
Abstract
Background:
Among the Indian adolescents, the prevalence of psychiatric morbidity and alcohol use disorders (AUD) are 7.3% and 1.3%. However, no separate data are available for indigenous tribal populations. This study estimated the prevalence of psychiatric morbidity and AUD and associated socio-demographic factors among adolescents in the tribal communities in three widely varying states in India.
Methods:
Using validated Indian versions of the MINI 6.0, MINI Kid 6.0, and ICD-10 criteria, we conducted a cross-sectional survey from January to May 2019 in three Indian sites: Valsad, Gujarat (western India); Nilgiris, Tamil Nadu (south India); and East Khasi Hills district of Meghalaya (north-east India) on 623 indigenous tribal adolescents.
Results:
Aggregate prevalence of any psychiatric morbidity was 15.9% (95% CI: 13.1–19.0) (males: 13.6%, 95% CI: 10.0–18.1; females: 17.9%, 95% CI: 13.9–22.6), with site-wise statistically significant differences: Gujarat: 23.8% (95% CI: 18.1–30.2), Meghalaya: 17.1% (95% CI: 12.4–22.7), Tamil Nadu: 6.2% (95% CI: 3.2–10.5). The prevalence of diagnostic groups was mood disorders 6.4% (n = 40), neurotic- and stress-related disorders 9.1% (n = 57), phobic anxiety disorder 6.3% (n = 39), AUD 2.7% (n = 17), behavioral and emotional disorders 2.7% (n = 17), and obsessive-compulsive disorder 2.2% (n = 14). These differed across the sites.
Conclusion:
The prevalence of psychiatric morbidity in adolescent tribals is approximately twice the national average. The most common psychiatric morbidities reported are mood (affective) disorders, neurotic- and stress-related disorders, phobic anxiety disorder, AUD, behavioral and emotional disorders, andobsessive-compulsive disorder.
This study estimated the prevalence of psychiatric morbidity and AUD among Indian adolescents tribals (11–19 years) in three Indian states using MINI 6.0 and MINI Kid 6.0.Key Messages:
The prevalence of any psychiatric morbidity was 15.9% (males: 13.6%, females: 17.9%) and AUD was 2.7%.
The most common psychiatric morbidities reported were mood (affective) disorders, phobic anxiety disorder, alcohol use disorder, and obsessive-compulsive disorder.
Despite constituting 8.6% of the Indian population, over ten crore indigenous tribal population (as of 2011) are among the most geographically isolated, socio-economically underdeveloped, and under-served communities in the country. 1 Of the total population, tribals comprise 14.75% in Gujarat, 86.15% in Meghalaya, and 1.10% in Tamil Nadu. 1
According to the Indian National Mental Health Survey (NMHS) 2015–2016, the overall weighted lifetime and current prevalences for any mental morbidity among adults were 13.7% and 10.6%, respectively. 2 The prevalence of mental morbidity among adolescents (13–17 years of age) was 7.3%. 2 Tribal populations are more vulnerable to communicable and non-communicable diseases due to their cultural practices and beliefs about health. 3 Rapid social changes alter their lifestyles, beliefs, and community living. The strain of acculturation on moving to urban spaces and the use of alcohol and other substances predispose them to many mental health issues. 4
India is home to the largest number of adolescents in the world, comprising about a fifth of its population (243 million). 5 During the past two decades, the prevalence of mental health disorders has increased considerably among adolescents. A meta-analysis reported that 6.5% of adolescents among community samples and 23.3% among school samples experienced significant mental health morbidity. 6
In a cross-sectional study of adolescent tribal girls (ages 10–19) from Jharkhand in Eastern India, 12% reported depression or anxiety. 7 High suicide rates are said to be a major public health problem among tribal adolescents.8,9 However, there is scant recent work on the extent and nature of psychiatric morbidity and substance use among tribal adolescents in India. The present study was conducted to estimate the prevalence of psychiatric morbidity and alcohol use disorders (AUD) and associated socio-demographic factors among adolescents in three different tribal communities in three widely differing states of India.
Methods
Study Design
This cross-sectional study was conducted in tribal blocks of three Indian states.
