
Abstract
Chronic medical conditions in children and adolescents have a significant impact on development and quality of life. Children with vitiligo experience depression, anxiety and guilt, body image concerns, and conflicts of acceptance–rejection among peers. Understanding issues of relevance through a developmental perspective is pivotal. Here, we report the experiences of working with an adolescent who presented with depressive symptoms, mood dysregulation, and self-harm, in the background of vitiligo and child sexual abuse. We describe the unique therapeutic challenges, focusing on the interplay between depressive psychopathology, childhood trauma, and normative adolescent development. Therapeutic strategies for patient-centered psychological interventions are discussed. The therapy processes focused on a narrative approach, with the active involvement of the family.
Globally, the prevalence of vitiligo varies from 0.5% to 2%, and 50% have a prepubertal onset. 1 A confluence of internal and external psychological factors significantly impacts the onset, course, and outcome of the disorder, and the relationship is bidirectional. The course of the disorder has a significant impact on the normative developmental experiences. 2 Children with vitiligo experience depression, anxiety and guilt, body image concerns, and conflicts of acceptance– rejection among peers, and often undergo grief reaction. Parents of children with vitiligo face emotional issues due to blame-responsibility conflicts, need for an increased focus on childcare and treatment, and, notably, the intractable nature of the disorder itself. 3 Sociocultural considerations influence psychological and psychiatric comorbidities in this population. In a tertiary hospital setting in India, among patients with vitiligo, 56% were diagnosed with adjustment disorder, 22% had a major depressive episode, and 9% had dysthymia. 4
Here, we describe an adolescent with prepubertal-onset vitiligo presenting with depressive symptoms and self-harm, in the background of a loss of normative developmental experiences, early child sexual abuse (CSA), and conflicts related to autonomy in the treatment process. We also describe the complex interactions impacting her developing sense of self and identity and highlight the unique therapeutic challenges and strategies for patient-centered psychological interventions. Written informed consent and assent have been taken from the parent and the adolescent, respectively.
Case Summary
A 17-year-old girl, temperamentally sensitive to criticism and with difficulties in emotional regulation, the second born of nonconsanguineous parentage, presented with 2 years history of depressive symptoms and self-harm. She had persistent low mood, lack of interest in previously pleasurable activities, easy fatiguability, emotional dysregulation, suicidal ideations, episodes of prolonged anxiety, and multiple episodes of self-cutting, with an initial fluctuating course, followed by progressive worsening over the last 6 months. She had prepubertal-onset vitiligo (at age 12), with active progression in the initial years, followed by a predominantly static course over the last two years. She had a past history of alleged CSA by a known, extrafamilial perpetrator in the form of contact, nonpenetrative abuse over multiple occasions when she was 5 years of age.
As an early adolescent, she had negative experiences of peer rejection and bullying at school due to vitiligo. She underwent various treatment procedures for vitiligo, and multiple consultations were sought with a focus on “complete cure.” There was a shift in parenting style from authoritative to permissive, and adopting avoidance coping strategies to facilitate the resolution of vitiligo and provide a stress-free environment. She was restricted from activities of her interest, such as outdoor play, and was home-schooled for secondary education. She was denied the company of a pet, to prevent the worsening of skin lesions. There was an increased focus on her treatment for vitiligo, with the reorganization of family routines and priorities, resulting in self-blame in the adolescent. She also faced failure and rejection in the context of peer and romantic relationships.
According to the adolescent, repeated rejection in the context of peer and romantic relationships were due to her prominent vitiligo and the prevailing societal standards of beauty and appearance. Although she was passive during the initial years of treatment, during late-adolescence, she had grown up to “accepting vitiligo as part of herself” and refused to continue treatment, with a clear understanding of the future consequences. However, her parents continued to persuade her to seek treatment in her best interest. As per the adolescent’s perspective, she perceived a sense of rejection by her own family, where only the resolution of vitiligo and conforming to the societal norms would enhance acceptance and belonging.
