
Abstract
Background:
The COVID-19 pandemic has led to the risk of common mental illnesses. Consultation liaison psychiatry has been one of the most requested services in the face of this pandemic. We aimed to assess (a) the prevalence of psychiatric illness, (b) different types of psychiatric diagnoses, (c) presenting complaints, (d) reasons for psychiatric referrals, and (e) psychiatric intervention done on COVID-19 positive inpatients referred to consultation liaison psychiatry at tertiary care hospital.
Method:
This was a retrospective study of data collected from April 1, 2020, to September 15, 2020. Total 300 patients were referred and diagnosed with clinical interview and Diagnostic and Statistical Manual for Mental Disorder Fifth Edition criteria. Analysis was done using chi-square test, Kruskal–Wallis test, and fisher exact test.
Results:
Out of 300 patients, 26.7% had no psychiatric illness. Adjustment disorder was the commonest psychiatric diagnosis (43%), followed by delirium (10%). Statistically significant differences were found for parameters like Indian Council of Medical Research Category 4 of the patient, (hospitalized severe acute respiratory infection) (P value < 0.001), medical comorbidity (P value = 0.023), and past history of psychiatric consultation (Fisher exact test statistic value <0.001). Behavioral problem (27.6%) was the commonest reason for psychiatric referral. Worrying thoughts (23.3%) was the most frequent complaint. A total of 192 (64.3%) patients were offered pharmacotherapy.
Conclusions:
Psychiatric morbidity was quite high (73.3%) among them and adjustment disorder was the commonest (43%) psychiatric diagnosis followed by delirium (10%). Pharmacotherapy was prescribed to 64.3% patients and psychosocial management was offered to most of the referred patients.
Consultation liaison psychiatry should be strengthened to deal with the mental health burden of the COVID-19 pandemic. All the COVID-19 patients should be screened for psychiatric illness and nonpsychiatric healthcare workers should also be trained in this direction.Key Message:
COVID-19 has negatively affected mental health and increased the incidence of psychological crisis. 1 Psychological morbidities and chronic fatigue are common in COVID-19 patients. 2 After the declaration of the pandemic, there was an increase in negative emotions and a decrease in positive emotions and life satisfaction. 3 There is a risk of common mental illnesses in patients with diseases that require hospital admission, which may be compounded by the effects of social isolation. 4
A recent survey conducted by the Indian Psychiatric Society indicates a 20% rise in patients who have mental illness during lockdown.
5
In light of the experience from the previous novel virus pneumonia occurrences worldwide, the assessment and management of psychiatric problems are important during the COVID-19 pandemic. This is particularly true of consultation-liaison psychiatrists, who possess expertise at working individually, institutionally, and systemically at the intersection of mental and physical health.
6
It was hypothesized in this study that there is an association between the sociodemographic and clinical profile of the COVID-19 positive inpatients referred to consultation-liaison psychiatry. In this background, the objectives of the study were as follows:
Primary objectives: (a) to estimate the proportion of different types of psychiatric diagnoses, (b) to identify various reasons for the psychiatric referral and presenting complaints, and (c) to identify pharmacological and nonpharmacological psychiatric intervention done among COVID-19 positive inpatients referred to consultation-liaison psychiatry at tertiary care hospital. Secondary objectives: (a) to determine the association of psychiatric illness with sociodemographic and clinical parameters of COVID-19 positive inpatients referred to consultation-liaison psychiatry at a tertiary care hospital.
Materials and Methods
Study Design and Participants
This was a retrospective chart review study. All the data of consecutive COVID-19 positive inpatients referred to and treated by consultation-liaison psychiatry at a tertiary care hospital, from April 1, 2020, to September 15, 2020, were included. The data was extracted from the hospital’s software-based electronic record system by three of the authors. As per statistical calculation for sample size, 246 patients were approximately required; hence, 300 patients referred during this period were taken in the study. There were no exclusion and missing data in the files. All the patients were already admitted to the hospital and referred by a physician. All the patients’ confidentiality and anonymity was strictly maintained. There was no separate interaction with the patients for the purpose of the study. Hence, consent was not taken. The institutional review board approved the study on September 11, 2020.
