (1) type of study design; (2) sample size; (3) CT parameters: type of intervention/condition, training duration, frequency, and training tasks; (4) outcome measures, significant treatment effects; and (5) results.
Quality Assessment and Risk of Bias
The risk of bias assessment (also called study “quality assessment”) was done to establish transparency of evidence synthesis results and eliminate bias in the findings using a standardized quality rating tool. The Downs and Black 47 method provides a framework for assessing the quality of randomized and non-randomized trials. Hence, it was chosen to be an appropriate tool for assessing quality for the present review. The quality index used correlates highly with existing standardized appraisal tools for assessing randomized studies (r = 0.90) 47 and is highly ranked for use in systematic reviews. 48 The quality rating checklist included the following areas: (1) reporting, (2) external validity, (3) bias, (4) confounding variables, and (5) power. Out of a maximum score of 27, quality is classified as excellent (score 23–27), good (19–22), fair (14–18), and poor (<14). Quality was assessed independently by the first two authors; any discrepancy in rating was discussed amongst all authors to achieve consensus and agree on a score.
Results
Selection of Studies
We found a total of 773 studies via database search (Figure 1). After removing duplicates and reading the abstract or full text, eight articles met the inclusion criteria. Given the small number of studies, we decided to retain the case series.
Quality Assessment and Risk of Bias
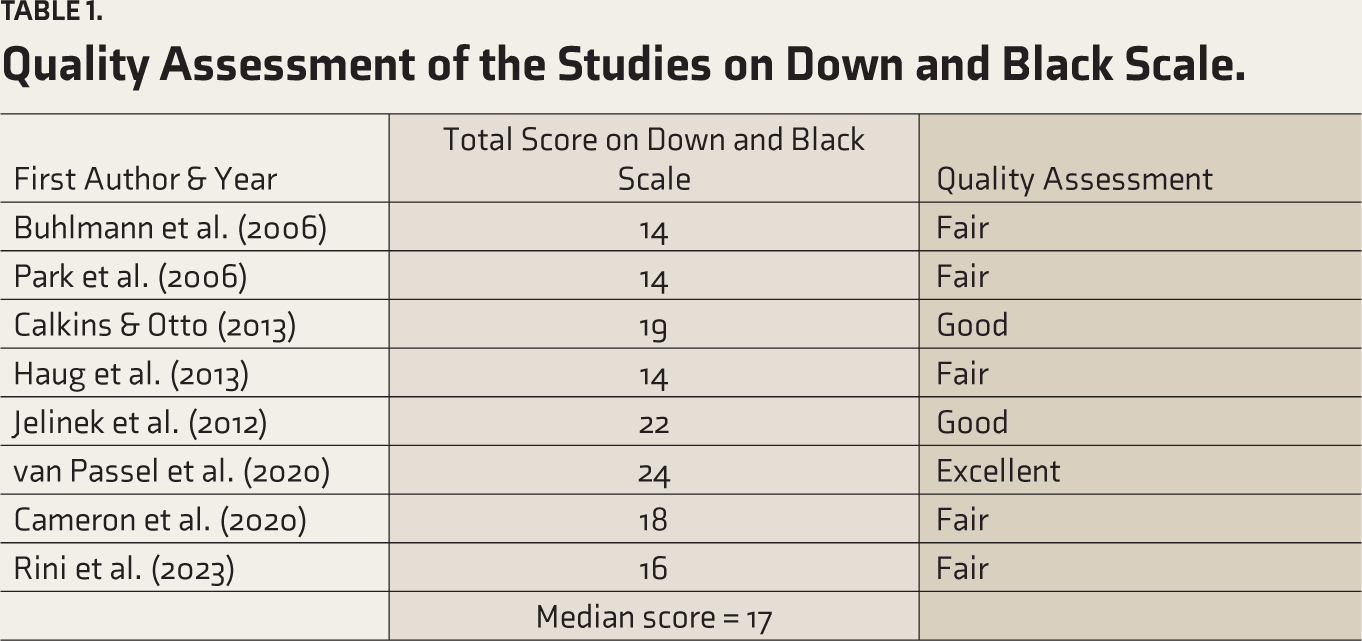
While quality rating was useful in an overall evaluation of the literature, it was not used as an exclusion criterion. Table 1 shows that in terms of quality rating, 12.5% of the included papers were rated as excellent, 25% as good, and 62.5% as fair. No paper was rated as poor. The median quality score was 17, ranging from 11 to 24.
