
Abstract
Background:
The National Mental Health Survey identified a vast treatment gap across India. This treatment gap is partly attributed to the availability and accessibility of mental health services in different states. Accessibility to a psychiatrist in Madhya Pradesh (MP) is essential due to the significant disparity among urban, rural, and tribal regions across the state. The study attempted to identify the geographical disparity of psychiatrists in MP to improve future mental health service delivery.
Methods:
An online survey of practicing psychiatrists was conducted in December 2022 in the settings of public and private healthcare service delivery systems through offline and online accessibility/availability of psychiatrists practicing in MP, and the data were mapped using geo-locations of psychiatrists and were analyzed using ArcMap 10.8.1.
Results:
In total, 152 psychiatrists were practicing in MP across 195 locations, which amounts to 0.21 psychiatrists per 100,000 population with a concentration around big cities. Out of 54 districts, 24 districts did not have any practicing psychiatrists. A total of 155 health facilities were identified across 30 (55.6%) districts where at least one psychiatrist provided mental health services. The nearest-neighbor index for 152 points was –13.69.
Conclusions:
Combining psychiatrist geo-mapping data with population data comprehensively explains the MP state’s mental health service delivery needs. It could be wise to improve the spatial distribution of psychiatrists in each district rather than achieving the recommended ratio of doctors to patients per state. These data need to be supplemented with qualitative inquiry to help policymakers and health planners generate effective public–private partnerships in mental health service delivery in the coming time.
Keywords
A considerable treatment gap for mental disorders across Madhya Pradesh is attributed to the geographical disparity in availability and accessibility to a psychiatrist. There is a need to improve the spatial distribution of psychiatrists in each district rather than achieve the recommended ratio of doctors to patients. Future mental health service delivery may combine psychiatrist geo-mapping data with population data to understand mental health service delivery needs comprehensively.Key Messages:
Mental disorders are a significant public health concern in India, ranking at the top in terms of Years Lived with Disability according to the latest Global Burden of Disease Study 2017 estimates. 1 The burden of mental disorders is exceptionally high among adults between the ages of 15 and 49 years, which is also the most productive age group. Madhya Pradesh (MP) is the second largest state in central India, having a population of 7.2 million, and it is divided into 54 districts. 2 Despite the lifetime prevalence of mental disorders among the adult population in India being 16.7%, only a few psychiatrists are available to provide specific mental health interventions, which results in a huge treatment gap. Unfortunately, MP has a treatment gap as high as 91%. Also, according to the National Mental Health Survey (NMHS) 2015–16, the state has only 0.2 mental health professionals per lakh population and 0.05 psychiatrists lakh population, far less than the recommended national requirement of one psychiatrist per lakh population. 3
In a survey, the median interval between the onset of illness and consultation was 1 year. 3 It is also reported that at least two healthcare providers were consulted by the patient for mental disorders, and two-thirds of the times consulted doctors were from the public sector. 4 The majority of the patients who reported seeking mental health care were found to be relying on magico-religious therapy from temples, dargahs, local priests, or traditional healers. The main reasons reported for not seeking advice from the psychiatrists were costly treatment, distant hospitals, lack of availability of psychiatrists, and unawareness about the treatment. 5
This prompts us to study the geographical inequality of psychiatrists in MP. Identifying areas with high treatment gaps due to unequal geographical distribution would be an essential contribution to prioritize the distribution of mental health services in the state. 6 Since Psychiatrists are pivotal in the delivery of both pharmacotherapy and psychotherapy, the availability of psychiatrists would almost meet the expected professional barriers for mental health delivery. This study aimed to find the total number of working psychiatrists and their spatial distribution in MP, including the government and private sectors.
Methods
Study Design and Settings
This cross-sectional study was conducted in public and private healthcare service delivery systems within MP. The Institutional Human Ethics Committee reviewed and approved the protocol (LOP No 2021/ IM0263, dated April 17, 2021).
Participants
The study included all psychiatrists practicing in MP as of December 2022, except for postgraduate trainees of psychiatry and psychiatrists who had migrated elsewhere and were currently not practicing in MP.
Study Variables
The questionnaire extracted information on the address of the health facility with pin code and geo-location of the health facility providing mental health services.