Measures
All the patients referred to consultation-liaison psychiatry had been assessed by senior psychiatrists. Those patients who had access to mobile phones, were cooperative, and had feasibility were interviewed by using audiovisual technologies. For some uncooperative patients in intensive care units, those who were delirious, and those who did not have access to mobile phones, in-person face-to-face clinical interviews were conducted after using PPE kits. Clinical diagnoses were made using the Diagnostic and Statistical Manual for Mental disorder Fifth Edition (DSM-5) criteria. Patients were given pharmacotherapy in the form of antidepressants, antianxiety agents/hypnotics, antipsychotics, mood stabilizers, and other drugs as per need. They were also advised nonpharmacological management in the form of relaxation techniques, sleep hygiene, and supportive counseling as appropriate.
Statistical Analysis
Sociodemographic and clinical data of the patients were extracted from the electronic records of the hospital along with treatment records. Descriptive and statistical analysis of the collected data was done using Microsoft Excel. Chi-square test and Fisher exact test were used to assess the association of psychiatric illness with sociodemographic and clinical variables.
Results
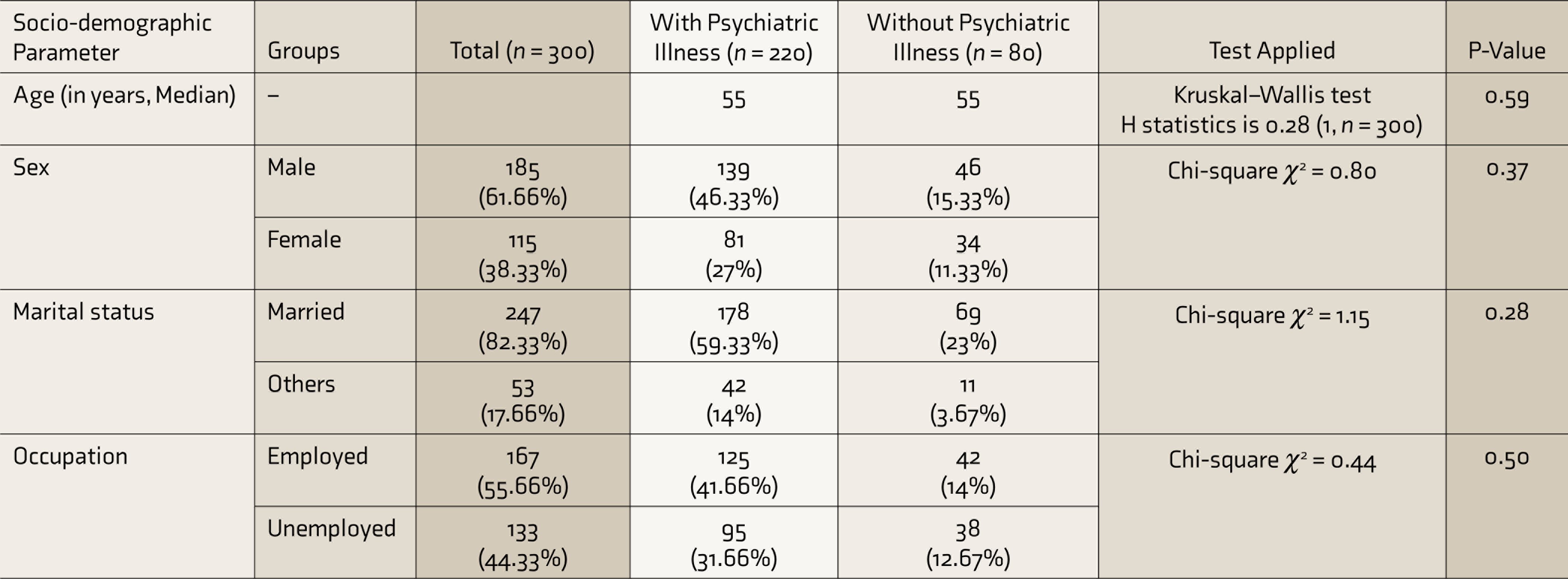
During the study period, a total of 300 patients were referred to consultation-liaison psychiatry. The median age of COVID-19 patients in the sample was 55 years (IQR 66–38). The majority of patients were male (61.6%), married(83.3%), and employed (55.6%).