Study Settings
The study was conducted in tribal blocks served by a Government Medical College in Gujarat, a university-based site in Meghalaya, and a well-established Healthcare NGO in the Nilgiri Hills, Tamil Nadu. These sites were chosen considering their significant tribal population and socio-cultural and geographical differences between the sites (western, eastern, and southern parts of India).
Sample Selection
Valsad (Gujarat): The participants were recruited from the Dharampur and Kaprada blocks of Valsad district as these have a predominantly (more than 90%) tribal population, 10 but the samples were selected only from the indigenous tribal communities residing in the study area. The major tribes found in these districts are Bhils, Kharva, Nayakas, Dhodiya, and Halpati. From a total of 235 villages in the Dharampur and Kaprada blocks, we selected 30 villages by simple random sampling. The number of participants selected from each village was according to the probability proportional to the sample size (PPS) method based on the village population.
Tamil Nadu: Participants were recruited from the tribes of the Gudalur and Pandalur Taluks of the Nilgiris District. Participants were from four tribes: Mulakurumbas, Betakurumbas, Paniyas, and Kattunayikans and were recruited through cluster random sampling. The membership of a specific tribe and the difficulty in accessing their villages were the two parameters used for the sampling.
Meghalaya: The tribe sampled were the Khasis residing in the East Khasi Hills District, which has around 55% rural population (as per the 2011 census). Of the total estimated sample size of 200, 89 were drawn from urban and 111 from rural areas. The eight blocks were considered strata, and two wards/villages from each block were selected using the lottery method. The number of participants from each ward/village was determined using the PPS sampling technique.
Data were collected between January and February 2019 for Gujarat and Tamil Nadu sites. For Meghalaya, data were collected between February and July, 2019. The detailed methodology has been published. 11
Sample Size
According to the NMHS of India, 2015–2016, 2 7.3% of 13- to 17-year-old adolescents have psychiatric morbidity. Considering this prevalence of 7.3% of psychiatric morbidity, 95% level of confidence, 12 and design effect of 1.5, the required sample size was 156. Further, considering 20% non-participation, non-response, and attrition rates, the final sample size was 188, which was rounded off to 195 from each site.
Inclusion and Exclusion Criteria
Adolescents in the age-group of 11–19 years were included. Those with known developmental disorders were excluded. The developmental disorders were screened by Rashtriya Bal Swasthya Karyakram (RBSK) medical officers by visiting schools and Anganwadi centers. This is their regular activity. Those screened positive were referred to pediatricians and psychiatrists for further management, as per government protocol.
Procedure
In Gujarat, the District Health Department was informed about the study’s objectives and methodology for data collection. Then, the data collection team, with the support of the staff of Primary Health Centers (PHCs), personally contacted villagers and started a door-to-door survey. In Meghalaya, the headman of the village was informed about the study and recruitment of participants from the village. Then, the data collection team collected the information through a door-to-door survey. In Tamil Nadu, the NGO has been serving this tribal area for decades, and thus, they had established a good rapport with the population in the area. After selecting the villages, the data collection team conducted a door-to-door survey.
After obtaining written informed consent or assent as appropriate, from the parents and the participants, the interviews were conducted in private spaces like separate rooms inside the house, under a tree, or on the premises of a school or temple, to maintain privacy. Confidentiality and privacy were maintained throughout the interview process. Socio-demographic and clinical details, such as age, gender, religion, education, occupation, marital status, presence of Below Poverty Line (BPL) card, comorbid medical and psychiatric illness, and details of ongoing treatment, were collected using a semi-structured questionnaire. The MINI International Neuropsychiatric questionnaire (MINI 6.0) and the MINI KID 6.0 were administered to 18–19-year-old and 11–17-year-old participants, respectively, at each site to assess psychiatric morbidity. MINI 6.0 and MINI KID 6.0 were chosen to make our data comparable to the findings of the NMHS 2015–2016, 2 which used the same tools. The copyright permission to use the MINI 6.0 version was obtained from author Dr David Sheehan.