Data Collection Tool
A self-reported questionnaire was developed, which included information on the location of the psychiatrist practicing in MP and the facility through which the mental health services are delivered. These services were categorized as Medical college (M), District hospital (D), Other Govt hospital (G), Private clinic (P), Addiction treatment centers (A), Proposed but not started addiction treatment centers (A*), and Mental health institution (MHI). The facility associated with the medical college is operationalized under the M category. An institution operated by the government deploying only specialized psychiatric services, research, and education, which is responsible for consultation with patients, community programs for education and quality of care, was operationalized as MHI. This questionnaire was deployed on a paperless data collection platform through which a link for an online web form was generated (KoboToolBox, free, open-source software [GNU License]).
Data Collection Procedure
All the psychiatrists working in MP were approached using three methods. First, 152 psychiatrists (excluding residents) who were members of the WhatsApp group of psychiatrists in MP were approached. We circulated the link to the web form. We adopted the snowball sampling method wherein psychiatrists were asked to forward links to their known psychiatrists. Because there is a limited number of psychiatrists, snowball sampling was employed to reach the maximum sample within a short period. Then, the data were supplemented based on the publicly available information obtained from the websites of the Indian Psychiatry Society (IPS), Indian Psychiatry Society-Madhya Pradesh Chapter (IPS-MP), and the National Medical Commission website. The information was limited to the psychiatrist in MP as of December 2022. Responses collected from those psychiatrists who practice at multiple locations, such as both a medical college and a private clinic were represented twice for their location of service delivery. These psychiatrists were represented at each location where they provide services. For instance, a psychiatrist working at a medical college and associated with two private clinics would be represented at three different service delivery locations. Postgraduate trainees of psychiatry and psychiatrists who migrated elsewhere and are currently not practicing in MP were excluded from the data. Finally, a registered list of psychiatrists practicing in MP was obtained from the IPS-MP to supplement the missing data. The geographical coordinates of the locations where psychiatrists were providing services were primarily obtained through a paperless data collection form that included a feature to fetch geo-location information. The survey included non-mandatory questions, including information about specialty services such as geriatric, addiction, child and adolescent, etc., and types of services such as inpatient, outpatient, electro-convulsive therapy (ECT), and psychological intervention services. Participation in the survey constituted an indication of consent.
Psychiatrists filled out this form to provide their location data. In case data were supplemented through the methods described above, we have obtained geographical coordinates from the addresses provided in these databases.
Data Analysis
We downloaded the data as a spreadsheet from a paperless data collection platform. Data obtained from supplementary sources were added to this spreadsheet. The frequencies of the types of health facilities and the number of health facilities per district were calculated. The density of psychiatrists per 100,000 population was computed by considering district-wise population as per the Government of India Census 2011 2 in the denominator and the total number of psychiatrists practicing in that district in the numerator. Then, we mapped the geo-locations of psychiatrists using ArcMap 10.8.1. The spatial distribution of psychiatry facilities/services was plotted using geo-coordinates. We computed a nearest-neighbor index (NNI) to explore whether there is clustering. The NNI is a statistic that quantifies a dataset’s spatial distribution of points. It compares the observed average distance between each point and its nearest neighbor to the expected average distance under a completely random distribution. If NNI < 1 indicates clustering, meaning points are closer to each other than they would be in a random distribution. If NNI = 1, it suggests a random distribution. If NNI > 1, it suggests dispersion, meaning points are farther apart than in a random distribution. In our context, it is based on the average distance of each psychiatrist location to its nearest-neighboring psychiatrist location. We have also generated a choropleth map of districts of MP by density of psychiatrists per 100,000 population.
Results
We have approached 152 psychiatrist members of a WhatsApp group of psychiatrists practicing in MP. Of these, 65 members from the WhatsApp group completed the mandatory part of the questionnaire. Additionally, 20 responses were obtained from non-members of the WhatsApp group who might have received the forwarded link as envisaged for snowball sampling. Then, we identified 24 psychiatrists from the District Mental Health Program (DMHP) and 43 from the IPS-MP chapter. Thus, we have been able to identify 152 Psychiatrists and map a total of 195 places of their services in the state of MP as of December 2022. Overall, responses obtained through snowballing were 85 out of 152 (response rate of 56%). The total number of psychiatrists practicing in the government sector was 55. The density of psychiatrists is represented in Figure 1.
Spatial Distribution of Psychiatrists Practicing Locations Across the State.
