
Abstract
The COVID-19 pandemic and subsequent lockdown to mitigate the spread of the COVID-19 have resulted in social isolation, reduced social support system, and increased domestic violence (DV) cases against women and children. The governments and NGOs have taken several measures to prevent DV by starting helpline, WhatsApp numbers, and counseling services during the lockdown to safeguard the women. This paper describes a case scenario of how we offered tele-case work consultation during the lockdown period due to the COVID-19 pandemic, the procedure adopted, and preventive measures followed while providing a tailor-made psychosocial intervention to a DV survivor. It also discusses the strengths and challenges while offering tele-consultation and possible steps to overcome the technological barriers to mental health professionals.
The COVID-19 pandemic has affected about a billion people worldwide and has been recognized as one of the worst public health crises in a decade. 1 To prevent the spread of infection, most countries have adopted social distancing, quarantines measure, social isolation, travel restrictions, and stay-at-home orders that affected men and women differently. As a result, gender inequality and gender discrimination have intensified globally. 2 In fact, the Executive Director of the United Nations (UN) Women has described this as a “shadow pandemic.” 3 The national and global data revealed exponential spikes in domestic violence (DV) incidents during the pandemic.4,5 Analysis of the secondary data of phone calls to the helplines of DV at Peru 6 reported a 48% increase in the incidence rate of calls during the nationwide lockdown. The findings brought out an urgent need to frame policies to mitigate the impact of stay-at-home orders to combat COVID-19. Vieroa et al. 7 recommend the need for innovative measures to provide services for victims of violence during the COVID-19 pandemic.
Several countries initiated digitally-driven innovative strategies, such as separate WhatsApp numbers, 24×7 helpline services, online chat services with geolocation linking, and web-based digital resources, to help DV survivors during the COVID-19 pandemic.8,9 However, the novel digital modalities have specific strengths and challenges in mitigating the problem of women undergoing DV during the pandemic. Herewith, we are sharing a case scenario of how we offered tele-case work consultation during the national lockdown period due to the COVID-19 pandemic, the procedure adopted, and precautionary measures followed while providing psychosocial interventions to a DV survivor at “AWAKE” Special Clinic for Women with DV in National Institute of Mental Health and Neurosciences (NIMHANS), Centre for Well-Being, BTM layout, Bengaluru, Karnataka, India.
The clinic provides comprehensive and tailor-made psychological counselling for the victims and survivors of DV or intimate partner violence (IPV). At the individual level, the gender aspect of therapeutic counselling is done by addressing an array of issues such as self-blame, guilt, trauma, and much more. The aim is to empower them to adopt adequate strategies to handle the violence and protect themselves and their children. A range of services are provided, such as telephone counselling, trauma care, crisis intervention, referrals to free legal and shelter care, and supportive group psychotherapy to both prevent social isolation and enhance social support of women survivors of DV/IPV. The services are offered by faculty and consultants with expertise in mental health clinical services, women’s mental health, trauma care, and psychosocial intervention for survivors of gender-based violence (GBV).
Case Scenario
A 35-year-old married woman, residing in Bengaluru city, from a middle socioeconomic background, is the mother of a five-year-old girl and an eight-month-old toddler. She is a graduate in commerce but has been a homemaker post-marriage. She was referred by COVID-19 Mental Health Helpline during the national lockdown period to address psychological distress secondary to DV by her husband. The client reported that she was unable to sleep, feeling sad, unable to concentrate on day-to-day activities, and worried about the future of herself and her children as the husband stopped giving money to maintain the family. When the client was referred for tele-case work consultation from the COVID-19 Mental Health Helpline, psychological first aid was provided to handle the crisis (i.e., LIVES approach, which includes: listening, inquiring about the client’s needs and concerns, validating, enhancing safety, and support of client). Later, individual sessions were held by following the tele-psychiatric social work (PSW) practice guidelines of NIMHANS. 