
Abstract
Background:
Post-traumatic stress disorder (PTSD) is an understudied construct in the psychiatric setting. The majority of existing Indian studies on PTSD focus on the general population or disaster-stricken communities. Here, we present data from a five-year retrospective chart review from a tertiary care psychiatric center in India.
Methods:
Medical records of adult patients (≥18 years) who had attended psychiatry outpatient services between April 1, 2015 and March 31, 2020 (five years) and were diagnosed with PTSD, as per ICD-10 criteria, were reviewed (n = 113). The relevant sociodemographic and clinical details were extracted using a semistructured pro forma.
Results:
The percentage of adult patients with PTSD diagnosis in the five years was 0.22%. PTSD was more common in females (n = 65, 57.5%). Most patients had interpersonal trauma (n = 85, 75.2%), specifically sexual abuse (n = 47, 41.6%).The median age of onset was 22 years. All the patients had re-experiencing symptoms, with an equally high rate of avoidance (n = 109, 96.5%) and arousal symptoms (n = 110, 97.3%). 82%(93) had a comorbid psychiatric disorder, with mood disorder being the most common (n = 44, 38.9%). Males had a higher rate of comorbid substance use disorder (n = 14, 29.2%) and depression (n = 20, 42%), and females had a higher rate of comorbid dissociative disorder (n = 13, 20%). Most of the patients received non-trauma-focused psychological interventions, and only 18% (20) received evidence-based trauma-focused psychological interventions.
Conclusion:
Interpersonal trauma, specifically sexual abuse, largely contributes to PTSD among adults attending psychiatric services. The need for trauma-focused psychological interventions is underscored.
Keywords
There is a high prevalence of interpersonal trauma and comorbid psychiatric disorders among adults with PTSD visiting tertiary care psychiatric settings. Only a small proportion of them receive evidence-based psychological interventions receive evidence-based psychological interventions. There is a need for evidence-based psychological interventions for addressing PTSD in psychiatric settings.Key Message:
Posttraumatic stress disorder (PTSD) is characterized by four cardinal symptoms—experiencing or witnessing a stressful event, re-experiencing symptoms of the traumatic event, avoidance of the reminders of the traumatic event, and hyperarousal. PTSD is one of the severe reactions to psychological trauma. However, PTSD has not been well examined in the psychiatric setting.
The lifetime prevalence rates of PTSD range from 14% to 53% in the psychiatric population. 3 The prevalence of PTSD in the general population in India was 0.24%. 4 However, the prevalence of PTSD in psychiatric settings in India is largely unknown. The vast majority of Indian studies have investigated PTSD construct in disaster-stricken community populations.2,5 Two studies from India reported the prevalence of PTSD among adults visiting psychiatric settings. These studies, however, focused only on those exposed to specific traumas, such as intimate partner violence and child sexual abuse. In one study, Chandra et al. 6 reported that almost 12% of adult female patients exposed to intimate partner violence had PTSD. In another study, Radhika et al. 7 found that 15.4% of adult psychiatric patients who were exposed to child sexual abuse had PTSD.
PTSD usually co-occurs with other psychiatric disorders. 8 Previous Indian studies have not systematically documented comorbidities in those diagnosed with PTSD. Western studies have revealed a high prevalence of interpersonal trauma and often, multiple and prolonged exposure to trauma among patients with PTSD in psychiatric settings.9, 10 However, none of the previous Indian studies looked at trauma characteristics, that is, type of trauma, the age of trauma exposure, and the number of traumatic events in adults with PTSD, especially in psychiatric settings. In western studies, only a small percentage of patients with PTSD received trauma-focused interventions in clinical settings. 11 So far, no Indian study has reported the type of psychological interventions received by adults with PTSD in a psychiatric setting.
Existing Indian studies on PTSD have focused either on the general population or disaster-stricken community, except for two studies from the psychiatric setting, which were trauma-specific or gender-specific. Therefore, we have undertaken this retrospective chart review study in a psychiatric setting. It had three objectives: (a) to examine the sociodemographic and clinical profiles of adults with PTSD, (b) to compare symptoms of PTSD and comorbid psychiatric disorders among adult males and females with PTSD, and (c) to examine the type of psychological interventions received by adults with PTSD.