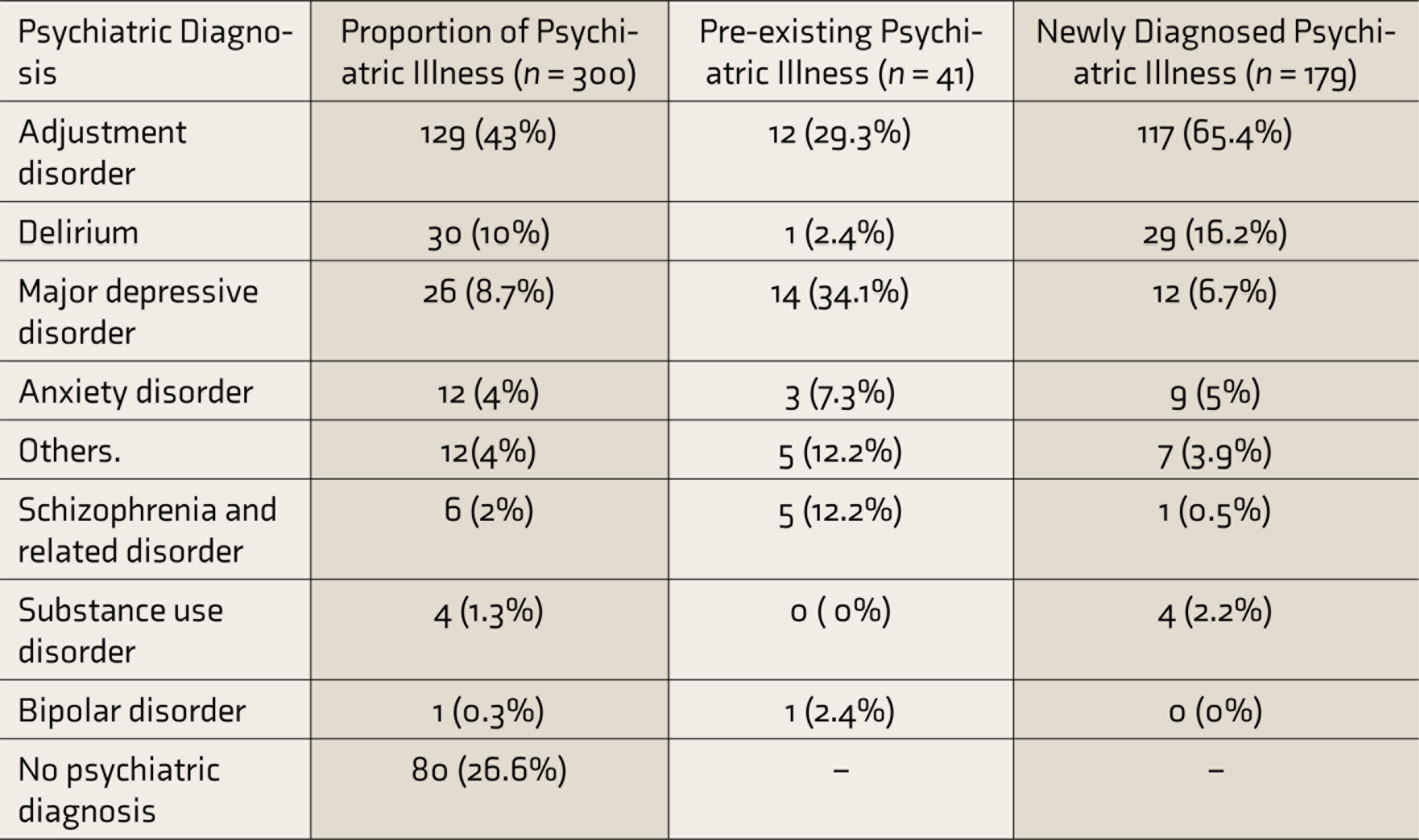
Table 1 shows that out of the 300 patients, 73.3% were diagnosed with psychiatric illness, which included 13.6% patients with a past history of psychiatric illness and 59.6% with newly diagnosed psychiatric illness. Out of 41 patients with psychiatric illness in the past, 63.4% presented with the illness they were diagnosed with in the past, while 36.5% developed different psychiatric illnesses than in the past. Adjustment disorder was the most common psychiatric diagnosis (43%), followed by delirium (10%).
