
Abstract
Introduction:
Sialorrhoea, or excessive salivation, is common in psychiatric patients. This can be distressing because of its physical and psychosocial complications. Sialorrhoea due to psychotropic drugs has been reported repeatedly in the literature. Clozapine is the antipsychotic most commonly associated with sialorrhoea.
Objective:
The objective of this review was to examine and discuss the existing literature on all psychotropic drugs associated with sialorrhoea, except clozapine.
Methods:
Google Scholar and PubMed were searched for the literature on psychotropic-induced sialorrhoea. The search terms used were sialorrhoea, antidepressants, antipsychotics, mood stabilizer, and benzodiazepines. Case reports on patients suffering from psychotropic-induced sialorrhoea except clozapine are reviewed in this study.
Results:
The pathophysiology behind psychotropic-induced sialorrhoea, the population susceptible to sialorrhoea, and the exact duration from the start of sialorrhoea the drug course to the onset of sialorrhoea are unknown. Also, sialorrhoea is not associated with drug toxicity and is observed even in patients receiving normal doses of psychotropic medications. Treatment involves dose reduction, discontinuation of drugs responsible for the adverse effect, or adding anticholinergic drugs.
Conclusion:
Sialorrhoea due to clozapine has been reported in the literature. Many other antipsychotics, antidepressants such as sertraline, and other psychotropic drugs such as lithium have also been reported to cause sialorrhoea. No increase in the risk of sialorrhoea was seen in any of the age groups, and no association was found with treatment duration. In cases of lithium-induced sialorrhoea, no relationship was observed between serum levels of lithium and sialorrhoea.