Quality Assessment of the Studies on Down and Black Scale.
Data Synthesis and Effect Measures
The data items were tabulated (Table 2). The included studies showed major clinical and methodological differences. Across the studies, the outcome measures and the statistics for calculating the intervention effect were heterogeneous. Therefore, a meta-analysis was not appropriate, 49 and we do not present a mean effect size across the studies.
Study Characteristics
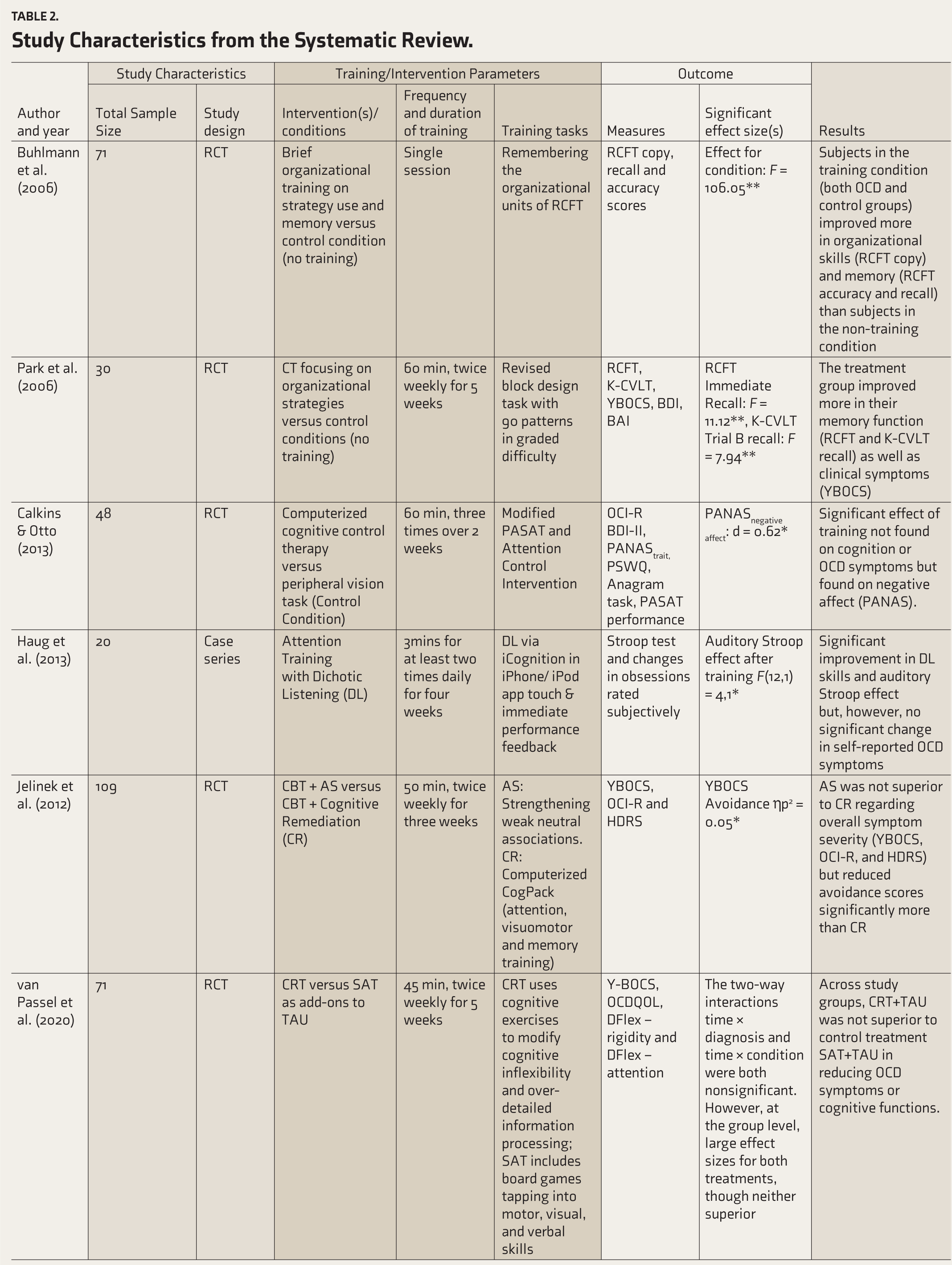
Table 2 summarizes the findings from the eight studies CT. Broadly, studies can be classified based on the approach 50 as (1) Drill & Practice/Restorative approaches that target cognitive deficits directly through repeated task practice, hierarchically organized task difficulty, and maintenance of high levels of accurate performance or (2) strategy-based/hybrid approaches, which, in addition to practice of complex tasks, may focus on training new