The field investigators were trained by the Principal Investigators and the Psychiatrist working at the study sites on how to collect the data and fill relevant information in the questionnaire. They were also trained to develop rapport, maintain privacy while asking questions, and note down the information. The data was collected on the paper format questionnaire.
Diagnostic Interview Schedules
MINI: With an administration time of approximately 15–20 min, the MINI is a short structured diagnostic interview developed jointly by psychiatrists in Europe and America to diagnose psychiatric disorders according to ICD-10 and DSM-IV.13-15 The MINI 6.0 includes 17 Axis-1 disorders (which have at least 0.5% prevalence as per NCS/ECA survey), 16 one axis- 2 personality disorder (antisocial personality disorder), and a suicidality module. The instrument has been translated and validated into 30 languages. 17
MINI KID: The MINI KID is the version of the MINI for use among children and adolescents up to 17 years of age.
At the Gujarat Site, the authorized Gujarati version obtained from MAPI Research Trust, Paris, was used. At the Meghalaya site, the data collection team used the original English version, as most participants could understand English. For the few who did not understand English, experienced personnel with mental health and social work backgrounds did the forward translation of the MINI and MINI Kid questionnaires into the Khasi language. A bilingual faculty did the back translation of the same. A Khasi psychiatrist then vetted the appropriate use of mental health terms. In Tamil Nadu, the wide variety of dialects used by the sample population and time constraints precluded systematic translation. Instead, staff experienced in communicating with the population used Tamil to communicate, which was also understood by the people.
The study was approved by the respective Institutional Ethics Committees of the three sites.
Data Analysis
The classification of psychiatric disorders was done according to the ICD-10 criteria. The socio-demographic and clinical factors were calculated as percentages and frequencies. Univariate associations between psychiatric illness and socio-demographic/clinical factors were calculated using chi-square test. A p-value of <0.05 was considered significant. Data was analyzed using Epi info 7 software. 18
Case Definition
We used MINI 6 for defining ‘caseness’ (ICD-10 criteria). We then estimated any psychiatric morbidity by combining estimates for schizophrenia and psychotic disorders, depression and bipolar affective disorders, substance use disorders (except tobacco), panic disorders, social and agoraphobia, obsessive compulsive disorders, posttraumatic stress disorder, generalized anxiety disorder, anorexia and bulimia, suicide risk, and antisocial personality disorders.
Behavioral and emotional disorders are defined as per the ICD-10 Classification. Attention-deficit hyperactivity disorders, conduct disorders, and oppositional defiant disorder are assessed using MINI Kid 6.0.
Results
Six hundred twenty-three adolescent tribals participated in the study from all three sites (Gujarat n = 206, Meghalaya n = 222, and Tamil Nadu n = 195). Among them, 266 (42.7%) were in the 11–14 age-group, while 357 (57.3%) were in the 15–19 age-group. The distribution of participants according to sex was similar (males: 300; females: 323); 519 (83.3%) participants were studying in school during the time of the survey, 49 (12.2%) were employed (working full time), 606 (97.3%) were single, 398 (63.9%) were living in nuclear families, and 154 (74.8%) had BPL cards. Site-specific socio-demographic data are shown in Table 1.
The sample was balanced in terms of age and sex but overwhelmingly from poorer socio-economic strata. Most were unmarried, studying (possibly full-time), and had 1-2 siblings. Two-thirds lived in nuclear families.
Distribution of Participants According to Socio-demographic Variables.