Psychiatric medications have significant side effects that range from common to rare, including extrapyramidal symptoms; metabolic, 1 cardiovascular, and psychosexual side effects 2 ; as well as tremors, gastrointestinal disturbances, Steven Johnson’s Syndrome, etc. 3 Sialorrhoea is a rare side effect of many psychotropic drugs. 4
Sialorrhoea, also known as drooling or excessive salivation, is an embarrassing side effect encountered in psychiatry patients. Factors contributing to this adverse effect include hypersecretion of saliva, dental malocclusion, postural problems, and an inability to recognize salivary spill. It can cause physical and psychosocial complications, including perioral chapping, dehydration, odor, and social stigmatization, which can be devastating for patients and their families. 5
Many psychotropic drugs, such as clozapine, olanzapine, risperidone, quetiapine, aripiprazole, and lithium, cause sialorrhoea as a side effect. 4 Hypersalivation due to clozapine has been reported many times in the literature. 6 In this study, we have reviewed the literature on psychotropic drugs causing sialorrhoea, except clozapine.
Materials and Methods
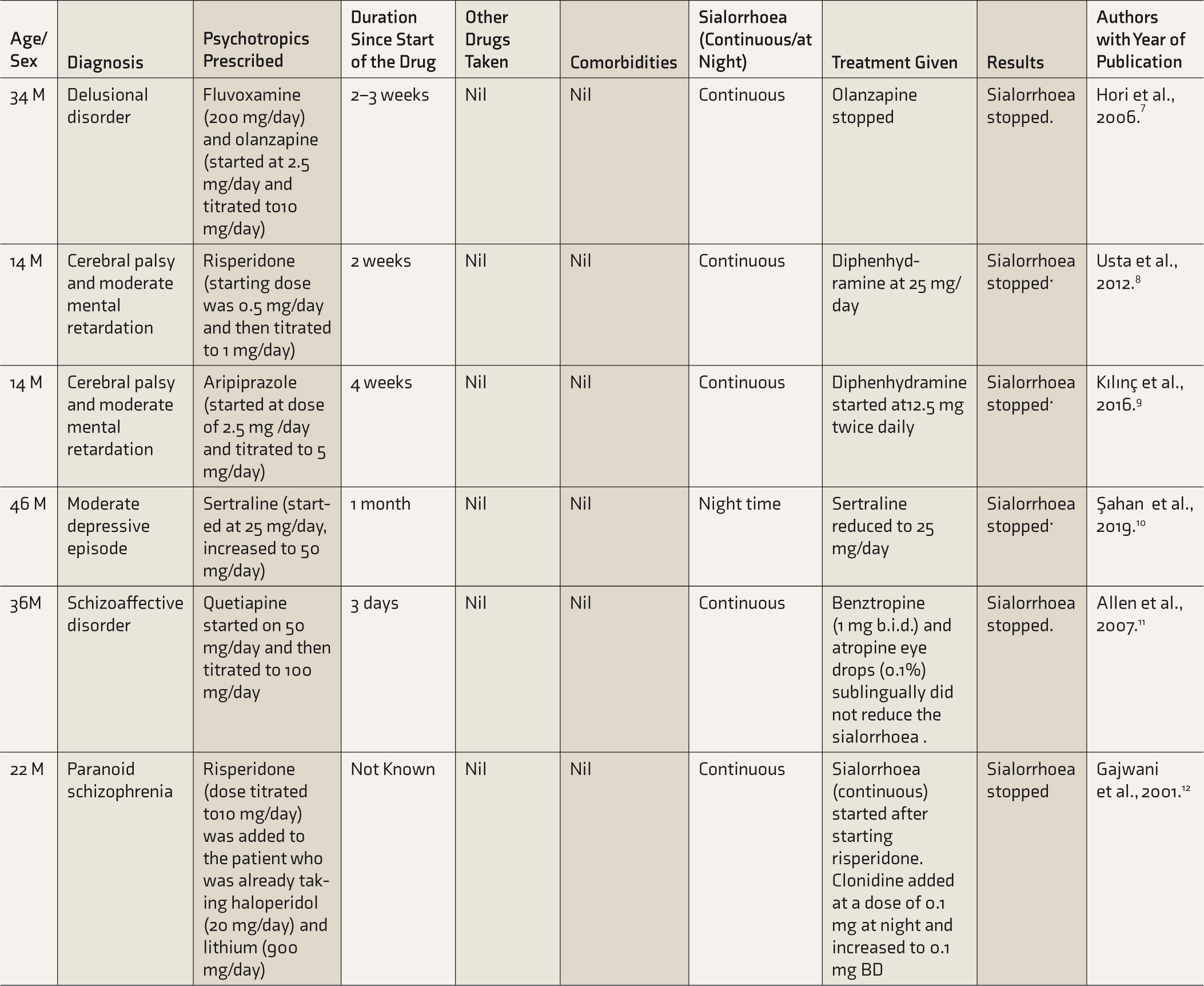
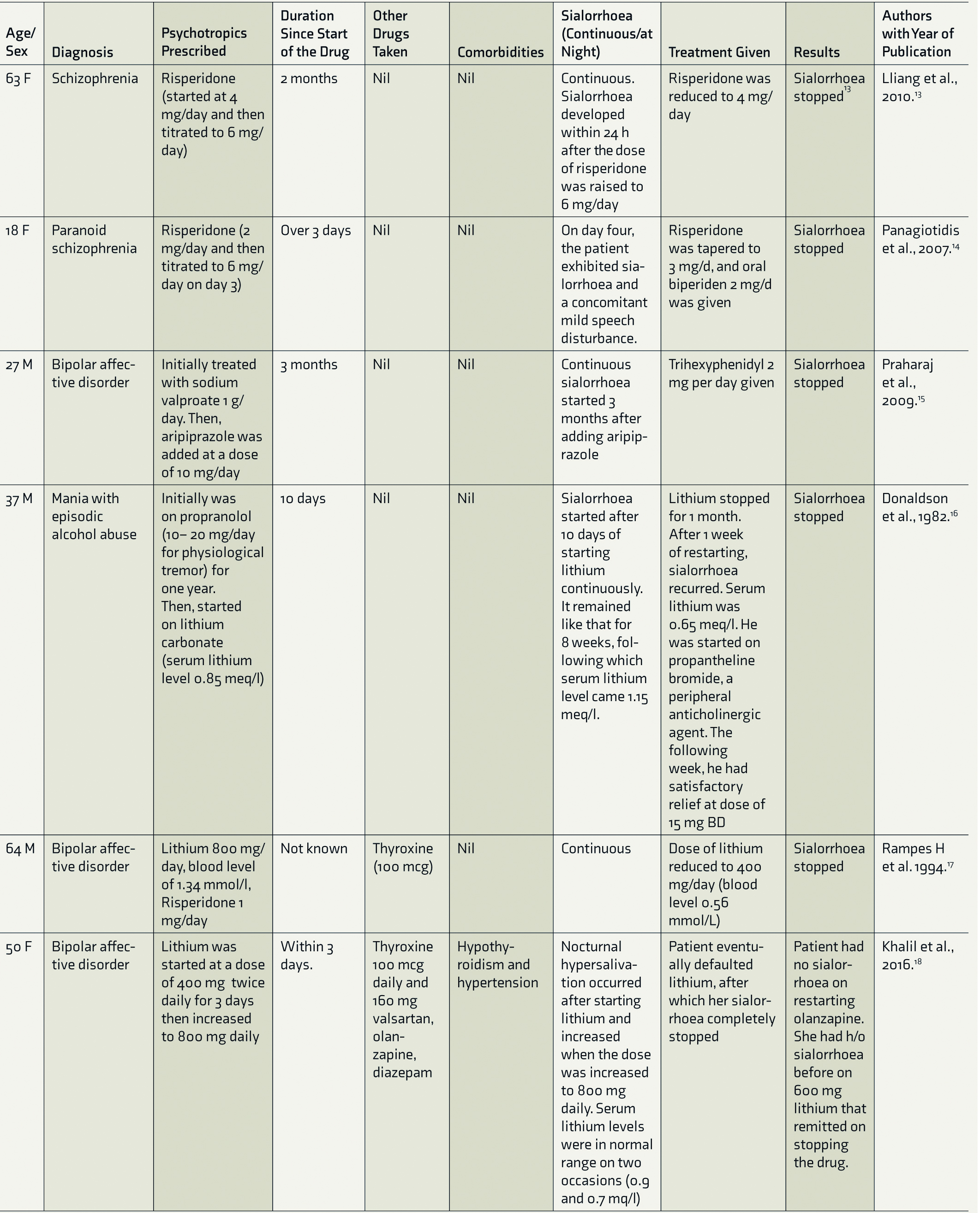
Google Scholar and PubMed were used to search for the literature on psychotropic-induced sialorrhoea, from January 23, 2021 to March 25, 2021. The search terms used were sialorrhoea, sialorrhoea, antidepressants, antipsychotics, mood stabilizers, and benzodiazepines. The search resulted in a list of 236 articles. Eighty-three articles related to clozapine-induced sialorrhoea were excluded. One hundred forty-one articles were excluded as they were not related to the topic of interest. Case reports on patients suffering from psychotropic-induced sialorrhoea except clozapine were reviewed in this study (Table 1).
List of Case Reports on Sialorrhoea Induced by Psychotropics Other Than Clozapine
Results and Observations
Demographic characteristics of the Cases Included in This Review
Age Group