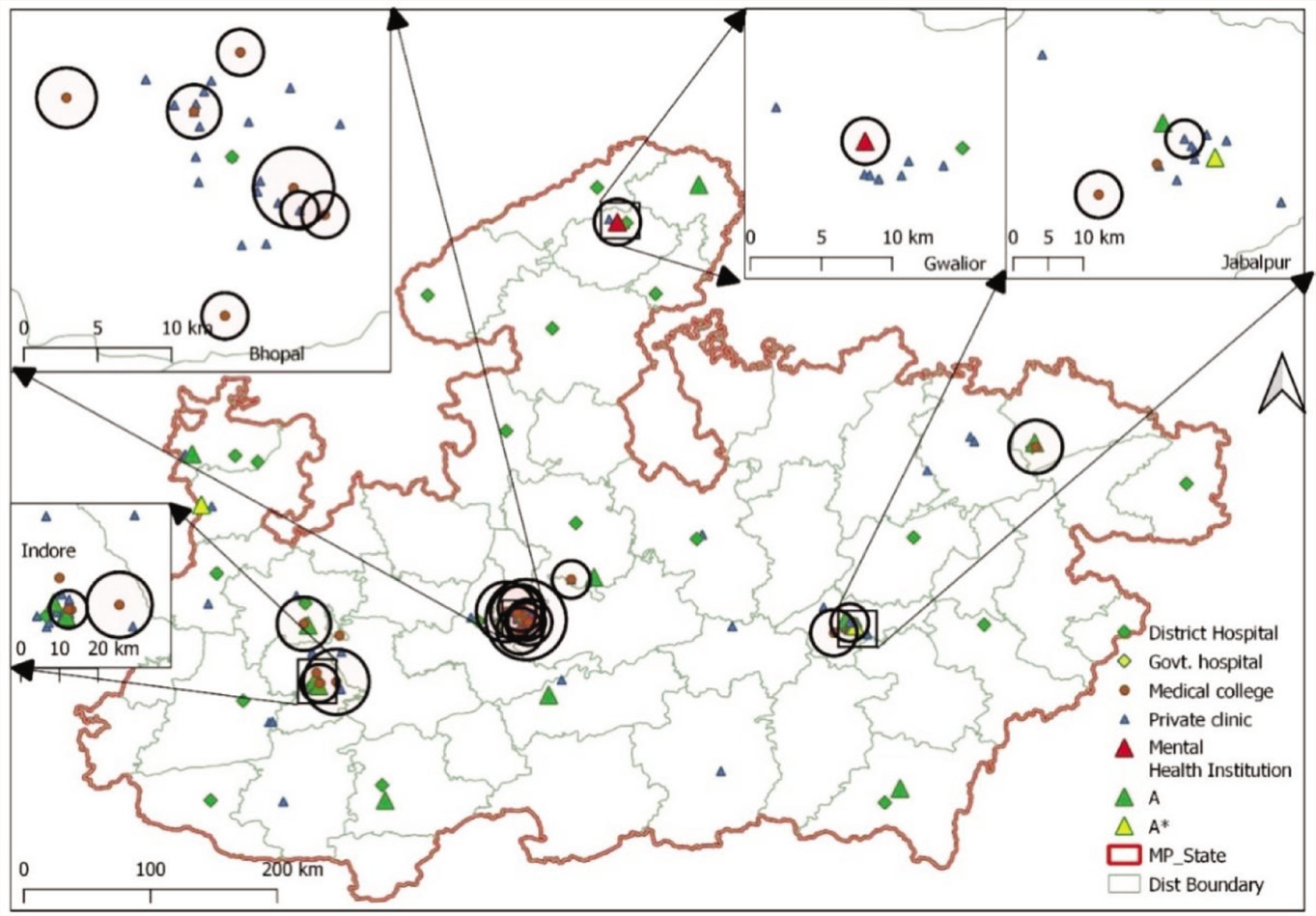
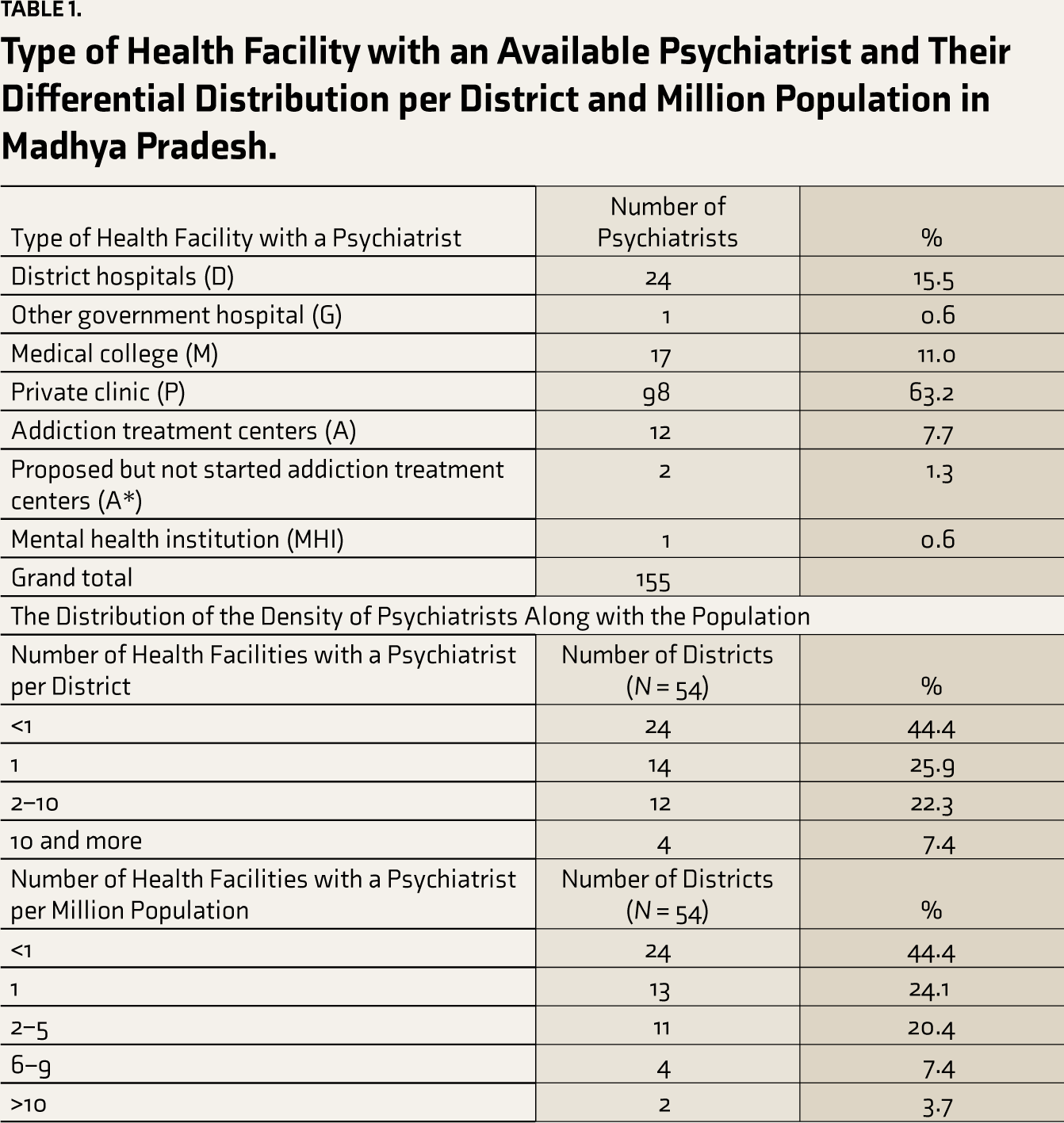
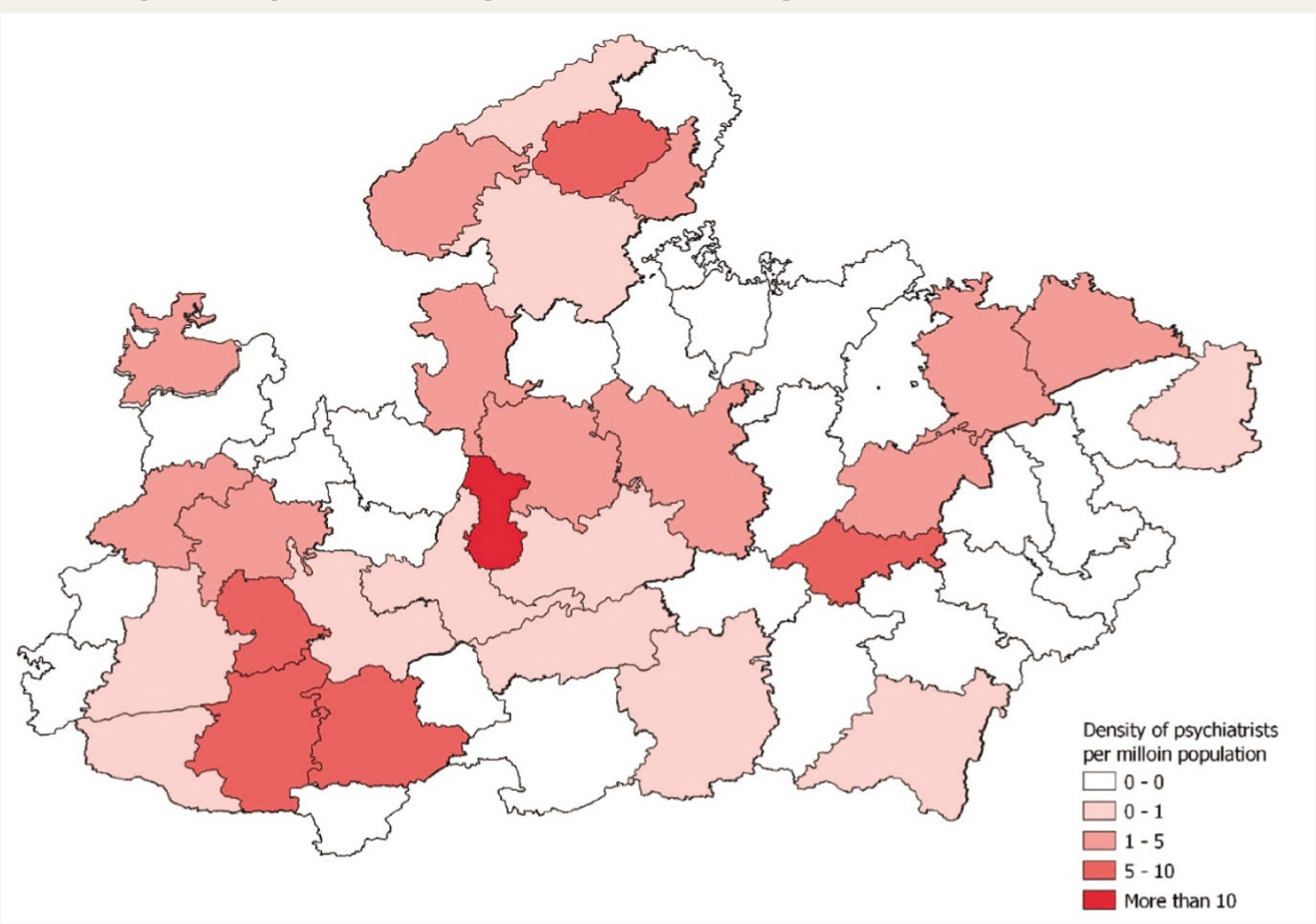
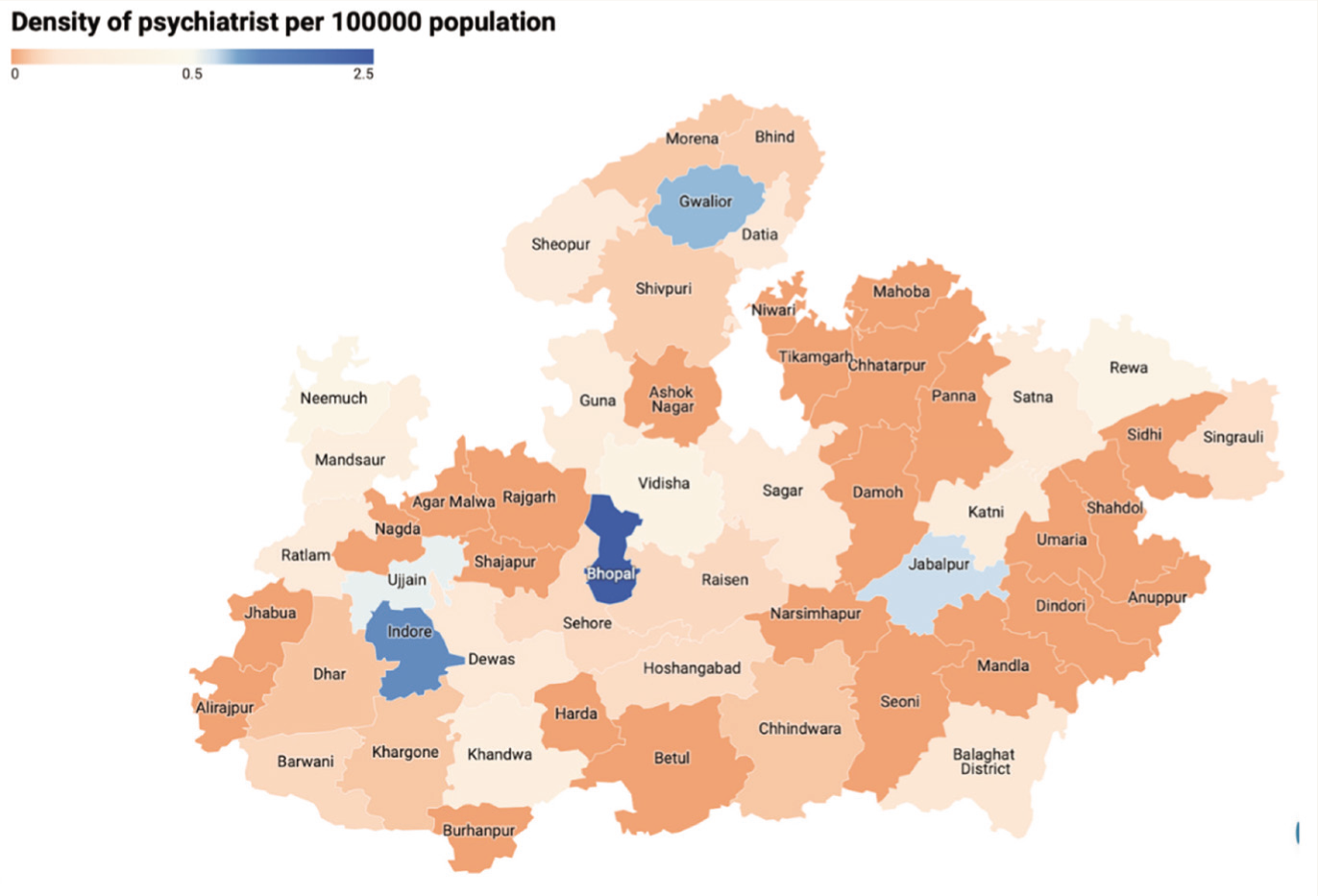
This amounts to 0.21 psychiatrists per 100,000 population for the state of MP. Out of 54 districts, 24 districts did not have any practicing psychiatrists. A total of 155 health facilities were identified across 30 (55.5%) districts where at least one psychiatrist provided mental health services. The distribution of these facilities by their type is shown in Table 1. Figure 1 reflects the spatial distribution of psychiatrists across the state. It can be observed that most of the psychiatrists are clustered in the bigger cities of the state, viz Indore, Bhopal, Gwalior, Jabalpur, and Ujjain. Nearest-neighbor analysis for 152 points revealed an observed mean distance of 0.10, expected mean distance of 0.24, NNI of 0.42, and Z-score of –13.69. Given the Z-score of –13.69, there is a <1% likelihood that this cluster could result from random change. Figure 2 shows the density of psychiatrist services per 100,000 population. Figure 3 shows the choropleth map of the density of psychiatrists per 100,000 population. The supplementary table and figure show the nearest-neighbor analysis.
Type of Health Facility with an Available Psychiatrist and Their Differential Distribution per District and Million Population in Madhya Pradesh.
Density of Psychiatrists per 100,000 Population.
Choropleth Map of the Density of Psychiatrists per 100,000 Population.