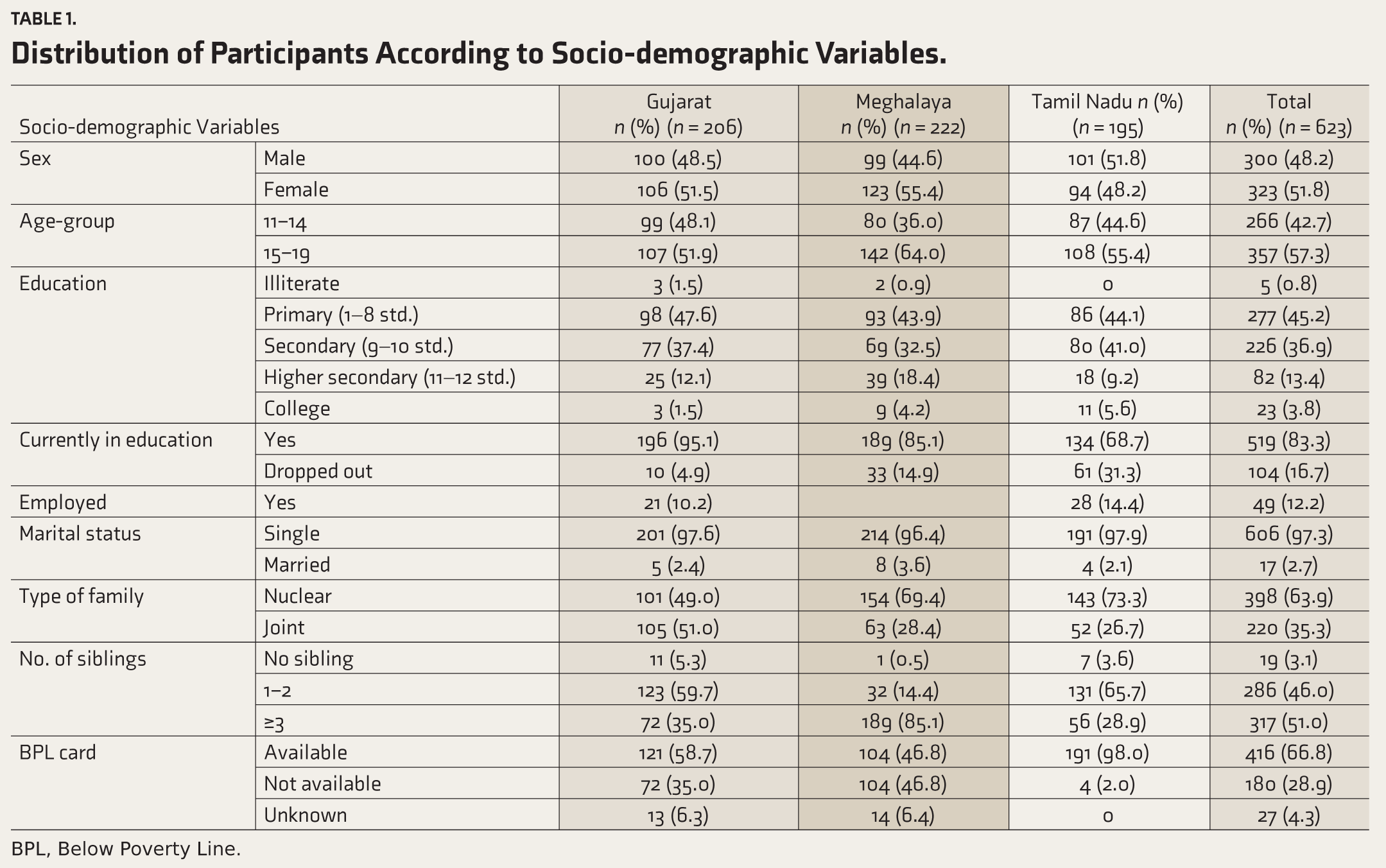
BPL, Below Poverty Line.