Methods
Selection of Participants
This was a retrospective chart review study with a descriptive research design. The study was carried out at National Institute of Mental Health & Neurosciences (NIMHANS), Bengaluru, a tertiary care center in southern India. The hospital register (electronically available) was accessed to find out the total number of patients registered for psychiatric services and the total number of adult patients (≥18 years) diagnosed with PTSD from April 1, 2015, to March 31, 2020 (five years). We used a complete enumeration approach to collect the data. Totally, 59,769 patients were registered for psychiatric services in these five years. We identified 131 adult patients with a diagnosis of PTSD as per ICD-10 (F43.1). Of these, we excluded 18 as they lacked detailed workups and adequate information. After exclusion, charts of 113 patients (74 outpatients and 39 inpatients) were included for the detailed review and analysis.
Tools
The data were extracted using a semistructured pro forma prepared for this study. The details extracted from the charts included sociodemographic profile (age, gender, education, occupational status, marital status, socioeconomic status) and clinical details such as symptoms of PTSD, onset, comorbid psychiatric disorders, trauma characteristics (age of exposure to the trauma, type of trauma exposed, number of trauma exposures, and perpetrators), and type of psychological interventions received.
Procedure
The first author extracted the data from the psychiatry charts and coded the data on an Excel sheet. The data extracted were verified by the other authors. Initially, pilot testing was done to check the availability of data on selected study variables and to assess the semistructured pro forma, overall study design, and feasibility. For this purpose, charts from the past year with PTSD diagnosis were reviewed.
The detailed workups, initial coding, and diagnosis were made by postgraduate trainees, that is, junior residents in psychiatry,Mphil in clinical psychology/psychiatric social work trainees. One of the senior mental health professionals double-checked each file’s coding for accuracy and errors before arriving at the final diagnosis.
ICD-10 criteria were used to capture the symptoms of PTSD, and the same was documented in the charts. We captured the comorbid psychiatric disorders based on the diagnostic impressions given in the charts. The details of trauma characteristics were coded using the terminologies related to trauma characteristics as given in the literature. For the categorization of trauma, Forbes et al. (2014) 12 was referred. Information on the type of psychological intervention received was coded based on the psychological intervention notes in the charts. A password-protected computer was used to store the data, and personally identifiable information of the patients was removed while recording the data. Institutional Ethics Committee approved the study.
Statistical Analysis
Data obtained were analyzed using Statistical Package for the Social Sciences version 23.0 for Windows (IBM SPSS Statistics for Windows, version23.0). Sociodemographic and clinical characteristics were analyzed using frequencies, percentages, proportions, and central tendencies. The proportions between the two groups were compared using Pearson’s chi-square test. The statistical significance was set at P < 0.05 (two-tailed).
Results
The total number of registered patients in psychiatry between April 1, 2015, to March 31, 2020, was 59,769. Among them, 131 (0.22%) adult patients had a file diagnosis of PTSD.
Sociodemographic Characteristics
The mean (±SD) age of the patients was 30 ± 10.57 years. The majority of the patients were young adults, females, never married, belonged to middle socioeconomic strata, and were employed (see Table 1).