efficient information-processing strategies; individualizing therapy to address deficits in motivation, metacognition, social cognition, and/or social skills, and aiding the transfer of cognitive gains to the real world.42,44,51,52 Five53–57 (Table 2), studies used predominantly drill-practice approaches and three used strategy-based/hybrid approaches.58–60 Five studies are randomized control trials (RCT),53–60 one is a two-group open-label trial, 58 and two are case series.55,59 Sample sizes ranged from 10 to 109, with four studies having less than 20 participants per group.55,57–59 Most studies were characterized by less than 10 h of total training,54,56,60 one even employed a single 45 min session, 53 and yet another, 6 min of daily training for 4 weeks. 55
Study Characteristics from the Systematic Review.
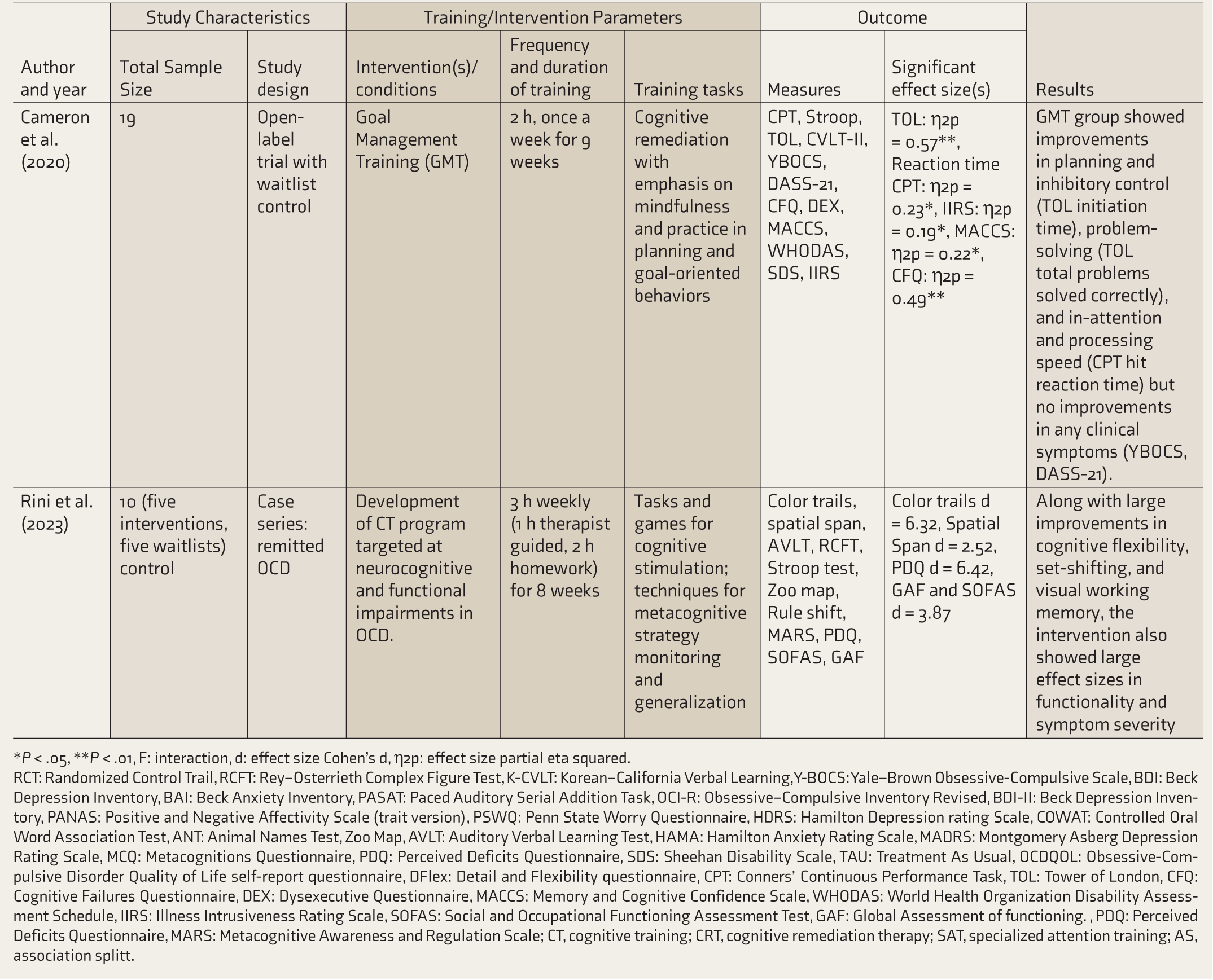
*P <.05, **P <.01, F: interaction, d: effect size Cohen’s d, η2p: effect size partial eta squared.