Five patients belonged to the age group of 10–30 years, five patients were aged between 30 and 60 years, and two patients were >60 years of age.
Duration of Treatment With Psychotropics and Onset of Sialorrhoea
In 7 out of the 12 reported cases, sialorrhoea was reported in 30 days since the start of treatment, whereas 4 patients reported after 30 days of treatment onset.
Comorbid Conditions in Patients With Psychotropic-Induced Sialorrhoea
Only 1 out of the 12 cases had comorbid conditions. The patient had comorbidities such as hypothyroidism and hypertension.
Concomitant Medications
One of the cases received thyroxine and valsartan as concomitant medications.
Treatment of Sialorrhoea
In three patients, sialorrhoea stopped after discontinuation of the psychotropic drugs, including aripiprazole, olanzapine, and lithium. Three patients reported no sialorrhoea after the dosage of drugs such as risperidone, lithium, and sertraline was reduced. In five patients, sialorrhoea improved on treatment with one of the following drugs: propantheline bromide, trihexyphenidyl, clonidine, benztropine, atropine, and diphenhydramine. In one patient, risperidone was tapered down and biperiden was added.
Pathophysiology of Sialorrhoea
Saliva formation and secretion is considered to be a two-step process.19,20
Stage 1. Secretion of the isotonic plasma-like primary saliva fluid occurs in the acinar cells. A functional coupling mechanism operates between salt and fluid secretary processes. Ion channels and transporter leads to a vectorial ion transport from the serosal (basolateral) to the luminal (apical) side. Transcellular secretion of Cl facilitates movement of water.
Stage 2. The NaCl-rich fluid is modified as it passes along the duct system, where most of the NaCl is reabsorbed, and KHCO3 is secreted.
The end product is saliva, which is usually hypotonic. This is due to the poor permeability of the ductal epithelium to water and, moreover, higher NaCl reabsorption compared to KHCO3 secretion.