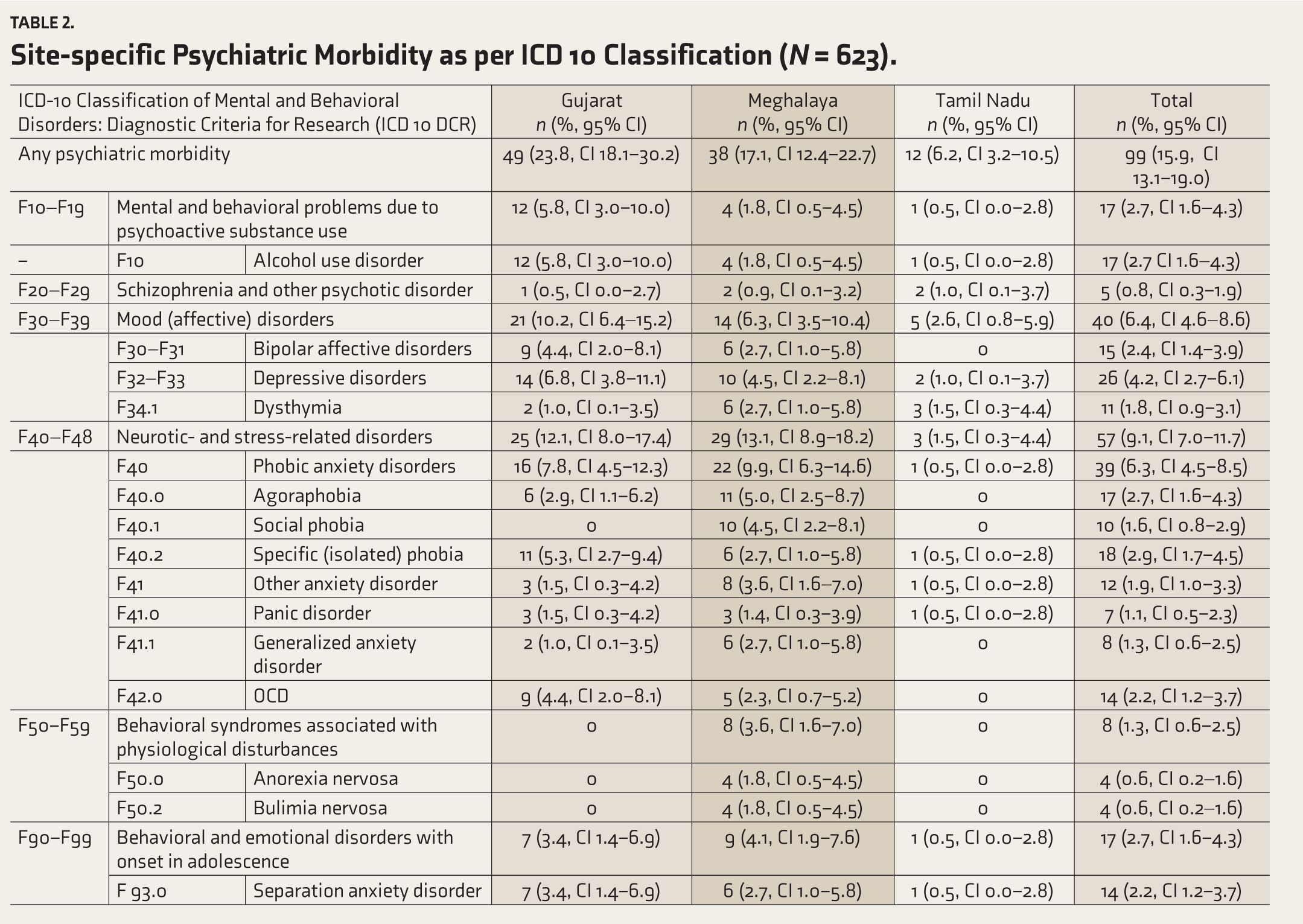
The prevalence of any psychiatric morbidity was 15.9% (95% CI: 13.1–19.0, Table 2) in the aggregate population; the highest in Gujarat, 23.8%, 95% CI: 18.1–30.2, (n = 49), followed by 17.1% (95% CI: 12.4–22.7) at Meghalaya (n = 38), and 6.2% (95% CI: 3.2–10.5) at Tamil Nadu (n = 12). Among psychiatric disorders, the prevalence of mental and behavioral problems due to psychoactive substance use (alcohol) was 2.7% (95% CI: 1.6–4.3, n = 17); mood disorders was 6.4% (95% CI: 4.6–8.6, n = 40); neurotic and stress-related disorders was 9.1% (95% CI: 7.0–11.7, n = 57), behavioral and emotional disorders were 2.7% (95% CI: 1.6–4.3, n = 17). The site-specific proportion of psychiatric morbidities is shown in Table 2.
Site-specific Psychiatric Morbidity as per ICD 10 Classification (N = 623).