Conflicts between the parents’ sense of responsibility and the adolescent’s emerging identity and need for autonomy resulted in strained interpersonal interactions in the family in the form of frequent verbal arguments, and emotional dysregulation in the adolescent, frequently culminating in deliberate self-harm. Anger toward parents, holding them responsible for current life events, and expecting an apology were the recurrent themes in the interpersonal interactions. There was a progressive worsening of emotional dysregulation, accompanied by persistent low mood and feelings of emptiness. Ongoing identity crisis, depressive symptomology, and interpersonal conflicts resulted in the resurfacing of the memories related to the past CSA. She had recurrent intrusive memories of the events related to the abuse, accompanied by negative emotional states, such as prolonged periods of intense autonomic arousal and emotional numbing. She also had persistent cognitions about the causes of the traumatic event, such as the parents having failed to protect her and not having taught her to understand and identify malicious intentions of the perpetrator when she was young. Disclosure of CSA to the family occurred in the context of the ongoing struggle to promote feelings of power and control and attaining a new sense of self.
Given her temperamental vulnerabilities and chronic medical illness, these experiences were perceived as significant losses, compounded by peer rejection and the discrepancy between her evolving self-concept and the expectations from her family. The timeline of the traumatic events resulted in intense struggles to attain a satisfactory representation