Sociodemographic Characteristics (N = 113)
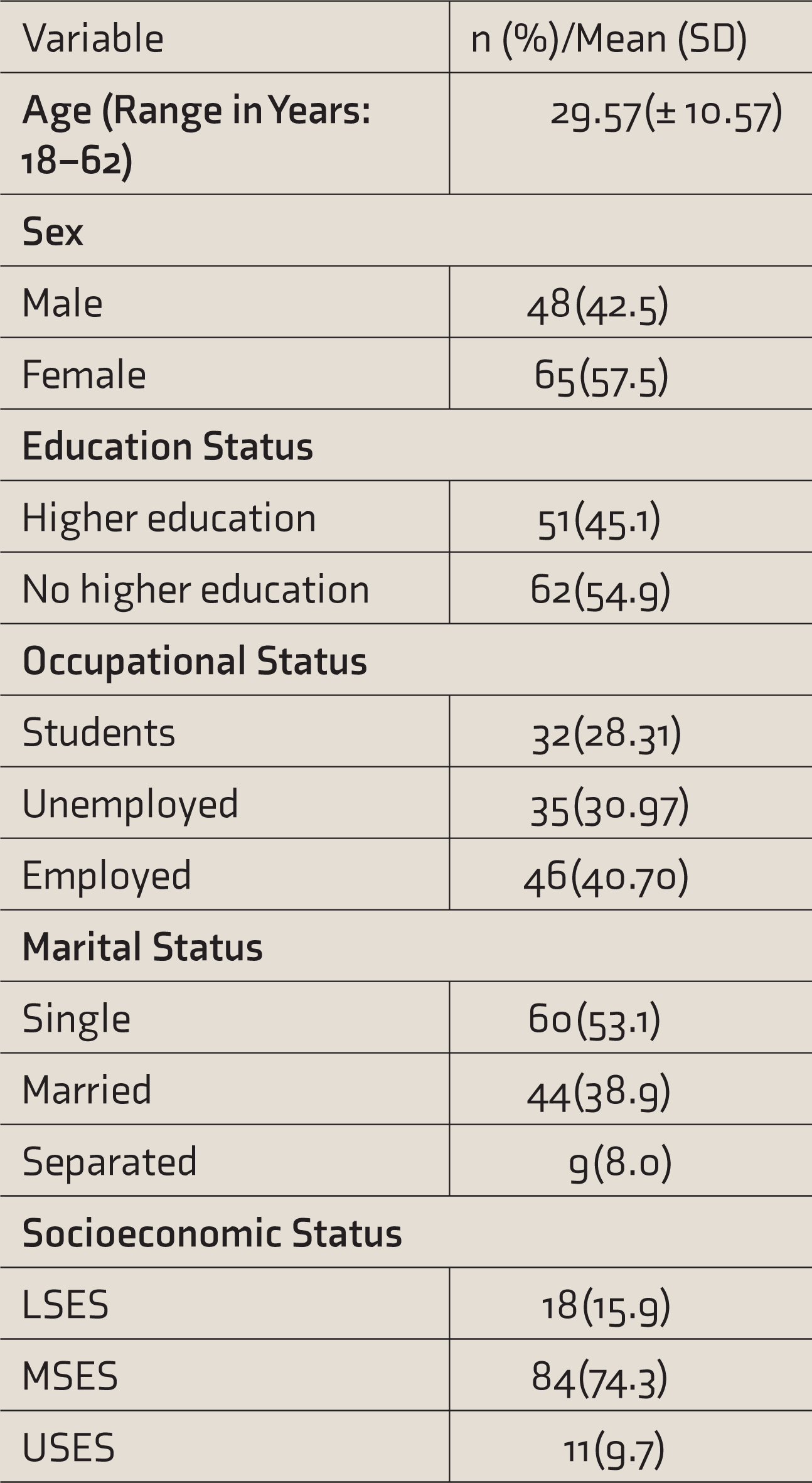
LSES: lower socioeconomic status, MSES: middle socioeconomic status, USES: upper socioeconomic status, SD: standard deviation. Higher education refers to tertiary level of education which is obtained after class 12th.
Trauma Characteristics
The median age of trauma exposure was 21 years (range 7–61 years). A majority were exposed to interpersonal traumas, with more females reporting the same compared to males. Sexual abuse was the most frequently reported interpersonal trauma in females. Among non-interpersonal traumas, exposure to accidents was significantly higher in males than females. Close relatives were identified as perpetrators in the majority of sexual abuse cases (see Table 2).