RCT: Randomized Control Trail, RCFT: Rey–Osterrieth Complex Figure Test, K-CVLT: Korean–California Verbal Learning, Y-BOCS: Yale–Brown Obsessive-Compulsive Scale, BDI: Beck Depression Inventory, BAI: Beck Anxiety Inventory, PASAT: Paced Auditory Serial Addition Task, OCI-R: Obsessive–Compulsive Inventory Revised, BDI-II: Beck Depression Inventory, PANAS: Positive and Negative Affectivity Scale (trait version), PSWQ: Penn State Worry Questionnaire, HDRS: Hamilton Depression rating Scale, COWAT: Controlled Oral Word Association Test, ANT: Animal Names Test, Zoo Map, AVLT: Auditory Verbal Learning Test, HAMA: Hamilton Anxiety Rating Scale, MADRS: Montgomery Asberg Depression Rating Scale, MCQ: Metacognitions Questionnaire, PDQ: Perceived Deficits Questionnaire, SDS: Sheehan Disability Scale, TAU: Treatment As Usual, OCDQOL: Obsessive-Compulsive Disorder Quality of Life self-report questionnaire, DFlex: Detail and Flexibility questionnaire, CPT: Conners’ Continuous Performance Task, TOL: Tower of London, CFQ: Cognitive Failures Questionnaire, DEX: Dysexecutive Questionnaire, MACCS: Memory and Cognitive Confidence Scale, WHODAS: World Health Organization Disability Assessment Schedule, IIRS: Illness Intrusiveness Rating Scale, SOFAS: Social and Occupational Functioning Assessment Test, GAF: Global Assessment of functioning., PDQ: Perceived Deficits Questionnaire, MARS: Metacognitive Awareness and Regulation Scale; CT, cognitive training; CRT, cognitive remediation therapy; SAT, specialized attention training; AS, association splitt.
Five studies reported improvement in the trained cognitive domains.53,55,57–59 Improvement in untrained domains and/or symptom reduction was evident in four,54,56,57,59 and among these, two54,56 did not find any improvement in the trained cognitive domains but reported some clinical improvements. A large RCT, 60 which compared the effectiveness of Cognitive Remediation Therapy (CRT) with a control treatment called Specialized Attention Training (SAT), found that CRT was not superior to SAT in reducing clinical symptoms or cognitive deficits. Two studies found improvements in at least one clinical measure, albeit not traceable to cognitive changes. Calkins & Otto 54 failed to detect any direct effect on cognitive functions or on OCD symptoms. Still, an indirect effect was found in which the intervention was able to reduce symptoms of negative affect (depression and anxiety). An RCT 56 that compared cognitive remediation (CR) versus association splitting (AS) technique as an add-on to CBT did not find AS to be superior to CR in reducing symptom severity but found some reduction in avoidance scores. This study did not report neuropsychological outcome measures. Two studies57,59 demonstrated transfer of effect on untrained domains. The RCT using CT focussing on organizational strategies 57 with 60 min, twice weekly sessions for 5 weeks found improvement in trained domains of memory functions and in untrained domains in the form of reduction in OCD symptom severity. In a case series, 59 the intervention combining cognitive stimulation, metacognitive monitoring, and generalization techniques found improvements in cognitive control, memory, and socio-occupational functioning, with a simultaneous reduction in the severity of anxiety, depression, and obsessive-compulsive symptoms.