of self and cognitive and social competencies, throughout her adolescence. On the one hand, her evolving identity comprised accepting her early childhood experiences of CSA and chronic medical illness as part of what defines her. On the other hand, she continued to have distorted views of the parent–child relationship because the parents had repeatedly failed to protect her from adverse experiences and also prevented her from exploring her identity.
Diagnoses of major depressive disorder and comorbid posttraumatic stress disorder (PTSD) were made as per the DSM-5 diagnostic criteria. The severity of depressive symptoms as assessed on the Children’s Depression Rating Scale (CDRS) was 50, indicating moderate severity. On the Clinical Global Impressions-Severity scale, she was rated as moderately ill, with a score of 4. Given the duration and severity of the depressive symptoms, a combination of psychotherapeutic and pharmacological interventions was planned. The case conceptualization and biopsychosocial formulation are provided in Figure 1 and Table 1. She was started on escitalopram 5 mg/day, titrated to 15 mg/day, carefully monitoring for side effects. Escitalopram was chosen as per recommendations for antidepressant choice in adolescents with major depression. 5
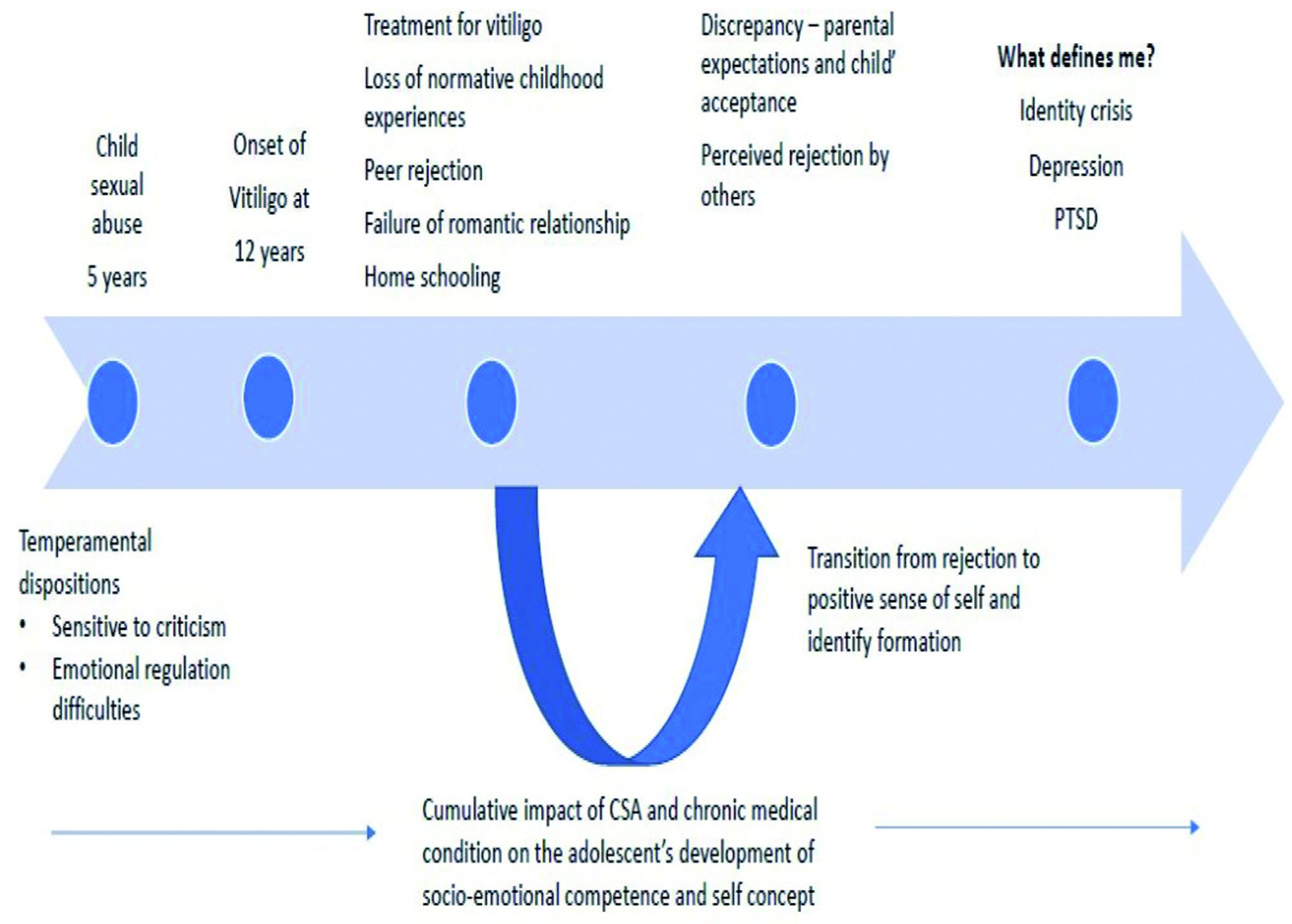
CSA: child sexual abuse; PTSD: post-traumatic stress disorder.
Biopsychosocial Formulation.
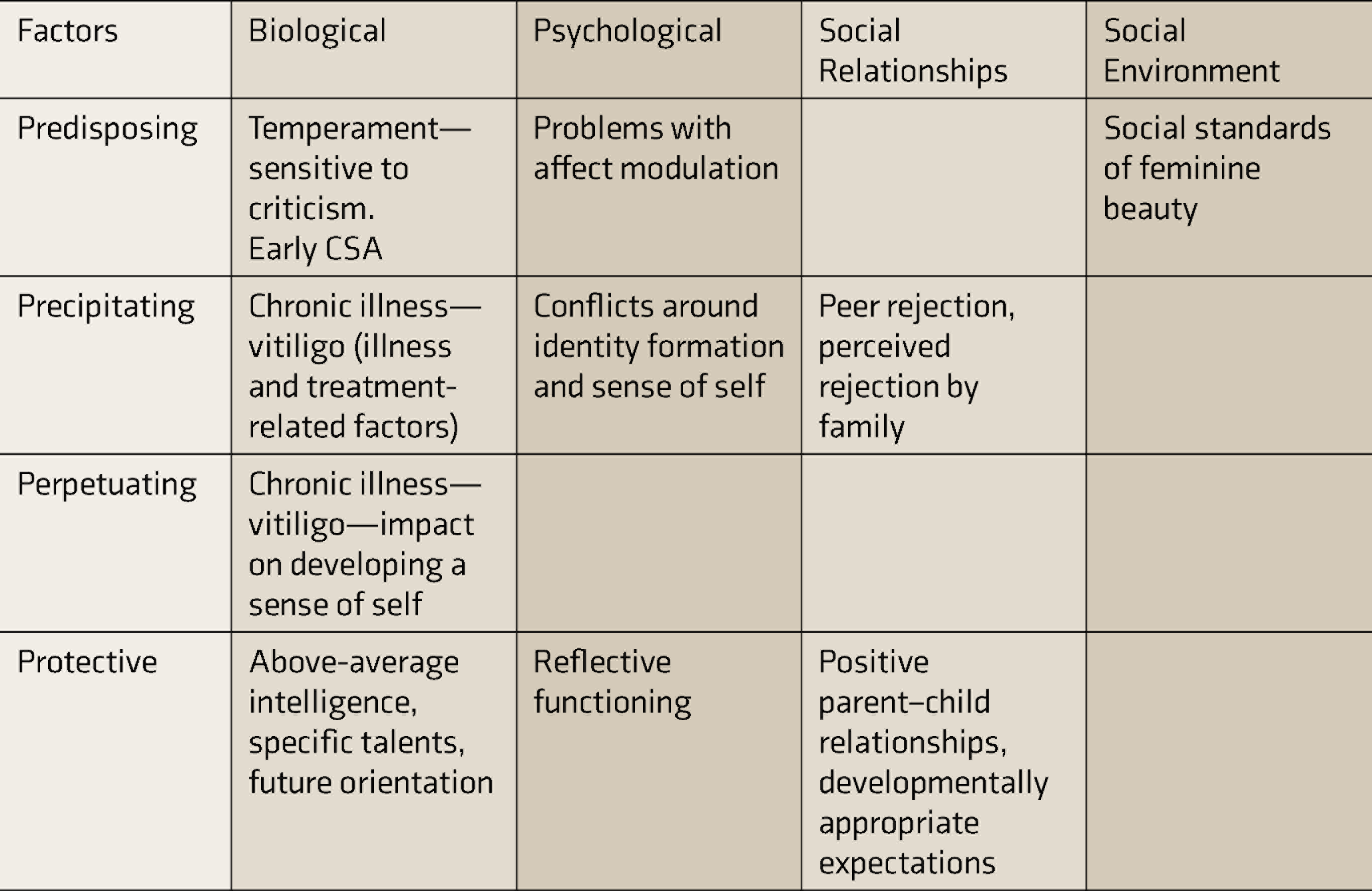
CSA: child sexual abuse.
Case Conceptualization
Stages of Intervention