Trauma Characteristics
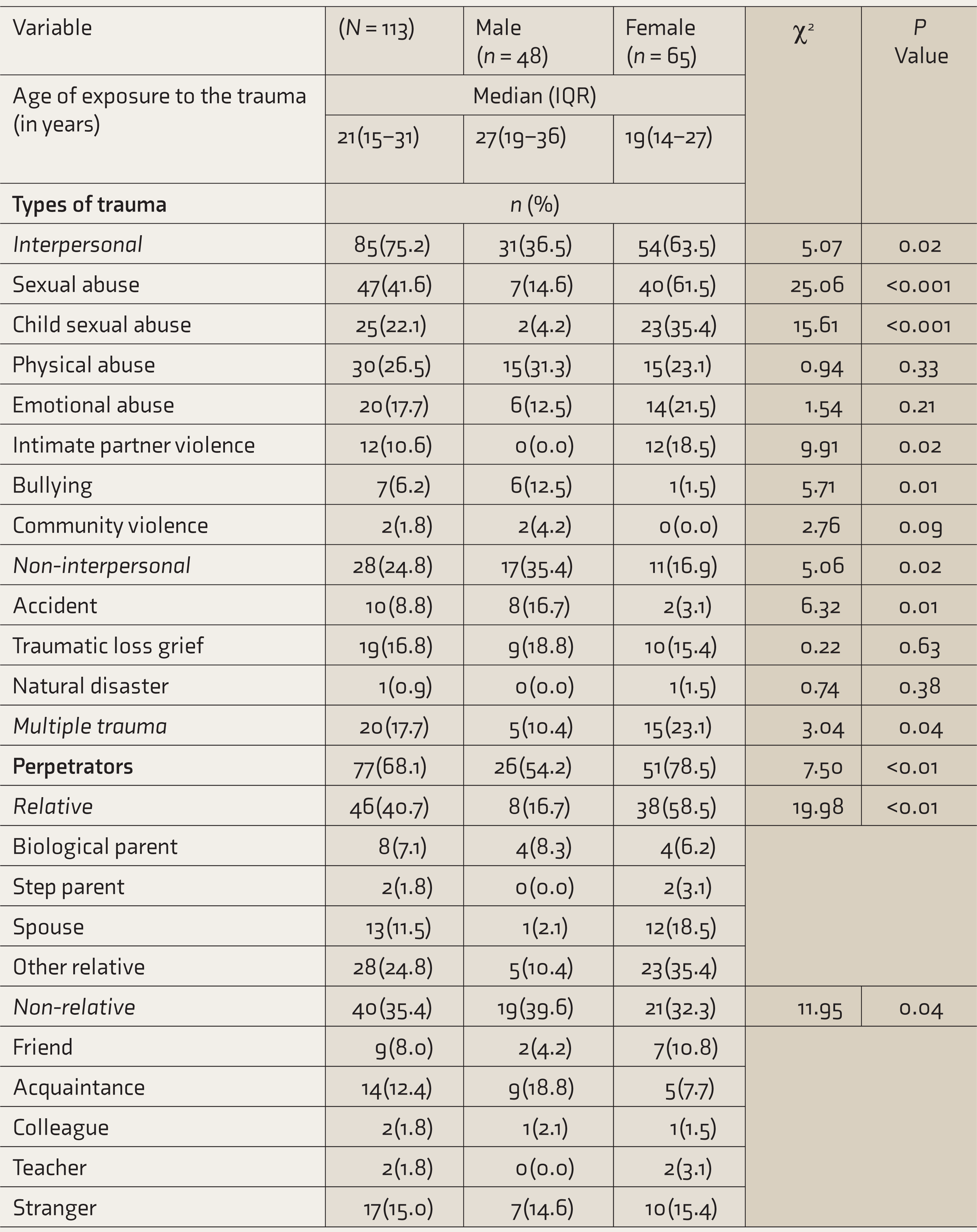
IQR: interquartile range. Based on their nature, various types of traumas are categorized under the headings of interpersonal traumas,non-interpersonal traumas and multiple traumas. Various perpetrators are categorized as Relative and Non-relative.