Table 1 shows that among the patients with past psychiatric illness (n = 41), major depressive disorder (34.1%) and adjustment disorder (29.3%) were the most common diagnoses. The proportions of schizophrenia and bipolar mood disorder were 12.2% and 2.4%, respectively. Table 1 also shows that among (n = 179) newly diagnosed patients, adjustment disorder (65.4%) and delirium (16.2%) were the most common psychiatric diagnoses.
Proportion of Psychiatric Illness and Different Types of Psychiatric Diagnoses
Sociodemographic Correlates of Psychiatric Illness
Statistical analysis of sociodemographic parameters such as age, sex, marital status, and occupation, using the Kruskal–Wallis test and chi-square test, is depicted in Table 2. Patients were divided into two groups—with or without psychiatric illness—and checked for statistically significant differences. No statistically significant differences in the presence of psychiatric illness were found among various sociodemographic parameters.
Sociodemographic Correlates of Psychiatric Illness
Clinical Parameters’ Correlation with Psychiatric Illness
The association of psychiatric illness with various clinical parameters was studied (Table 3). The COVID-19 categories were decided based on the Indian Council of Medical Research (ICMR) 7 guidelines. The severity of COVID-19 was assessed by COVID-19 treating doctors based on guidelines given by the Ministry of Health and Family Welfare (MOHFW). 8 Proportion of those with psychiatric illness was significantly higher among COVID-19 patients with ICMR Category 4 (hospitalized, severe acute respiratory illness) (56%, P value < 0.001), medical comorbidity (42%, P value = 0.02), and past history of psychiatric consultation and treatment (Fisher exact test statistic value <0.001). Commonly found medical comorbidities were hypertension, diabetes mellitus, thyroid dysfunction, and dyslipidemia.
Clinical Parameter Correlation with Psychiatric Illness
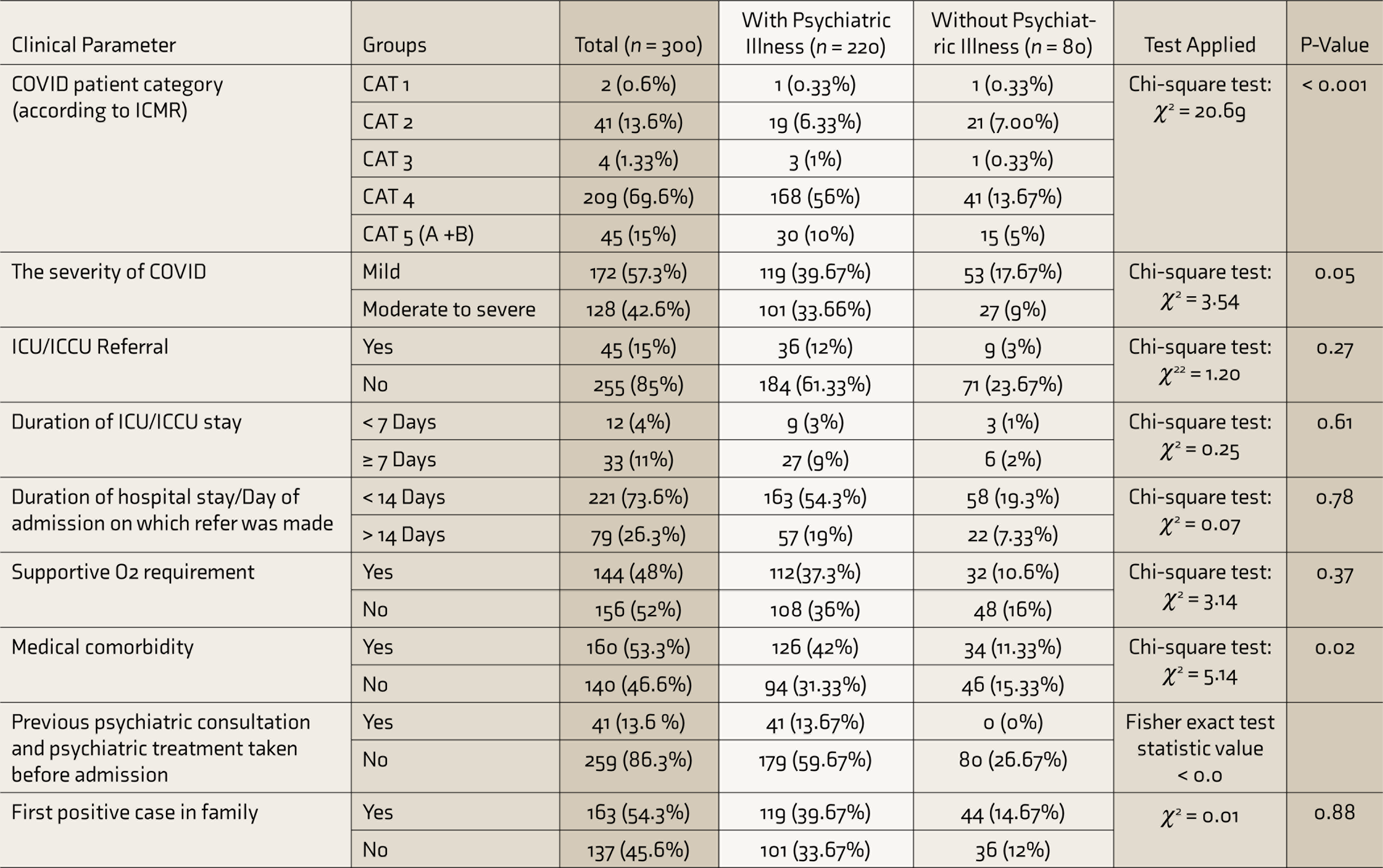
ICMR: Indian Council of Medical Research, ICU: Intensive Care Unit, ICCU: Intensive Coronary Care Unit.
Reason for Psychiatric Referral
Behavioral problem (27.6%) was the most common reason for psychiatric referral, followed by low mood (27%) and anxiety (16%). Among the behavioral problems, apart from patients with delirium and adjustment disorder, the remaining had behavioral problems in the form of irritability, uncooperativeness, and treatment noncompliance due to various stressors like absence of close family members in the hospital, not being able to adjust to the hospital facilities social distancing practices in the ward, and uncertainty about treatment outcome and duration of hospital stay. The other reasons for referral were being a known case of psychiatric illness (13.6%), fluctuation of orientation(8%), and insomnia (6%). Substance use was the least common (1.6%) reason for referral.