Discussion
The article aimed to systematically review and appraise the current evidence base regarding the utility and efficacy of CT interventions on cognitive, clinical, and socio-occupational outcomes in OCD. Only eight studies were identified, with the first published study dated 2006. The small number of studies may be related to early negative results.53,54 Three studies53,55,58 demonstrated the improvements in only the trained domain, not extending to untrained neuropsychological domains, clinical symptoms, or socio-occupational functioning. Although two other studies54,61 showed improvements in at least one clinical measure, the relationship to cognitive changes could not be established. Only two studies57,59 showed improvements in trained domains extending to other cognitive and clinical domains; however, both studies were limited by small samples. Overall, the review indicates that the evidence for the efficacy of CT in OCD is limited at this stage, partially owing to the heterogeneity of methods and outcomes, but highlights methodological considerations that may provide useful insights for future studies.
A review of the vast body of literature available for CT, in general, reveals that while several early models of CT used “graded stimulation,” that is, exercises presented in increasing difficulty, to achieve restoration of cognitive functions, 62 most of these techniques consistently showed lower generalization and transfer of training to everyday life. 50 Studies analyzing predictors of response highlighted that attention, motivation, and clinician expertise, along with the measures of “brain reserve,” are key determinants of positive treatment response. 50 Practice standard recommendations for training of executive functions and attention42,44 have strongly recommended using metacognitive strategy training (self-monitoring and self-regulation), training in formal problem-solving strategies, and their application to everyday situations to foster generalization to real-world tasks. Studies using such strategy training and integrated methods show stronger and more durable effects on overall functioning. Only three of the OCD studies reviewed here used strategy training,57–59, and two of them demonstrated generalization to untrained domains. Another study excluded from the systematic review because of its single case design 63 also used a combination of CT, metacognitive strategy monitoring, and generalization activities over a 12-week period, finding significant improvements in trained and untrained cognitive, socio-occupational, and clinical domains.
It has also been emphasized that process-specific training (learning that focuses on methods and strategies in variable contexts) may result in the broad transfer of training.64,65 It is noteworthy that incorporating techniques of mindfulness in CT may be one efficient way of enhancing the generalization/transfer of training to real life. Independent research has demonstrated that mindfulness enhances cognitive control 66 and may produce broad-level transfer to untrained tasks and domains. 64 Two of the reviewed studies58,59 used process-specific training integrated with mindfulness-based practices for strategy training and yielded positive results, thus indicating the potential of such training in treating OCD.
In terms of the training method, it is important to highlight the use of smartphones and gamified CT which has gained importance in recent times. Four of the reviewed studies have used technology-based interventions.54,55,59,61 Recent studies67,68 demonstrate that using gamified CT and smartphone-based training has benefits in conditions like traumatic brain injuries and dementia. In OCD, one study, 69 not employing CT, investigated the effects of novel smartphone interventions on cognitive flexibility and OCD symptoms in healthy individuals with OCD-like contamination fears and found high levels of adherence to the interventions and improvements in cognitive function and symptoms. Concerning the method of delivery, using technology-driven interventions has several advantages: they are easily available, interesting, and engaging and include objective methods of scoring that are self-explanatory and can also serve as a reinforcer for the participants.
Another important consideration may be the dose, duration, and frequency of training. A few existing guidelines comment on the necessary and sufficient timelines for CT. However, Lauenroth, 43 in an examination of the literature, recommended that 1–3 h of weekly training for 12–16 weeks (or more) is more likely to lead to detectable improvements in cognitive performance than other training schemes, with a minimum being 10 h of training. Dose effects may partly explain the lack of significant effects in most reviewed studies.53–56,60 Only three studies employed training equal to or more than the recommended 10 h,57–59 of which two demonstrated broad transfer of training. This finding emphasizes the need to consider duration and frequency factors carefully in future research.