Symptoms of PTSD and Comorbid Psychiatric Disorders
The median age of onset of the PTSD symptoms was 22 years. With respect to symptoms, all the patients had re-experiencing symptoms of PTSD, followed by a majority having at least one of the arousal symptoms (sleep difficulties, hypervigilance, irritability, and anger) and avoidance symptoms. Comorbid psychiatric disorders were reported in 82% of the patients, with mood disorders being the most common, followed by anxiety and stress-related disorders and substance use disorders. Male patients with PTSD had a significantly higher percentage of substance use disorder and depression, whereas female patients with PTSD had a significantly higher rate of comorbid dissociative disorder (see Table 3).
Symptoms of PTSD and Comorbid Psychiatric Disorders
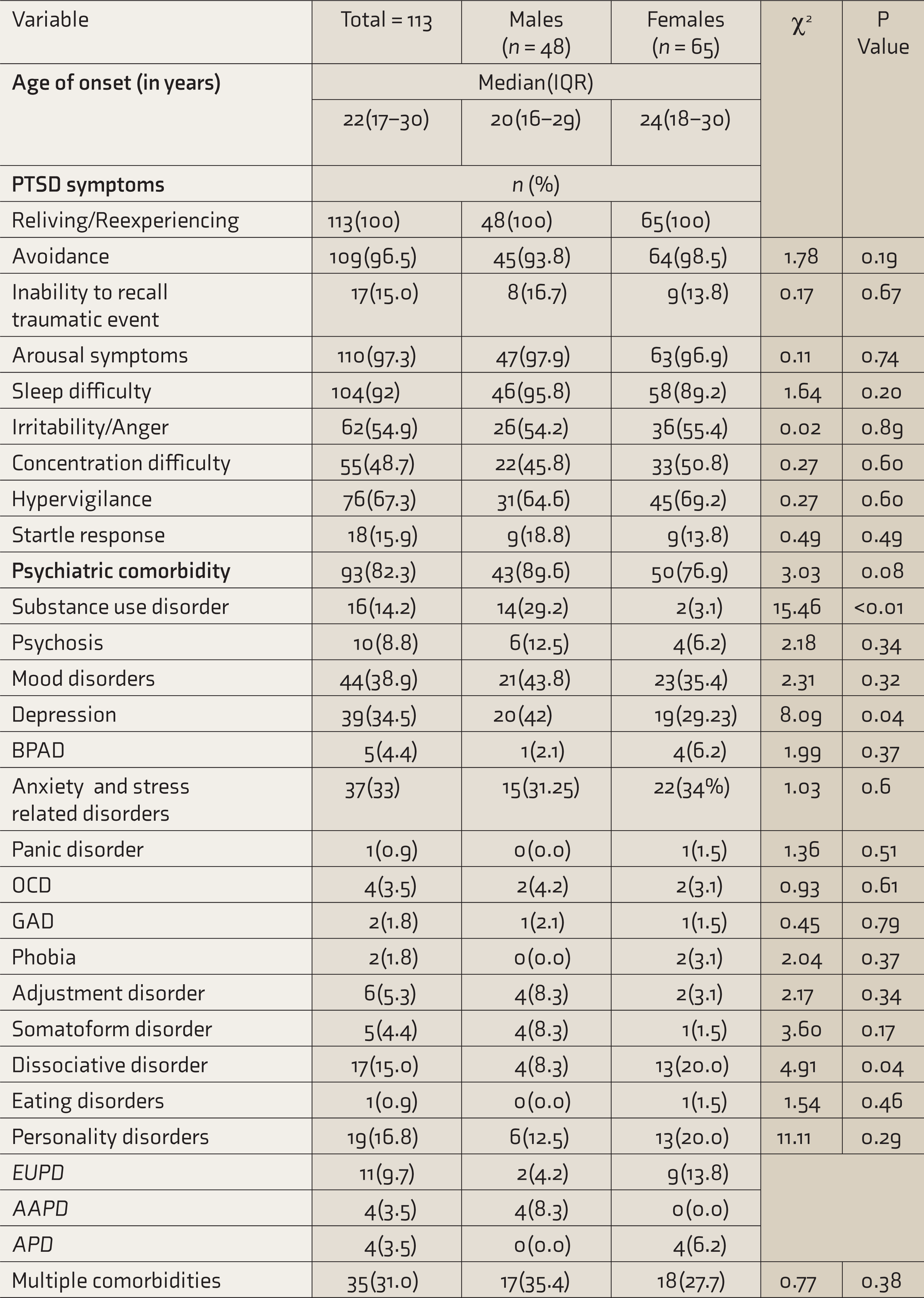
PTSD: post-traumatic stress disorder, BPAD: bipolar affective disorder, OCD: obsessive compulsive disorder, GAD: generalized anxiety disorder, EUPD: emotionally unstable personality disorder, AAPD: anxious avoidant personality disorder, APD: anankastic personality disorder, IQR: interquartile range.