Intensive psychotherapeutic interventions were done on an inpatient basis over 1 month. Following the initial assessment, diagnostic clarification, and case conceptualization, a framework for psychotherapeutic sessions was planned. A total of 15 sessions comprised ten individual sessions with the adolescent, two sessions with the parents focusing on psychoeducation and feedback, and three joint family sessions. The sessions lasted for 1 hour on average. This was followed by biweekly booster sessions on an outpatient basis, focusing on the maintenance of gains.
Individual Therapy with the Adolescent
Child-centered interventions focused on establishing rapport and understanding the child’s perspective of the loss experiences, by building both chronological and contextual narratives. Loss of normative childhood experiences, such as play, schooling, loss of a pet, romantic relationship, and peer rejection, was explored using a meaning-focused narrative approach. Therapeutic processes focused on (a) understanding what these contexts of loss meant to her in the past, (b) how she has processed the loss experiences by rationalizing, explaining, and comprehending them, and (c) what she can do about it in the present. The meaning related to the loss of developmental experiences transitioned from “I lost a normal childhood” to “integration of loss experiences in her identity” as reflected by the narratives. Similarly, the impact of vitiligo in the past and the child’s current experiences and meaning-making were explored through narratives. She had undergone a transition from passively accepting the vitiligo treatment to struggling for autonomy in treatment-related decision-making and “acceptance” of the condition. Empathetic listening and facilitating reflection were the primary therapeutic processes.