Chief Psychiatric Complaints
Worrying thoughts (23.3%) was the most frequent complaint, followed by low mood (19%), insomnia (12%), and fluctuation of orientation (8%). No psychiatric complaint was reported in 25% of patients. Other complaints (13.5% and each less than 5% in frequency) were irritability, weeping spells, unresponsive episodes with multiple vague complaints, obsessive thoughts, withdrawn behavior, forgetfulness, irrelevant talking, visualization of images, tobacco use, alcohol use, headache, hearing of voices, and suspiciousness.
Psychiatric Treatment Advised
Pharmacotherapy and psychotherapy both were given to 45.6% patients. Pharmacotherapy alone was given to 18.6% of patients. General psychosocial measures such as sleep hygiene, removal of misconceptions related to COVID-19, and reassurance were advised to 80% of patients. Specific psychosocial intervention such as relaxation techniques, teaching distraction techniques, and supportive counselling to help alleviate anxiety, depression, and negative emotional responses was done in 22.6% of patients. Most frequent pharmacotherapy was anti-anxiety/sedative drugs (65.8%) followed by antidepressants (36.7%), antipsychotics (17%), mood stabilizers (0.5%), and others (4%).
Discussion
This is one of the very few studies on consultation-liaison psychiatry during COVID-19, especially in India. It is also unique in a way that it involves a large sample size (300) compared to other similar literature worldwide (studies from Qatar and Morocco).9,10 The study results will provide the portrait of psychiatric illness associated with acute COVID-19 and help formulate the further consultation-liaison guidelines for pharmacological and nonpharmacological intervention among COVID-19 positive inpatients.
Sociodemographic Profile
In this study, the median age of COVID-19 patients was 55 years (IQR 66–38). In the study by Arbeloet al., 11 the median age was 64 years (IQR 54–73). In this study, majority of the patients were male (61.6%), which was similar to the study by Iqbal et al. 9 (96% male) and contrary to the study by Benjelloun et al. where 55.5% were female. 10 There were almost equal numbers of male and female COVID-19 patients in the study by Kong et al. 12 In this study, majority (82.3%) of COVID-19 patients were married. Similar findings were reported by Zhang et al. 13 where 78.6% were married.