Psychological Intervention
A total of 55% of the patients received at least one psychological intervention session. About 25% of them received supportive psychotherapy, 18% received trauma-focused therapies (cognitive behavior therapy—9.73%, narrative exposure therapy—6.19%, dialectical behavior therapy for PTSD—1.76%,), 12.4% received integrated psychotherapies, and 1.76% also received family therapy in addition to the above-mentioned individual therapies.
Discussion
This study examined PTSD as presented in a tertiary care psychiatric setting based on the chart review data of adult patients. Our study is one of the few studies with data on PTSD from a psychiatric setting. The sociodemographic profile showed that most of the patients were young adults, employed, unmarried, and hailing from middle socioeconomic strata, with female patients making a large portion of the sample (see
Contrary to the findings of previous studies in the psychiatric population,10,15 our study showed a much lower percentage of PTSD (0.22%). The first important reason for the same could be that our data is from a specialized tertiary care psychiatry center. In the previous studies, data were collected from community mental health centers 10 or general hospital psychiatric centers. 15 For instance, Mueser et al. (2004) 10 screened for PTSD in patients receiving treatment for severe mental illnesses through the public mental health system. Also, most of the participants in this study had a primary diagnosis of schizophrenia and schizoaffective disorders, whereas in our study, we included only those patients who had a file diagnosis of PTSD. A second possible reason is that the diagnostic system used in our hospital’s routine clinical evaluation was ICD-10. The rates of PTSD were reported to be higher when DSM-5 criteria were used, compared to ICD-10 and ICD-11.16, 17 The third possible reason is that, since PTSD commonly occurs with other comorbid psychiatric disorders, it may go unidentified, resulting in underreporting of PTSD diagnosis in the charts.18,33 Lastly, previous studies reporting the prevalence of PTSD in the psychiatric population were conducted on western subjects. There might be variations in the manifestation of PTSD symptoms in the Indian culture, as trauma reaction can differ from culture to culture. 19 Such culture-specific symptoms might not have been captured by the diagnostic system used in our routine psychiatric setting. For instance, in the Indian setting, somatic expression of PTSD may be more common than its classic symptoms.19,31, 32
Our study showed that most patients were exposed to interpersonal trauma than noninterpersonal trauma (see Table 2). Of those who had interpersonal traumas, most were females, and a high percentage of them were exposed to sexual abuse perpetrated by close family relatives. Non-interpersonal traumas, such as accidents, were high in male patients. Although many male patients too had exposure to interpersonal traumas such as sexual abuse, the perpetrators were more likely to be strangers and senior acquaintances rather than close relatives. These findings are consistent with previous studies on the general population and psychiatric population.3,8,10, 15
The age of onset of PTSD as observed in this cohort is 22 years, which is comparable to the findings of a previous study
20
that showed 23 years as the median age of onset. With regard to PTSD symptoms, it was found that all patients in the sample had re-experiencing symptoms, and an almost equally high rates of avoidance and arousal symptoms were found (see
A majority of our sample had all three classical symptoms of PTSD namely re-experiencing, avoidance and arousal symptoms. Previously, an Indian study by Mehta et al. 1 on a community sample also found these three symptoms. Our finding regarding avoidance symptoms contradicts the results of a previous Indian study on tsunami survivors, which reported a lower presentation of avoidance symptoms. 2 The reason for lower rate of avoidance symptoms may be that the tsunami survivors had limited opportunity to avoid stimuli associated with the trauma, that is, seashore, destroyed dwellings, etc. They had to return to their destroyed dwellings to ensure their livelihood and reconstruct their lives. Also, because of the collective traumatic experience, they had an opportunity to practice social and religious coping strategies. On the other hand, in our study, majority of the patients had individual traumas that were predominantly of interpersonal type. Interpersonal traumas are usually triggered by interpersonal situations, and there can be a high possibility of avoidance because encountering these stimuli may not always have survival value.
