
Abstract
Background and Objectives:
Medical illnesses seen in persons with psychiatric disorders are important but often ignored causes of increased morbidity and mortality. Hence, a community level intervention program addressing the issue is proposed.
Materials and Methods:
Patients with severe mental illnesses will be identified by a door-to-door survey and assessed for comorbid physical illnesses like anemia, hypertension, diabetes, and so on. They will then be randomized into two groups. The treatment as usual (TAU) group will not receive intervention from the trained community level workers, while the Intervention group will receive it.
Results:
The two groups will be compared for the prevalence and severity of comorbid physical illnesses. The expected outcome is compared to the TAU group, the intervention group will have a greater reduction in the morbidity due to physical illnesses and improved mental health.
Conclusion:
If successful, the module can be incorporated into the community level mental health delivery system of the District Mental Health Program (DMHP).
Physical illnesses are very common in people with severe mental illness. But they are often ignored. Hence a community level intervention program is needed to address them.Key Messages:
Background and Rationale
Several epidemiological studies have focused on prevalence of specific mental disorders (psychoses, substance use, etc.) or related behaviors (suicide).1,2 However, the prevalence of physical illnesses in persons with mental disorders has not been examined in any detail in India. The few studies done have been limited to hospital settings while none have been reported from the community.3–5 Life expectancy of a person with mental illness is approximately 10–15 years lower than the general population. 6 It is critical to examine factors related to physical health which could contribute to this increased mortality. It is highly likely that individuals with severe mental disorders (psychoses, bipolar affective disorders, dementia, etc.) do not use health services or use them irregularly, and hence are frequently under diagnosed for their physical health conditions and do not receive appropriate care. 7 In addition, people with mental disorders have poor compliance to treatment and frequently drop out of care for their physical disorders as they do for treatment of mental disorders.8,9 However, there is no clear data available as of date in Indian settings regarding the prevalence of physical comorbid conditions in those with mental illness and their treatment status in the general community.
Given the limitations in the availability of trained health personnel in India, especially in rural communities, it is imperative to use task shifting strategies to widen the reach of health services. 10 Use of lay community level health workers (CHWs), after some basic training, has proven to be an effective strategy to increase coverage of health services and has also been successfully utilized to deliver mental health care in both rural and urban communities.11–15 CHWs have been used to screen and identify patients and deliver home- and community-based care which has proven effective in improving the health of the patients. A multicenter, parallel-group, randomized controlled trial at three sites in India found that collaborative community-based care plus facility-based care intervention is modestly more effective than facility-based care, especially for reducing disability and symptoms of psychosis. 14
If a suitable model of care can be developed and its efficacy is proven, the intervention can be scaled up and replicated especially if it can be built into the existing public health system leveraging the existing resources such as the primary health center (PHC), the District Mental Health Program (DMHP), and so on.
Objectives
This study has been designed with the following objectives.
To train CHWs to identify physical health disorders in persons with mental illness
To compare intervention by CHWs with a treatment as usual (TAU) control group for whom no community-based interventions are offered
To study the differences in improvement in physical and mental health in both the groups
To devise a suitable mechanism by which these persons will access treatment facilities for both physical and mental health issues
Trial design: A population-based, cluster randomized trial.
Methods: Participants, Interventions, Outcomes
To meet the objectives of the study, two complementary designs will be followed. For case identification and estimation of prevalence, a population-based door-to-door, two-stage informant-based survey will be carried out in a geographically defined catchment area. For evaluating the effectiveness of the intervention program, a cluster randomized control trial will be carried out.
Study Setting
The study area is the catchment area of the PHC at the Kallur Village of Tirunelveli District in Tamil Nadu. Here, a Model Rural Health Research Unit (MRHRU) of the Indian Council of Medical Research (ICMR) has been established. A three-year cohort study of non-communicable diseases, risk factors, health-seeking behavior, morbidity, and mortality patterns has been completed (2015–2018). 16 The population of adults (age above 18 years) is 34,920 individuals. The entire adult population would form the study sample for the two-stage survey component of this study to estimate the prevalence of physical morbidity in mental disorders. The entire population is divided into 14 clusters.