The sample size was small in four of the studies,55,57–59 making it difficult to draw reliable and generalizable conclusions. The heterogeneity of the outcome measures used also warrants attention—most studies used a combination of neuropsychological assessments and clinical measures to report outcomes. Still, the type of neuropsychological test used to measure a particular function differed greatly across studies. Moreover, two studies60,61 using CT as an intervention did not report standardized neuropsychological outcome measures and used only clinical scales and self- report inventories as outcomes. Another question that could not be answered in the present review is of practice effects with repeat assessments. However, performance improvements due to practice are known to be pronounced with weekly or fortnightly testing in the initial phase and generally plateau beyond three months. 70 Only two studies reported assessments spaced more than 2 months apart.58,59
Only five of the reviewed studies used RCT designs.53,54,57,60,61 In intervention studies, controlled designs are crucial to rule out confounding factors, and RCTs contribute to the highest level of evidence. However, the problem of designing RCTs is nuanced, particularly in non-medical studies. For instance, the psychotherapy literature has long argued the definition of placebo, when the benefits of treatments and placebos both depend on psychological mechanisms. 71 This is echoed in the CT literature with the issue of control tasks and double-blinding 72 —in particular, identifying a “sugar pill” task which is face-valid yet inert when the very act of participating in an exercise may be cognitively stimulating. Such practice effects may have contributed to the lack of differences observed in the largest RCT reviewed, 60 in which active cognitive stimulation (using games of strategy) was common to both intervention and control groups. More research is needed to identify active and inert ingredients in CT interventions. For instance, task engagement and expectation have been underscored as moderators that remain to be understood. 25 Nevertheless, research in analog samples has demonstrated that the effects of CT are independent of participant expectations. 73
A distinct issue central to OCD neuropsychological research is the lack of agreement on the core deficit. Some studies conceptualized organizational impairment53,57 or cognitive inflexibility 60 as the core deficit or target of training. However, several recent metanalyses1,3 and reviews 74 highlight the inconsistency of neuropsychological findings in OCD. Thus, the target for CT in OCD remains poorly understood. It has been posited that neuropsychological deficits in OCD may be best explained as a broader difficulty with executive control of lower-order cognitive abilities or cognitive control,4,75 which is a transdiagnostic construct highlighted in the Research Domain Criteria framework. 76
Limitations of the Review Process
It is important to highlight the heterogeneity of the studies reviewed: the studies had designs ranging from case series to RCTs, used different CT methods, and had varied durations and frequencies ranging from a single session to 12 weeks of training. Concerning outcome measures, not all studies reported neuropsychological functions. The heterogeneity of existing studies precluded a quantitative meta-analytic review, which may be considered in the future.
Future Directions
Studies of CT in OCD are sparse, with small samples, short duration, limited controlled data, lack of follow-up assessments, and varied approaches to training. The field needs empirically designed and adequately powered RCTs that investigate the variability of treatment response; explain mediators, moderators, and hypothesized mechanisms of action; and help determine the duration and dosage of training needed for enduring changes in neuropsychological and real-world functioning in OCD. The engagement of participants may also be enhanced through training tasks that mimic the demands of real-life situations and are technology driven. Future studies must also examine the synergistic effects of combining CT with other interventions and techniques.
The quest for suitable study designs to control for confounding factors in non-medical studies is ongoing; meanwhile, clinical reports and open-label studies may be valuable in generating useful insights for further testing. However, there is also a need for redefining the problem and testing novel methods. Novel approaches may need to be driven translationally, extrapolating methods and techniques from cognitive psychology/cognitive neuroscience to clinical practice.
Conclusion
This review found eight studies related to CT in OCD. Most showed improvement only in the trained domain. However, a smaller fraction of uncontrolled studies demonstrated improvements extending to untrained domains. Methodological strengths and limitations of these studies have been highlighted, along with problems intrinsic to research design in CT and the scope of using novel integrated approaches, drawing from translational research and evidence-based recommendations in other disorders.
Supplemental Material
Supplemental material for this editorial is available online.
Footnotes
Author Contributions
MB: concept and design, data acquisition, data extraction, interpretation of data, preparation of manuscript; HK: concept and design, data acquisition, interpretation, editing, approval of final manuscript, YCJR: design, editing, interpretation of data and approval of final manuscript.
All authors have contributed to and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
MB is funded by The Accelerator Program for Discovery in Brain disorders using Stem cells (ADBS), Department of Biotechnology, Ministry of Science & Technology, Government of India. (BT/PR17316/MED/31/326/2015).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.