With regard to arousal symptoms, sleep disturbance was the predominant symptom in the majority. Similar findings have been reported in Vietnam veterans (90% had sleep difficulties) and the general population (70%).21,22 This is a serious concern because sleep disturbance in PTSD is associated with negative psychiatric outcomes such as worsening of the comorbid psychiatric conditions and nonresponse to treatment.23,24 Hyper vigilance and irritability/anger were the other two arousal symptoms found in more than half of the patients, and a small percentage had a startle response.
A very high percentage had at least one comorbid psychiatric disorder, with a mood disorder, especially depression, being the most common comorbidity (see
Further, we observed a high rate of comorbid substance use disorders and depression in males compared to females. On the other hand, females were more likely to have the dissociative disorder as comorbidity. Previously, Zlotnick et al. 15 reported high comorbidity of substance use disorder in males with PTSD in a study carried out in a psychiatric setting. However, high comorbidity of depression in males was not found in that study. The rate of comorbid dissociative disorder was high in females because, in our sample, a large proportion of females (35.4%) were exposed to child sexual abuse than males (4.2%). Those exposed to child sexual abuse are more likely to have dissociative symptoms. 30
With regard to the psychological intervention received for PTSD, a vast majority of the patients received nontrauma-focused psychological interventions and only a small proportion of them received evidence-based trauma-focused interventions. Of those who received trauma-focused interventions, most of the patients received cognitive behavior therapy, followed by narrative exposure therapy and dialectical behavior therapy. However, we could not get data on the total number of sessions received as there was a lack of adequate information regarding this in many of the charts. However, our study has succeeded in capturing the most common psychological interventions received by patients with PTSD in a psychiatric setting. Another important finding is that only 55% of the patients received at least one session of psychological intervention, and the rest have not received any psychological interventions. This is of concern as psychological interventions are the first-line treatments for PTSD. Some of the potential reasons for lack of receipt of any form of psychological interventions could be high avoidance symptoms resulting in low motivation to seek help, complex presentation of PTSD symptoms with high comorbidity resulting in more focus on psychiatric treatment of comorbid symptoms and delay in initiating the psychological interventions, and limited utilization of evidence-based psychological interventions for PTSD in routine clinical settings.34,35,36 Also, factors such as time constraints, affordability, and reduced patient engagement might also lead to a lack of provision of adequate psychological interventions for PTSD in Indian psychiatric settings.
Limitations of the Study
The data was entirely based on the documentations found in psychiatry charts. Since the data has been gathered from an exclusive tertiary care center, the findings cannot be generalized. Our finding with regard to the rate of PTSD in a psychiatric setting is only a preliminary finding. Further studies with a more rigorous methodology are required to ascertain the prevalence rate of PTSD in the psychiatric population.
Conclusions and Future Directions
Interpersonal trauma, specifically sexual abuse, was highly prevalent among adults with PTSD in a psychiatric setting. Further studies using structured assessments and more rigorous methodology are required in the psychiatric population. Future studies can assess culture-specific symptoms of PTSD in addition to classic symptoms, using prospective study designs. There is also a strong need for Indian studies on evidence-based interventions specifically focusing on PTSD, especially in the psychiatric setting.
Footnotes
Acknowledgements
The authors would like to thank Dr Mariamma Philip (Department of Biostatistics, NIMHANS) for helping with the data analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.