Inclusion Criteria
Any person in the community diagnosed with severe mental disorder will be included in the study.
Survey and Instruments
A door-to-door, family informant-based, two-stage survey will be undertaken to identify those with mental illness and comorbid physical disorders.
Mental disorders screening: The CHWs will conduct the first stage of the survey wherein the initial screening using the General Screening Questionnaire (GSQ) of the Family Interview for Genetic Studies (FIGS) 17 will be done. Standard sociodemographic details will be collected and recorded. Personal and Psychiatric History Schedule (PPHS) 18 which will provide information on age of onset of illness, duration of illness, duration of untreated illness, pathways to care, and so on, will also be completed by the CHWs as part of the baseline data collection.
Confirmation of diagnosis: The diagnosis of mental illness is confirmed by a psychiatrist from the Department of Psychiatry Tirunelveli Medical College (TVMC). Individuals who have a positive score on the screening instrument will then be evaluated by a psychiatrist who will confirm the ICD-10 diagnosis using the M.I.N.I. International Neuropsychiatric Interview version 6.0. 19 The patient is either brought to the Department of Psychiatry, TVMC, or the psychiatrist who visits the PHC area fortnightly examines the person to confirm the diagnosis of those screened by the community worker. Severity rating of their illness will be assessed using the Clinical Global Impression (CGI—severity) 20 scale as part of the baseline assessment.
Physical disorders screening: All individuals with a confirmed diagnosis of mental illness will then be screened for physical disorders with the WHO STEPwise protocol. 21 Anthropometric parameters like height, weight, BMI (body mass index), and blood pressure will be measured. All the patients are brought to the PHC or the medical college hospital (TVMC). Blood investigations like hemoglobin, complete blood count, blood sugar, HbA1C, and lipid profile will be done.
Cluster randomization: Patients identified will be randomized into one of the two arms—TAU arm and TAU with intervention arm. In the TAU arm, the identified patient would be referred for appropriate care to the Kallur PHC and to the Department of Psychiatry, TVMC, and they will receive the standard treatment from these centers. In the intervention arm apart from the TAU, the patients will receive community-based intervention which will comprise regular visits from the CHWs who will provide inputs to the patients and families.
Intervention Module
An intervention module will be developed for CHWs considering both the mental health component and the physical disorders. The intervention module will be developed by the Departments of Psychiatry and Community Medicine, TVMC, in collaboration with the Schizophrenia Research Foundation, Chennai (SCARF).
The intervention training module will be made into a manual. According to the manual (which we plan to publish separately), the community worker needs to visit fortnightly, enquire about psychological and physical symptoms; conduct and record anthropometric measurements like weight, BMI, BP, pulse; time spent in exercise in the preceding week, adherence to medications both for physical illnesses and psychiatric illnesses. The manual also requires the worker to make weekly phone reminders and referral alerts in case of worsening of physical illnesses and mental illnesses.
Outcomes at the End of One Year
At the end of one year, TAU arm is compared with the arm that receives the intervention on the following:
Improvement in mental health as measured by CGI Improvement in physical health is defined as comparison of changes from the baseline of the following measures—weight and BMI for obesity, reduction in blood sugar values (fasting and post prandial), and HbA1C values for diabetes, blood pressure values for hypertension, reduction in triglycerides, and LDL (low density lipids) for hyperlipidemia.
The proposed activities of the entire protocol are given in Figure 1.