Proportion and Pattern of Psychiatric Illness
As shown in Table 1, out of a total of 300 COVID-19 patients referred to consultation-liaison psychiatry, 80 (26%) patients were not diagnosed with psychiatric illness. This difference can be explained by the initial transient emotional response to the stress related to COVID-19, for which the reference was made. This emotional response might have resolved or was not persistent enough for a diagnosis of psychiatric illness at the time of psychiatric evaluation. In the study by Iqbal et al., 9 out of 50 patients referred to consultation-liaison psychiatry, only 2% of patients were not having psychiatric illness. Difference in sample size, sample characteristics, assessment tools, etc., may contribute to such differences.
In this study, adjustment disorder was the most common psychiatric diagnosis (43%). Delirium was the second most common (10%) psychiatric diagnosis in our study and the most common diagnosis in other studies like Grover et al. 14 (a study before COVID-19 pandemic) and Iqbal et al., 9 (a study among COVID-19 positive inpatients). The proportions of major depressive disorders and anxiety disorders were 8.7% and 4%, respectively, in this study, which was less than the results found by Iqbal et al. 9 (16% and 16%, respectively). This may be due to the diagnostic tool used—DSM-5 in ours and ICD in theirs. There was no diagnosis of adjustment disorder made in other study, and we presume that even those cases have been diagnosed as either anxiety or depression in that study. The proportion of schizophrenia and related disorders was 0.4%, which was again lesser than the proportion (non-affective psychosis 18%) found by Iqbal et al. 9 Another study by Varatharaj et al. 15 found that out of 39 patients with altered mental status, 25% had new-onset psychosis, which was higher than that found in this study. The results are not directly comparable as the mentioned studies had studied all the COVID patients (confirmed, probable, and possible) and not just those referred to consultation-liaison psychiatry as in our case.
The traditional joint family existing in India is seen as a source of social and economic support and is known for its tolerance of deviant behavior and capacity to absorb additional roles in times of crisis.16,17 Here in COVID-19 patients, due to hospitalization and isolation, family support is deficient as patients may not be able to communicate with their relatives, and they faced this crisis alone in the hospital, which may have contributed to development of psychiatric illness.
Pattern of Psychiatric Illness in Patients with Past Psychiatric Illness
As shown in Table 1, 3.6% of patients already had a psychiatric illness before the COVID-19 pandemic. In a study by Benjelloun et al., 10 7 (19%) out of 36 COVID-19 patients had a past history of psychiatric illness. In a study by Iqbal et al., 9 one-third of the patients referred for consultation-liaison psychiatry had a past history of psychiatric illness (slightly higher than our study), of which nearly half of the patients had psychotic or bipolar 1 disorders. In this study, out of the 41 patients with a past history of psychiatric illness, 63.4% presented with the illness they were diagnosed with in the past, while 36.5% developed different psychiatric illnesses than in the past. On the other hand, in the study by Varatharaj et al. 15 out of 23 COVID-19 patients with altered mental status, only 2 (8%) had exacerbations of preexisting psychiatric illness. This suggests that COVID-19 patients not only had worsening of a preexisting problems but also developed new illnesses.
Types of Different Newly Diagnosed Psychiatric Illness
Among the newly diagnosed patients with psychiatric illness, most (65.4 %) were diagnosed with adjustment disorder (Table 1).This includes depressive, anxiety, emotion, and conduct symptoms due to the stress of having COVID- 19 per se. In this study, 16.2% of patients had newly diagnosed delirium. Similarly, in the study by Arbeloet al., 11 12.6% of COVID-19 patients had newly diagnosed delirium.
Sociodemographic Correlates of Psychiatric Illness
As shown in Table 2, psychiatric illness was higher among employed (41.6%) than unemployed (31.6%), which may be due to various reasons like fear of contracting COVID-19 at the workplace, uncertainty about salary, and insecurities of being jobless due to the overall economic impact of COVID-19. No statistically significant differences in the presence of psychiatric illness were found among those with different sociodemographic parameters such as age, sex, marital status, and occupation. In contrast, in the study by Kong et al., 12 multiple linear regression analysis showed that female sex (P = 0.034) and older age (P = 0.003) were significantly associated with anxiety, and older age (β = 0.084, P = 0.001) was significantly associated with depression.