Emotional dysregulation and self-harm were contextualized; critical incidents were debriefed to understand the triggers, the child’s inner voice, and the consequent behavioral and emotional responses. Affective communication and emotional regulation skills were practiced in sessions and generalized to interpersonal interactions. Strategies such as role play and reflection on emotional response during critical incidents were used.
The contextual narratives surrounding vitiligo and CSA were different in terms of her current understanding and meaning-making. Narratives surrounding vitiligo transitioned from experiences of loss and powerlessness to empowerment and integration into an evolving sense of self. However, in relation to CSA, the current emotional responses reflect the conflicts between the persistence of the childhood understanding of abuse, such as the need to justify the abuse itself and self-blame, to the need to confront the perpetrator, in order to facilitate self-healing. Trauma work focused on eliciting trauma narrative, blame reduction, and promotion of integration and mastery over trauma with the help of scenarios. Workbooks were used to complement the narrative framework. 6 The process of CSA disclosure was facilitated during the family sessions. The parental response was sensitive and nonblaming, and they encouraged the child’s help-seeking.
Work with the Family
Joint sessions with the family explored their attitudes and expectations regarding vitiligo and the treatment process and its impact on the child’s mental health and interpersonal interactions, using circular questioning and reflection. The dissonance between acceptance and outcome-oriented expectations were elicited and addressed. The importance of balancing the child’s autonomy and active parental decision-making, and the expected collateral improvement in the child’s functioning and family relationships were discussed. Building alternative narratives for scenarios like a childhood without vitiligo, appropriate opportunities for normative developmental experiences, various outcomes of current treatment-related decisions down the lane, and possible emotional consequences in the future were done using hypothetical scenarios projecting into the future.
Outcome
At the end of 1 month, the adolescent showed a significant improvement in depressive symptoms, mood dysregulation, and self-harm behavior and used adaptive strategies in interpersonal communication. This was reflected in the reduction in CDRS scores from 50 at baseline to 36 at 1 month and 32 at 3-month follow-up. On the Clinical Global Impressions-Improvement scale, she scored 2, “much improved.” Parental attitudes and understanding had improved, and they adopted participatory and collaborative decision-making regarding her treatment and improved interpersonal communication. She maintained the improvement at 3-month follow-up and continued to function well.
Discussion
The literature on psychocutaneous disorders report significant psychiatric comorbidities and integration of medical and psychological interventions are extensively studied. 7 This adolescent presented with unique challenges; depression and PTSD were precipitated by the identity crisis and perceived rejection by the family, compounded by early CSA. From a developmental perspective, CSA has a significant impact on socioemotional development, perception of self and others, and a sense of agency.8,9 The timeline and the nature of the traumatic events have had a cumulative and bidirectional impact on the developing self-concept and identity formation.
Understanding the emotional issues in children with chronic medical conditions through a developmental perspective and the context is essential. Collaborative goal setting, contextualizing symptomatology, and establishing a therapeutic alliance are the cornerstones of therapeutic work with adolescents. Therapeutic strategies for the current case borrowed principles from narrative therapy. The narrative framework was used to facilitate understanding and reflecting on her experiences and navigate toward the process of healing. Both CSA and vitiligo were significant traumatic events impacting her self-identity. The therapy processes focused on putting together a narrative, blame reduction, building alternative narratives to facilitate meaning-making, and reauthoring, establishing, and reestablishing identity.
Patient-centered psychological interventions and active involvement of the family in the therapeutic process are pivotal for effective and sustainable gains. From a sociocultural viewpoint, parental responsibilities and societal expectations were in disagreement with the child’s perception of self. The therapy process focused on a child-centered perspective, prioritizing respect, dignity, autonomy, and her rights. Mobilizing family support systems, restructuring interpersonal interactions, and reframing acceptance, with the adolescent’s well-being as the central focus, helped facilitate the change process.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.