Flowchart of Proposed Activities
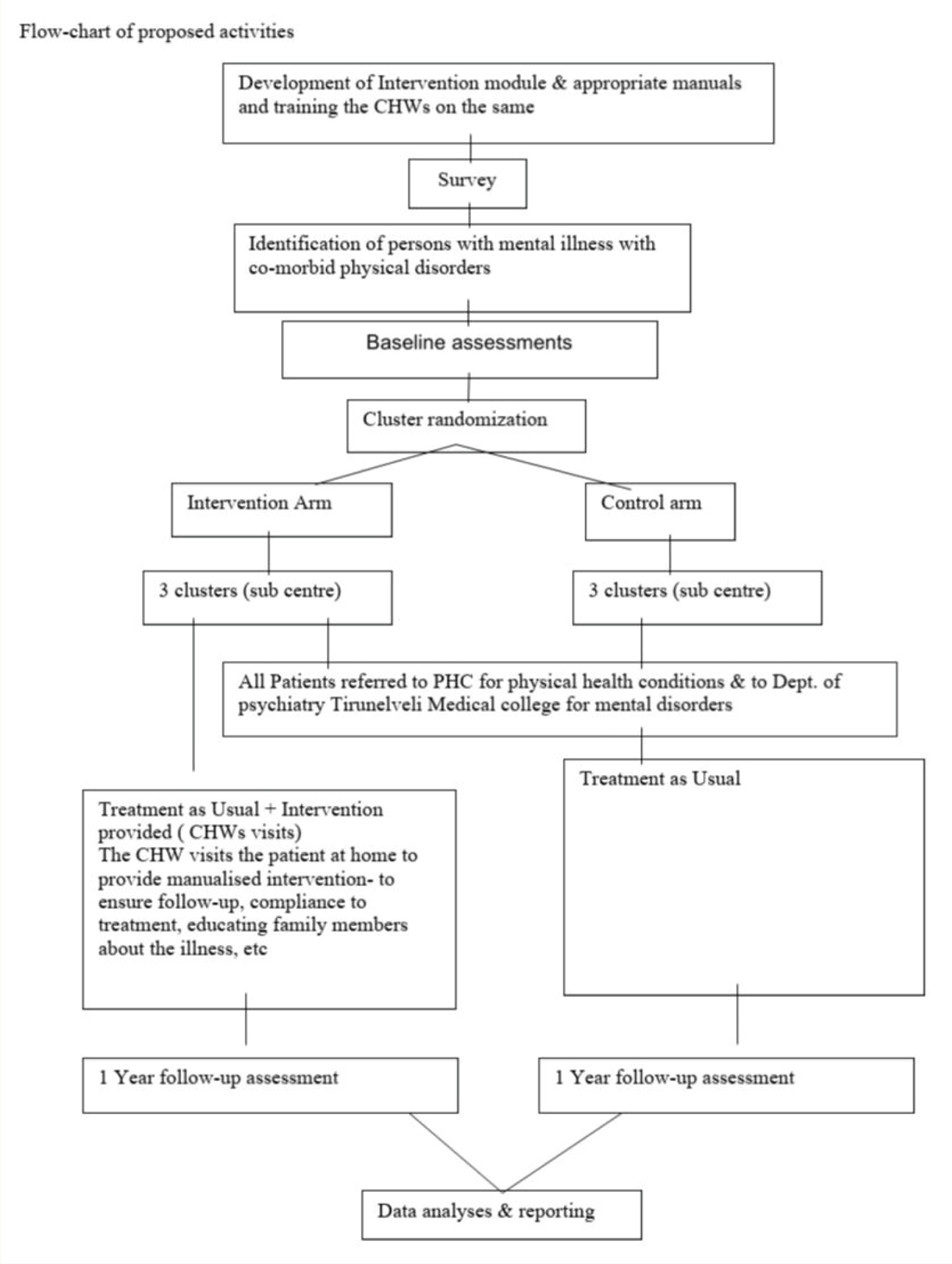
Blinding: Assessment of CGI and statistical analysis will be done by raters blind to the groups.
Study sample: The study area is the entire population under the cover of the MRHRU. About 37,920 people belonging to 11,000 families will be screened using key informant survey and the diagnosis of severe mental illness is confirmed by a psychiatrist. All patients with severe mental illness will be enrolled in the study.
Data Management and Statistical Methods
Findings for the study will be reported according to the CONSORT guidelines. The Statistical Package for the Social Sciences version 23.0 (SPSS) 23 will be used for the quantitative analysis. In accordance with good trial practices, data will be retained for seven years after completion of the trial.