Psychiatric morbidity was higher among girls (58.6%) and in the 15-19, that is, older, age-group (66.6%, Table 3). In our aggregate sample, exploratory analyses revealed significant associations between any psychiatric morbidity and the 15–19-year age-group (OR 1.38; 95% CI: 1.02–2.5) and being currently studying (OR 4.37; 95% CI: 1.85–12.47) or employed (OR 2.58; 95% CI: 1.26–5.13, Table 3). Morbidity was much higher among those living in nuclear families (n = 59) because our sample was skewed in terms of nuclear families.
Association Between Socio-demographic Profile and Psychiatric Morbidity Across the Three Sites.
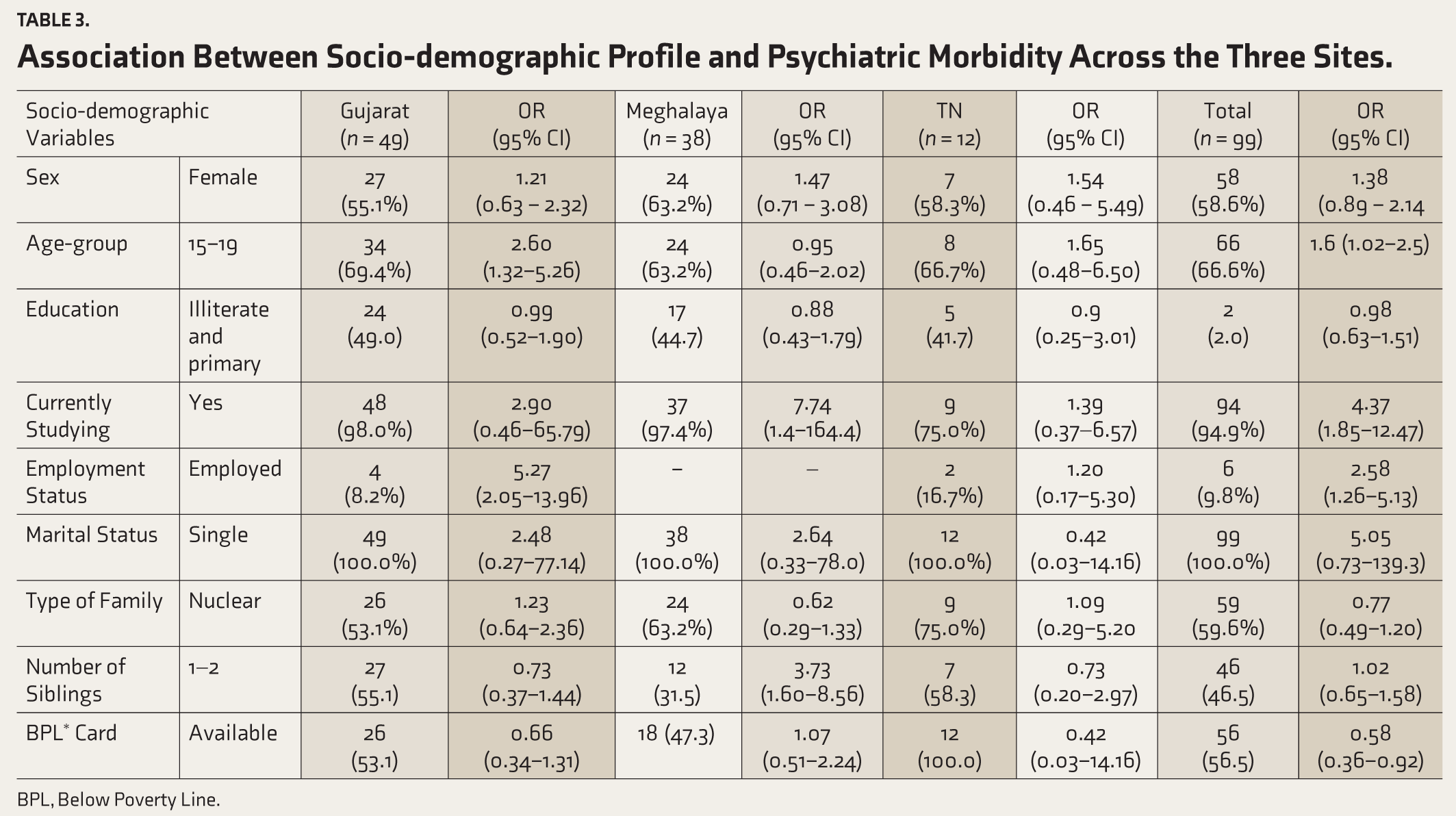
BPL, Below Poverty Line.