Salivation is controlled by the autonomic nervous system and increases with either sympathetic or parasympathetic stimulation. However, prolonged sympathetic stimulation eventually decreases salivary flow because of vasoconstriction. Salivation can be increased by local or central stimulation. Local stimulation involves mechanical or chemical stimulation, such as taste or chewing. Central stimulation is by stimulating the chemoreceptor emetic zone with drugs such as apomorphine or picrotoxin. Also, there is some evidence suggesting that aldosterone increases the volume of saliva. 21
Lithium-Induced Sialorrhoea
In cases of lithium-induced sialorrhoea, normal serum lithium levels around 0.85 meq/l 16 and 0.9 meq/l 18 were associated with sialorrhoea. Lithium-induced sialorrhoea also occurred in serum levels of lithium toxicity. 17
Another report suggested that lithium levels in the serum are directly proportional to the severity of sialorrhoea. 22
Lithium levels affect the catecholamine metabolism in the central nervous system but have no effects on the peripheral nervous system.22,23,26,27 The secretion of lithium ions in the saliva is known to cause persistent localized irritation. 23 Lithium is also known to trigger the central chemoreceptors in the emetic zone. 22 Lithium is reported to produce a transient rise in urinary aldosterone, which increases salivation. 22 Another possibility is the direct effect of lithium on salivary gland secretion. 22
Antipsychotic-Induced Sialorrhoea
Antipsychotic drugs such as clozapine are known to cause sialorrhoea via the blockade of alpha-2 adrenergic receptors or decreased noradrenaline and direct agonism of M3 and M4 muscarinic receptors.8,10,24 Sialorrhoea occurs in 30%–80% of patients with schizophrenia receiving clozapine.6,25,26 Patients receiving other antipsychotics, such as risperidone, aripiprazole, olanzapine and quetiapine, have also reported sialorrhoea.7,8,9,11
Antidepressant-Induced Sialorrhoea
In one of the cases, sialorrhoea occurred due to sertraline. 10 No specific mechanism behind sertraline-induced sialorrhoea was hypothesized. 10 Effect of selective serotonin reuptake inhibitors, such as fluoxetine, paroxetine, sertraline, and citalopram, on the content and flow of saliva has been studied,27–29 for a variety of reasons: first, association between dry mouth, halitosis, and oral candidiasis; second, inadequate salivary film leading to impaired retention of dentures; and third, the lack of salivary lubrication leading to denture-induced mucosal ulceration. 29
Patients using these drugs were shown to produce the same amount of saliva or less in comparison to healthy individuals, but due to dry mouth, noncompliance with antidepressant treatment was observed.27–29
Sialorrhoea as Adverse Drug Reaction of Psychotropic Drugs
Earlier studies, including Phase 3 of the Clinical Antipsychotic Trials for Intervention Effectiveness (CATIE), 30 revealed sialorrhoea in 38% of patients on clozapine and <12% of those on other antipsychotics such as aripiprazole, olanzapine, risperidone, and quetiapine.
In some cases, benzodiazepines may cause drooling, indicating a change in the underlying swallowing process due to excessive sedation, particularly at high doses. 31
Coming to antidepressants and lithium, sialorrhoea as an adverse effect was not mentioned in side effect profiles of these drugs.31–33
Conclusion
Sialorrhoea is an embarrassing side effect that can affect the personal, social, and occupational aspects of life. Sialorrhoea due to clozapine has been reported in the literature in case reports and studies. Other antipsychotics, antidepressants such as sertraline, and other psychotropic drugs such as lithium have also been reported to cause sialorrhoea. In this review, we focused on sialorrhoea caused by psychotropic drugs other than clozapine. No particular commonality (such as age and duration of treatment) was found between the cases reviewed. In cases of lithium-induced sialorrhoea, no relationship between serum levels of lithium and sialorrhoea has been reported. Multiple hypotheses for pathophysiology of psychotropic-associated sialorrhoea were proposed. On presentation with sialorrhoea, adding an anticholinergic agent and down-titrating or discontinuing the drug may prove beneficial.
Limitation of this manuscript is that it reviews only case reports. Monitoring sialorrhoea while starting psychotropics or while increasing the dosage and further research on the pathophysiology of sialorrhoea will aid in the better management of psychotropic-associated sialorrhoea.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.