Apart from baseline comparisons wherein descriptive sociodemographic details of the survey participants will be analyzed, prevalence figures will be tabulated along with frequencies of the various mental disorders and their comorbid physical health disorders.
Descriptive summaries of sociodemographic and clinical data will be provided for all trial participants at baseline, and for outcome measures at baseline, and 12-month follow up points; this will include means and standard deviations, or proportions, in the two arms, as appropriate. Scale and subscale totals with missing items will be pro-rated if 20% or fewer items are missing. Histograms within each arm will be used to assess normality of the distribution of the data, to identify any outliers and check for data errors. The proportion of participants who are fully, partially, or non-adherent to treatment (for both physical and mental disorders) will be reported for both arms.
The data will be analyzed under intention-to-treat assumptions (i.e., all those with baseline data will be analyzed in arms as randomized). The 12-month CGI score, adjusted for CGI scores at baseline (using analysis of covariance) and controlling for baseline value will be used for determining the comparative effects of the two arms. Similar methodology will be followed for other biological assessments made.
Results
The expected outcomes are that compared to the TAU group, the intervention group will show significant reduction in morbidity due to physical illnesses and improved mental health status.
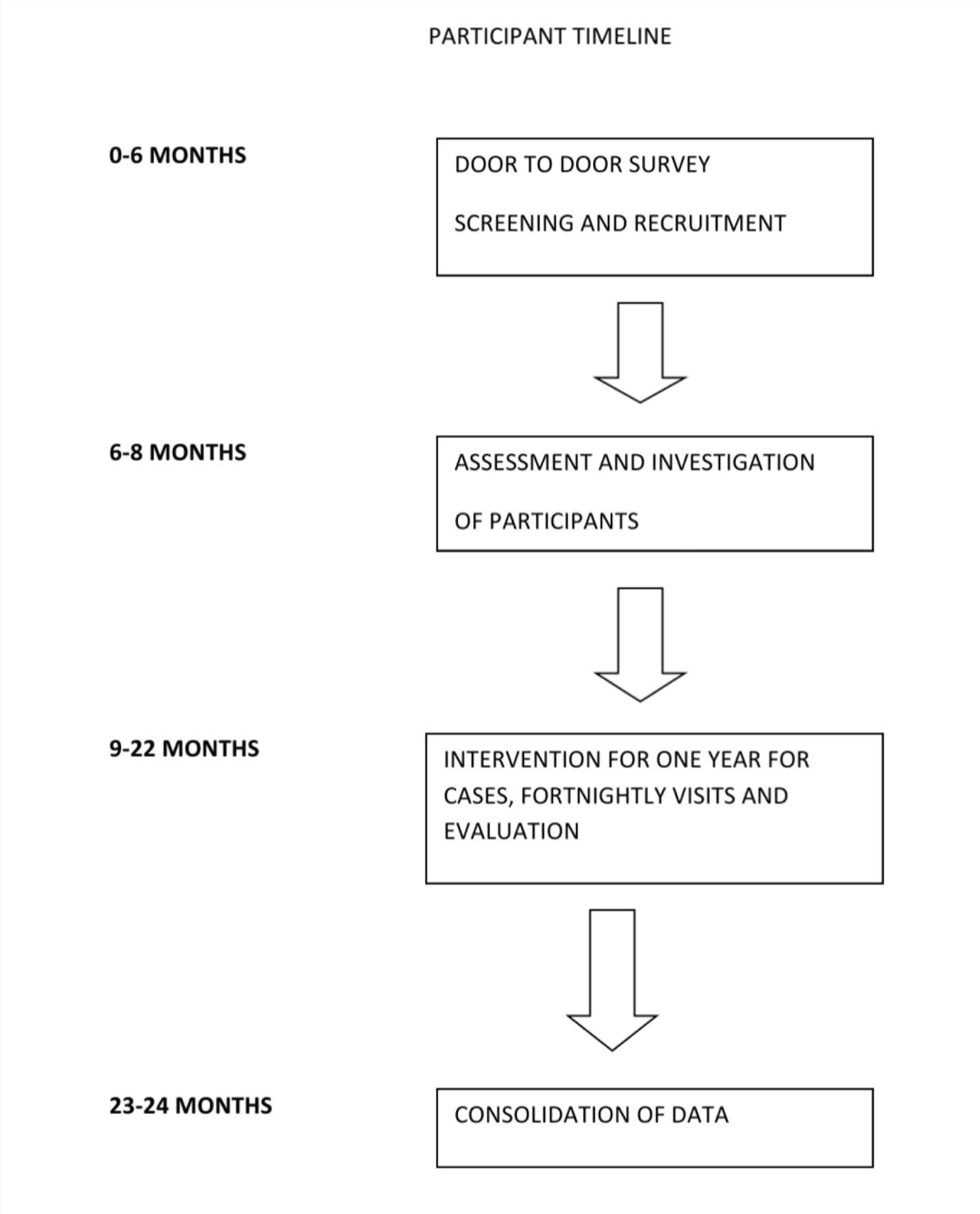
Timeline
The total period proposed for the project is three years, out of which the participants will be in the study for two years. The participant timeline is given in Figure 2.