10 The guidelines were framed after reviewing several national and international guidelines on the use of technology to provide health services, including the Medical Council of India Guidelines, 2020, and Tele-Psychotherapy Guidelines, 2020, of NIMHANS. The use of technology tools in PSW practice is offered stand-alone or in conjunction with in-person PSW services. Contemporary PSWs can provide services to individual clients, groups, and communities by using online/ telephonic/video/self-guided web-based services. PSW practice using telecommunication technologies includes the use of email, text messaging, video conferencing, online chat, messaging, or internet phone. The following standards are provided for five main areas of PSW services: (a) working with individuals-case work management, (b) working with families, (c) working with groups, (d) crisis management, and (e) working with communities. Each practice standard provides general guidance on using technology tools ethically and maintaining the professional boundary. 10
Process of Tele-Case Work Consultation
First Consultation (Intake Session)
The client first called the COVID-19 Mental Health Helpline where the oral consent was obtained before referring to the tele-case work consultation at AWAKE Clinic. Later, written informed consent was obtained from the client through email. Session notes were maintained as per the tele-session recording format. 10 During the first intake session, the therapist assessed the suitability of the case for the tele-case work consultation, following the guidelines of NIMHANS. 10 The identity of the client was confirmed by verifying the government ID she sent by email. Subsequently, she was informed that sessions could not be recorded or used as evidence in the future. An assessment of the suitability of the case for tele-case work consultation was done by briefly evaluating the mental health status of the client by asking open-ended questions about her mood status (e.g., “could you tell me how you are feeling for the past one week?,” “How is your mood?,” “Have you thought of hurting yourself/your children?,” “Have you ever made a plan?,” etc.), sleep, appetite, day-to-day functioning, and any fear associated with the experiences of violence. Apart from this, information about any past history of mental illness and treatment history was collected. From the assessment, it was revealed that the client had no psychotic symptoms or depressive mood, and her biological functioning was within the normal conditions. She had worries about ongoing marital issues. The client had no psychiatric illness in the past.
During the intake session, it was brought out that around eight years ago, the client and her husband, a graduate working as an accountant at a private firm, had married of their own choice, without the consent or support from either of their families. Though they have been living as a couple, as per the client’s account, the husband had not informed his parents or other family members about the marriage, citing the caste differences. The client reported that she has been undergoing DV for the past six years from her husband in the form of physical, psychological, and sexual violence. The client reported that initially their marriage was going on well; however, she noticed at times that her husband used to control and abuse her in filthy language for no reasons. The client reported that she accepted his behavior, thought that it was part of his personality. He used to control the finances and never allowed her to interact with friends or neighbors in the locality. On several occasions, he demanded her to bring money from her parents and physically abused her. The client reports that things got worsened from the last six months where he would beat her and scold her using abusive language. He would ask her to leave the relationship forever so that he can marry another woman and take dowry from them. When the client questioned his intention and refused to give approval for the second marriage, he would become more psychologically and physically abusive—to the point that he even threatened to kill her and the children. The client reports that following the birth of the second child, he completely deprived her of physical relationship, saying she is no longer attractive as she gained weight following the delivery.
The current reason for seeking teleonsultation was, two months before, the client’s husband had married another woman without her knowledge. Following his second marriage, he would visit her once a week, abuse her physically, and threaten to leave her and their children if she complained about his second marriage to the police or informed their neighbors. He would send her threatening messages whenever she tried to reach out to him or threatened to leave her forever as she does not have any proof of their marriage. When the client called us, she was in psychological distress, which affected her decision-making capacity. The client could not visit the hospital for therapy sessions due to the lockdown. The client had not visited any hospital or agency before approaching us for tele-consultation.