Discussion
The prevalence of any psychiatric morbidity was 15.9%. India’s NMHS conducted in 2015-2016 among 13–17 years old in four states (Gujarat, Tamil Nadu, Kerala, and Uttar Pradesh) of the 12 NMHS sites reported the prevalence of any psychiatric morbidity at 7.3% (95% CI: 5.8-8.7). This is around half of the prevalence found in adults in the same study of 13.67% (95% CI: 13.61–13.73). 2 Similar to NMHS results, the prevalence of psychiatric disorders among 11-17 years old adolescents in rural South India was 6.7%. 19 Our study differs from the above studies in that it involved a wider age-group (11–19 years) and focused on the tribal population alone. The prevalence of any psychiatric morbidity among the adolescent tribals in our study was 15.9%, which is considerably higher than in both of the above surveys. This might be related to our broader age-group, due to the increased prevalence of psychiatric morbidities in the indigenous population, or likely a combination of both these factors.
About ages, in a study from West Bengal, two-thirds (66.8%) of tribal adolescents in the age-group of 11–17 years were at substantial risk of developing of significant mental health problems due to different causes. 20 Our study found that the 15- to 19-year age-group was more vulnerable to mental illness, with 66.6% psychiatric morbidity while comprising 57.3% of the study sample. The higher prevalence in older adolescents could be related to exposure to the pressures of adult life, such as the need to support the family financially (around 10% of our sample was employed), the need to navigate personal relationships, loss of support related to schooling, and increased access to alcohol (2.7% of our sample had alcohol use disorder).
The prevalence of any psychiatric morbidity in our study was 13.6% and 17.9% in male and female adolescents, respectively. This was much higher than in the NMHS: 7.5% of any psychiatric morbidity among males (95% CI: 2.6–4.7) vs. 7.1% (95% CI: 2.6–4.7) among females, both sexes between 13 and 17 years of age. 2 However, an important difference would be that the NMHS focused on the general adolescent population, while our study focused specifically on tribal adolescents in the broader 11–19-year age-group. The challenges faced by the tribal populations are unique and might contribute an additional source of vulnerability to mental health issues. Our findings are similar to those reported by Pahwa et al., 21 who evaluated school-going 11-16-year-olds in Punjab and noted that the prevalence of any psychiatric morbidity in rural adolescents attending government schools (22.1%) was much higher than in those attending private schools in urban areas (17.6%) indicating the stressors that rural adolescents face. The same study noted that the overall psychiatric morbidity was higher in girls than boys (17.5% vs. 24.12%). 21 This is in accord with other studies that report a higher prevalence of psychiatric morbidity, especially mood and anxiety disorders, among adolescent girls. 22
The overall psychiatric morbidity was the highest in the Gujarat site at 23.8%, followed by Meghalaya at 17.1%, and Tamil Nadu at 6.2%. This could be reflective of the differences between the states themselves. According to the Government of India’s NITI (National Institution for Transforming India) 2019–2020 composite health index comparing the different states of India, Tamil Nadu stands second among the large Indian states in the overall composite health index (72.42), with Gujarat at 63.59, and Meghalaya at 43.05. 23 One plausible explanation for the difference is the wide socio-cultural and socio-economic difference among the tribals of the three states. According to the field experiences of investigators, we believe that tribal adolescents from Gujarat are more independent in decision-making and living independently, while the situation in Meghalaya and Tamil Nadu is different.
The prevalences of specific disorders in our study are comparable to the findings of NMHS except for the much higher prevalence of depressive episodes, recurrent depressive disorder, bipolar affective disorders, and phobic anxiety disorders. 2 This could be due to various social and cultural stressors faced by tribal adolescents, as detailed earlier in this section.