Participant Timeline.
Implications
If the tested model is found to be more effective, it can be incorporated into the existing programs for delivery of mental health care by the CHW and can also address the important issue of comorbid physical health issues.
Limitations
One major limitation will be adequate sample size. With an estimated prevalence of severe mental disorders at 1%, 22 it is anticipated that about 380 individuals would have some form of a mental disorder. Assuming a prevalence rate of 50% with comorbid physical illness calculated with a confidence interval of 95% at 0.05 level of significance, a sample of 132 is required in each arm of the study, that is, total sample size of 264. All people who are found to have severe mental illness will be enrolled in the study. Assuming a 10% attrition, the number of people expected to complete the study will be around 342. Hence, the sample size should be adequate for the randomized control part of the study.
Strategies to Tackle Potential Confounders
One major factor is to ensure that all patients in the arm receiving the intervention module get uniform level of care under the intervention. Another issue is to ensure whether the participants were compliant with the interventions. The community workers are trained to use a manual prepared for intervention and record findings therein. To ensure that everyone in the intervention arm gets the same intervention, steps are manualized and action taken at every step is documented in the manual itself. Regular feedback is provided to the research team according to the manual. Cross verification is being done by the research staff to ensure standardization.
The CHWs who already have some experience in dealing with people with mental illnesses will be recruited and trained over a period of three months on the intervention module. The training will be imparted by mental health professionals from SCARF and TVMC. The CHWs will also have regular ongoing training throughout the period of the study to ensure the quality of the intervention is maintained. The fidelity of the intervention will be ensured by regular supervision of the staff by the trainers from SCARF and TVMC
One confounding factor would be the inability of patients with severe cognitive impairment to follow the interventions. Such patients will be excluded from the study.
Footnotes
Acknowledgements
This work is supported by the Indian Council Medical Research (ICMR) under Capacity Building Projects for National Mental Health Programme, ICMR-NMHP. We thank Dr Soumya Swaminathan (then Secretary, Department of Health Research, DHR), Dr Balram Bhargav (current Secretary DHR), Professor V.L. Nimgaonkar, Professor Smita N. Deshpande, Dr Ravinder Singh, and Dr Harpreet Singh. We thank the faculty of “Cross-Fertilized Research Training for New Investigators in India and Egypt” (D43 TW009114, HMSC File No. Indo-Foreign/35/M/2012-NCD-1, funded by Fogarty International Centre, NIH). We are also thankful to National Coordinating Unit of ICMR for NMHP Projects for their constant support and guidance. We thank Data Management Unit of ICMR for designing the database. The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of NIH or ICMR. NIH and ICMR had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This protocol paper describes the methodology of a research project funded under 'Capacity Building Task Force for Mental Health Research in India' funded by the Indian Council of Medical Research vide file number 5/4-4/151/M/2017/NCD-1. International mentors were funded by the training program ‘Cross Fertilized Research Training for New Investigators in India and Egypt’ funded by FIC, NIH (No. D43 TW009114).