Interventions: Goals
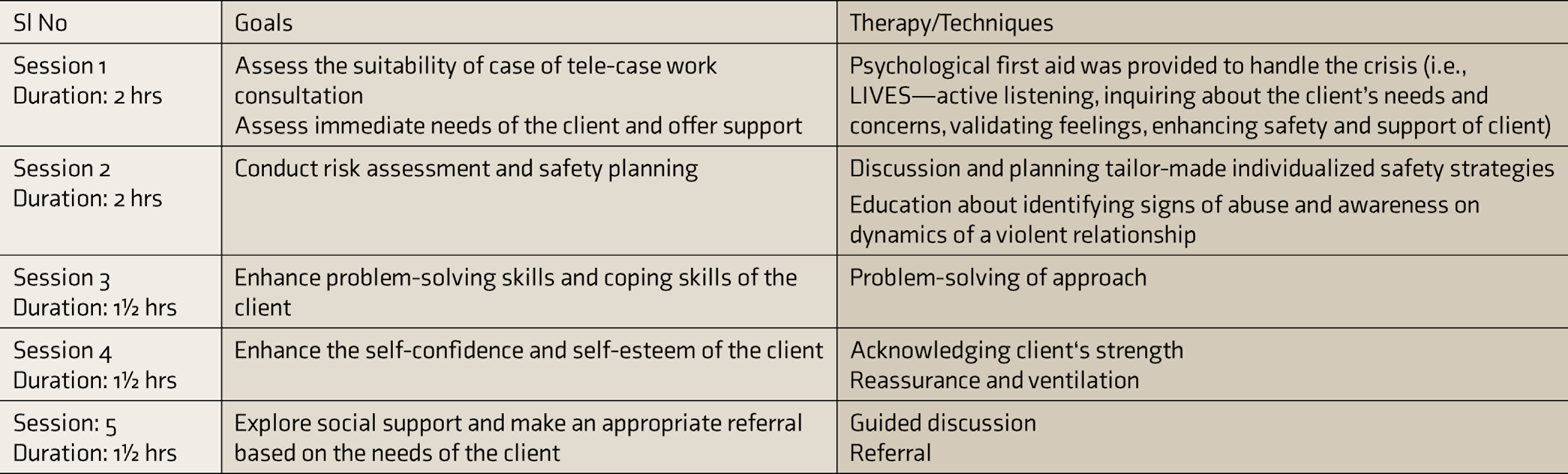
The short-term goals of the individual tele-counseling sessions were to assess the ongoing problems, immediate needs, and concerns of the client; offer the first line of emotional support; and enhance the safety of the client through risk assessment and safety planning. The long-term goal was to help the client deal with problems in an adaptive way using problem-solving and coping skills. Five individual sessions were held; each session lasted 1.5–2 hours. The sessions were conducted over the telephone once in 15–20 days, depending upon the convenience of the client. The details of each session, assessment done, and techniques adopted to address the issues are given in Table 1.
Details of Tele-Case Work Intervention
The initial stage of treatment focused on building therapeutic relationship and offering immediate first line psychological aid to alleviate the client’s distress.11,12 At the beginning of every session, the client was provided a safe space to express her feelings. The therapist would listen to her concerns empathetically, offered support nonjudgmentally, and reassured her that she was not alone. The client’s feelings were validated by asserting that the abuse was not her fault and appreciating her for having shown the courage to seek external help for preventing violence. The immediate needs and concerns of the client were assessed. The client wanted to share her distress; she needed professional guidance to explore the options available to prevent the ongoing violence and wanted financial assistance to run the family. The client was confused about whether to seek help from the police against her husband while also being worried about the repercussions of action from the husband towards her and the children. The self-confidence and problem-solving ability to deal with the problem were low, as the client could not solve the issues. These issues were addressed in subsequent sessions using a problem-solving approach.
During the tele-sessions, the therapist ensured the utmost safety of the client by checking whether the abusive husband was around. Prior to the session, she was hinted what she should say if the perpetrator suddenly enters the home while the session is in progress. she was asked to respond only in “yes” or “no,” use code words such as “rose,” or switch to a neutral topic such as cookery if the perpetrator was around. She was also advised to delete the incoming and outgoing callers’ list immediately after the session, to prevent tracking or monitoring of calls. The immediate risk of violence was assessed using a danger assessment scale 13 to ensure the safety of the client and her children. The result revealed a moderate level of risk of danger from the husband. Safety skills were taught to protect and escape from the abusive partner if the client perceives danger to herself and her children. She was provided contact details of local women’s helpline, designated protection officer under the Protection of Women for Domestic Violence Act, 2005, and addresses of nearby shelter care homes for availing service in case of crisis.
The therapist adopted a woman-centric approach in the long-term sessions, mainly guided by two fundamental principles of respect for women’s human rights and promotion of gender equality. 11 Throughout the sessions, the therapist created an accepting therapeutic environment by acknowledging her concerns nonjudgmentally and making her feel that violence was not her fault. The therapist accredited her strength and appreciated her for the courage she had taken to disclose her experiences. In the process, the therapist educated her regarding the abusive dynamics and power control in the marital relationship context and the possible preventive steps that could be taken to break the cycle of violence and take control of her situation. She was educated about her rights and the available legal options. The therapist enhanced the client’s problem-solving and decision-making skills in subsequent sessions, which facilitated the client to approach the free legal authority for legal counselling and explore legal options available to exercise her rights. Currently, the client is continuing tele-follow-up sessions at the AWAKE Clinic. She has been referred to local women’s organizations for financial aid and employment. From the telesessions, the therapist observed improved problem-solving skills, coping skills, and self-confidence level of the client to deal with issues by taking control of her situation. The therapist also observed clarity in the thought process in resolving the issues, where she was empowered to seek external support to seek legal options.