One in four Indian adolescents begin drinking before age 20, probably not amounting to AUD. 24 However, the prevalence of alcohol use disorder of 2.7% among adolescents in our study is moderately high, even though it is lower than the national average for adults, which is 4.7% (NMHS). Tribal populations in India historically do not have social taboos in relation to alcohol use, unlike mainstream Indian populations, and have used alcohol as part of cultural celebrations. Recent studies, however, indicate that tribals tend to use alcohol as a method to cope with distressing emotions. 25 This may explain the increased prevalence in the Gujarat site, which also had the highest overall psychiatric morbidity. Conversely, increased substance use could also be driving psychiatric morbidity. There was wide site-specific variation with Gujarat (a legally dry state where tribals may make their living from selling contraband alcohol), with 5.8% prevalence, followed by Meghalaya with 1.8%, and Tamil Nadu with 0.5%. For the Gujarat site, the data was collected from the Dharampur and Kaprada blocks of the Valsad district, which border the non-dry Maharashtra State. The availability of money with adolescents as they get jobs, social acceptance among tribals of alcohol use during festivals and marriages, and peer pressure about its association with “manly” image could be the reason for higher alcohol use disorder in Gujarat. The NMHS did not collect data on alcohol use disorder in the adolescent population. However, according to the National Survey on Extent and Pattern of Substance Use in India 2019, the prevalence of alcohol use among Indian adolescents (10-17 years of age) was 1.3%. 26 The low prevalence reported in the Tamil Nadu site could partly be due to under-reporting, caused by high levels of stigma and embarrassment regarding alcohol use in this community, even though every effort was made to ensure confidentiality. On a more positive note, there has been extensive education regarding the ills of alcohol use carried out by the health workers from one of the authors’ institutions in the Tamil Nadu site for over 20 years, and the reduced prevalence could reflect gains made from this approach. 2
Limitations
We did not estimate intellectual disability and developmental disorders, as the MINI 6.0 questionnaire does not cover these. Bias might have been introduced due to the study’s cross-sectional nature, elicitation of responses through interviews, and under-reporting due to stigma. There was variability in the methodology for selecting participants across the three sites due to geographical considerations. The study did not explore cultural and religious factors that might be an important link in the causation and treatment‑seeking behavior of the tribal population. It is also important to note that the prevalence of mental morbidity is likely under-reported in India, and the actual figures might be higher than those we have obtained. 27
Conclusion
The prevalence of psychiatric morbidity in adolescent tribals is twice as high as the national adult prevalence. The most common psychiatric morbidities reported were mood (affective) disorders, phobic anxiety disorder, alcohol use disorder, and obsessive-compulsive disorder. The prevalence of AUD among tribal adolescents is alarming and slightly lower than the national estimate for adults. Lack of awareness about the extent of psychiatric illness among tribal adolescents combined with a lack of services could lead to many tribal people not receiving the needed treatment. Concrete steps should be taken to educate about, identify, and address psychiatric morbidity. Future research on strategies to promote mental well-being and reduce alcohol use among adolescent tribals is crucial.
Footnotes
Acknowledgements
We thank Dr Soumya Swaminathan (then Secretary, Department of Health Research, DHR), Dr Balram Bhargav, Secretary DHR, Dr Ravinder Singh, and Dr Harpreet Singh of ICMR. We thank the faculty of “Cross-Fertilized Research Training for New Investigators in India and Egypt” (D43 TW009114, HMSC File No. Indo- Foreign/35/M/2012-NCD-1, funded by Fogarty International Centre, NIH). We are also thankful to National Coordinating Unit of ICMR for NMHP Projects for their constant support and guidance as well as to Dr Triptish Bhatia. We thank Data Management Unit of ICMR for designing the database.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This paper describes the results of a research project funded under ‘Capacity Building Task Force for Mental Health Research in India’ funded by the Indian Council of Medical Research vide file number 5/4-4/151/M/2017/NCD-1. International mentors were funded by the training program ‘Cross Fertilized Research Training for New Investigators in India and Egypt’ funded by FIC, NIH (No. D43 TW009114).