Clinical Parameters’ Correlation with Psychiatric Illness
Psychiatric illness (P value < 0.001) was significantly higher among ICMR Category 4 (hospitalized severe acute respiratory illness) patients (P value≤ 0.001; Table 3). This may be due to the COVID-related deterioration of physical health and social isolation leading to further stress and other psychiatric problems. Uncertainty about disease outcome and barrier nursing may add to the stress related to COVID-19. Nonpsychiatric healthcare workers should also be trained to screen and identify the psychiatric problems in patients with COVID-19. A total of 78.7% (126/160) of patients with medical illnesses had psychiatric comorbidity. Medical comorbidities were significantly associated with psychiatric illness (P = 0.02). Similarly, in the study by Arbelo et al., severe somatic comorbidities were significantly associated with delirium, severe mental illness, and nonsevere mental illness. 11
Past history of psychiatric illness was also significantly associated with psychiatric illness at present (Fisher exact test statistic value < 0.001). Everyone who had a history of psychiatric illness or consultation in the past had a relapse of preexisting illness or onset of the new psychiatric syndrome. This suggests the need to acknowledge the mental health pandemic that accompanies pandemics like COVID-19. One solution is the involvement of consultation-liaison psychiatrists in the COVID-designated centers for proactive screening of psychiatric problems and their management. Video conferences or telephonic helplines should be offered wherever possible. Community health workers should also be trained for awareness creation and screening for psychiatric illnesses at the community level.
Reason for Psychiatric Referral and Chief Psychiatric Complaint
Out of 83 (27.6%) COVID patients referred for behavioral problems, 37 (44%) received the diagnosis of adjustment disorder and 17 (20%) received the diagnosis of delirium, which are reflected as the two most common psychiatric diagnoses in our study. Such problems seek the role of psychiatric social workers or counsellors in the COVID designated hospitals. Low mood can be the initial transient emotional response to the stressful event of getting COVID-19 and admission to hospital for which the primary treating doctor might have referred them to the psychiatry liaison, but on detailed clinical evaluation and interviewing, we did not find persistent low mood amounting to psychiatric diagnosis and also, in some, the low mood had already been resolved, and hence there is difference between proportion of referred and diagnosed patients with low mood. The primary treating doctors in COVID-19 ward are not trained enough for detailed psychiatric assessment. Those patients who were referred for complaints other than insomnia were also evaluated for insomnia in detail by a psychiatrist. Hence, the proportion of insomnia was higher in diagnosed patients than in those who were referred. The study by Iqbal et al. 9 showed insomnia (70%) and anxiety (64%) to be the most frequent psychiatric complaints, and depressed mood was present among 42% of patients. As reported by Rogers et al., 18 in COVID-19 the most important finding was confusion (27.9%), suggesting that delirium was common, and other common psychiatric findings were depression, anxiety, and insomnia.
Psychiatric Intervention Done
Pharmacological intervention was offered to 64.3% of patients in our study. Similarly, in the study by Arbelo et al., 11 63.4% COVID patients received psychiatric medications. The antianxiety agents/sedatives, antidepressants, and antipsychotic medications were prescribed to 65.8%, 36.7%, and 17% patients, respectively, in our study and 35%, 42%, and 23%, respectively, in the study by Arbeloet al. 11 Benjelloun et al. 10 prescribed psychotropic medications for 55.5% of patients, which was slightly less than our study and consisted of anxiolytics/ hypnotics for 95% and antipsychotic for 5% of patients.
Limitations and Future Direction
This study has some limitations. As it was done in a single center, it reflects the picture of only one setting, and the results cannot be generalized to the whole country. There would be COVID-19 patients in other COVID-19 centers, which requires a multi-center study for more specific results. Moreover, in this study, only those referred to consultation-liaison psychiatry were included, but those not identified by physicians and hence not referred but actually had psychiatric problems may have been missed. Here the severity of psychiatric illness was not measured using questionnaires, which may be an objective of future research.
Conclusion
Adjustment disorder was the most common psychiatric diagnosis, followed by delirium. Behavioral problems, followed by low mood, were the commonest reason for referrals. Worrying thoughts was the commonest psychiatric complaint. Psychosocial management was advised in most patients, and pharmacotherapy was also advised in a substantial number of patients. Consultation-liaison psychiatry should be strengthened to deal with the mental health burden of the COVID-19 pandemic, and nonpsychiatric health care workers should also be trained to identify common psychiatric problems.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.