Strengths and Challenges Faced by the Therapist
Offering online tele-case work consultation has specific strengths and challenges in the current case scenario. The strength was that the therapist could provide immediate psychosocial first aid to the client in a safer environment, to vent out distress. It was cost-effective and accessible and reduced the travel time for the client, which was the need during the pandemic. The client could access the online therapy sessions during the lockdown while at home. However, the therapist could not assess the nonverbal behaviors, which are important for assessments during the tele-sessions. Having a specific timeline for each session was difficult as a few sessions got longer than planned, which mentally exhausted the therapist and resulted in difficulty sustaining concentration for long hours. A few sessions were disrupted due to poor network connectivity, where the therapist had to repeatedly reconnect to her, which inhibited the flow of continuity of the sessions. Keeping session lengths and times consistent can be more difficult if tele-session is viewed differently than an in-person consultation.
Discussion
The above case scenario clearly explains ways of offering tele-case-consultation to DV victims during COVID-19 lockdown. It is also important to assess the relative benefits and risks of providing case work management services using technology. For example, in-person services may be necessary when the client poses a significant risk of self-harm or harmful behavior or is cognitively impaired—then an appropriate immediate referral should be made by the therapist. The therapist should share information about the range of available tele-case work management options (e.g., audio/video/telephone) to the client and choose between the options based on technological support available to, preferences of, and suitability for the client. Informed consent is essential after the detailed evaluation and assessment of suitability, before initiating tele-sessions. In the current case scenario, the therapist adopted all these procedures before registering the client for tele-case work consultation.
In times of social distancing measures to curb COVID-19, Gelder et al. 14 recommend internet-based help platforms, replacing conventional in-person support to DV survivors, with a safety mechanism to quickly exit the page and clear browsing history as the abusers may monitor phone and internet use. Vranda and Febna 15 outlined the prerequisite for offering consultation using tele-health services to ensure women’s safety. Evans et al. 16 suggest safety measures such as establishing signals such as raised fist on a video call or setting phrases during an audio call to identify the presence of an abusive partner during teleconsultation. Other safety practices such as deleting internet browsing history or text messages, creating a separate confidential email account for easy communication with therapists, etc., should also be used while offering tele-consultation. Freed et al. 17 recommend designing interface-level security measures that can distinguish the abuser from the victim based on behavioural, keystroke, or contextual cues. In the current case scenario, the therapist ensured the client’s safety by advising the client to delete the caller history from the record immediately after the sessions to prevent the abusive husband from tracking the calls.
COVID-19 has posed significant challenges to human rights, especially the rights of women and children. UN general secretary 18 declared to “put women and girls at the centre of the efforts to recover from COVID-19.” Several countries have enacted innovative measures and policies to prevent violence against women. In India, the Ministries of Health and Women and Child Development have not take the matter seriously. A separate WhatsApp number was launched by National Commission for Women, New Delhi, to help DV victims. However, this may not be adequate enough, and far more serious attention is required in this area. Moreover, no policy level guidelines have been issued at the national or state level to declare DV as an emergency or to announce DV services or health services as essential either during the lockdown or post-lockdown period. 19 WHO 1 recommends providing sexual and GBV and sexual reproductive health services to be considered essential services during any emergency. There is a growing need for novel digital approaches in supporting DV victims, particularly in a pandemic situation. However, currently, little is known about the impact of service delivery through digital modalities than face-to-face approaches, and this needs to be studied extensively.
Recommendation and Conclusion
There is a need to frame guidelines and safety protocols to respond to DV using tele-technological tools. Health care professionals should identify and use DV digital tools and reinforce digital safety nets for DV survivors. Health care professionals need to be trained on safety protocol and guidelines while offering digitally-driven interventions to DV survivors in clinical settings. Researchers in DV must develop digitally-driven emergency preparedness into future service delivery protocols based on the lesson learned from existing experiences and services. There is an urgent need to create and test digitally delivered responses using technological tools, by the researchers, interventionists, and disaster preparedness team, for a complex problem like the COVID-19 pandemic to protect women against DV.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.