Discussion
Geo-mapping psychiatrists currently practicing in MP provide relevant information to researchers and stakeholders regarding the total number of practicing psychiatrists and the location of their health services in the MP state. The recommended number of psychiatrists, according to the World Health Organization, is 3 per 100,000 population, whereas the national average falls around 0.75 per 100,000 population. As per national data, the availability of psychiatrists varies from 0.05 per lakh population in MP to 1.2 per 100,000 population in Kerala; however, as noted earlier, we do not have the data on state-wide distribution in terms of geographical accessibility, which is worth reporting. 7 In this background, the Bhopal district, with 1.98 psychiatrists per 100,000 population, is observed to be doing better compared to other districts of MP (0 to 0.89 per 100,000 population) and collective MP (0.21 per 100,000 population). This complements the findings from the major states of India because major training institutes and private clinics providing mental health services are located in major cities in India, such as Delhi, Bangalore, Chandigarh, etc. Our study findings also report an increasing number of services being located around the major cities of Bhopal and Indore. Most of the services are provided by private clinics, followed by the contribution of district hospitals, the DMHP, and the medical colleges in MP. 7 It is good to see the expansion of psychiatric services to bridge the service delivery gap as opposed to the institutionalization of patients with mental disorders. Though most medical colleges have filled their post of psychiatrists, nearly 17 psychiatrists’ posts were vacant in DMHP at the time of the survey. Responses obtained from those psychiatrists practicing at more than one location were represented, respectively. However, this kind of data only appeared to be clustered around the major districts of MP. Notably, 24 (44.4%) districts have no psychiatrists, and 14 (25.9) districts have only one psychiatrist, reflecting the disproportionate availability of mental health services. 8
One of the reasons could be the higher demand for mental health services and the higher prevalence of mental disorders in urban populations because of urbanization-associated stress, social isolation, and lifestyle changes, which can precipitate mental health problems. 9–15 Another reason could be higher professional and income opportunities, better infrastructure, and better quality of life in urban areas, which provide natural migration of psychiatrists to urban areas over rural and tribal regions in MP and even in other states of India. The flip side is that it is also true that lack of awareness and higher stigma in rural areas might discourage people from approaching psychiatrists and indirectly contribute to lesser demand for the migration of psychiatrists to rural regions. Urban areas of MP also have greater availability of resources, such as funding and technology, to provide more comprehensive and advanced mental health services such as Electroconvulsive therapy, repetitive transcranial magnetic stimulation, etc., compared to rural areas. Government policies and initiatives might also indirectly be more focused on improving mental health services in urban areas due to the higher demand and availability of resources. Our study is the first attempt to understand the geographical disparity in accessing psychiatric services in MP and corroborate the estimated treatment gap of 70%–92% reported by the NMHS survey.3,10,11,16 Many of the metro cities in India have a surplus of doctors and specialists, which is better than the doctor–patient ratio of 1:1000. However, we fail to acknowledge that the geographical distribution of services is a better index than the ratio of doctors to population, which perhaps holds only for urban areas where population density is high. Therefore, equal distribution of services takes precedence over the generation of additional specialists and human resources, as indicated by these findings. 11
The possible solutions that are in place include increasing the number of postgraduate seats in psychiatry, reserving seats for candidates from the service-deprived region of India, and surveys to draw attention to differential resources available in the country. However, this study attempts to add value by assessing ground-level disparity of the total number of psychiatrists in the state of MP. Since earlier attempts such as merely training medical officers and nurses alone for this purpose 17 have not helped to equalize the district-wise treatment gap, 18 we propose better solutions such as retaining doctors in rural and tribal areas by providing a safe atmosphere, regular rotations, empowering and formally training the medical officers and nurses residing in such regions, creating psychiatrist posts in all districts and reserving MD seats for medical officers serving in underprivileged areas with a clause for bond to address the mental health needs of the specific population may be considered. Service delivery projects for such regions should prioritize establishing culturally acceptable models of indigenous healing methods and amalgamating traditional, conventional, and advanced medicinal models. The government initiative to launch the bridge courses should be carefully weighted from the service delivery lens regarding increasing accessibility of mental health professionals. 19 Identifying the low-performing districts, wherever feasible, holding traditional medical camps remains one of the solutions. The recent initiative in the Sehore district by training the medical officers and task sharing with community health workers has delivered good results20–22. Such models can see the replication elsewhere. Learning from the NMHS, taking one step forward with these findings, we must focus on targeted interventions and services that could address the problem of addiction, child and adolescent, and geriatric needs. In a nutshell, the findings emphasize that it is essential to understand the inequality in the accessibility of psychiatrists and not figures of best or worst-performing state in the Indian context.
Therefore, to prevent people in rural areas from traveling long distances to access mental health services, to increase awareness, and to reduce stigma, effective and incentivized government policies and initiatives focusing on improving mental health services in underserved areas, initiating Tele Mental Health Assistance and Networking Across States (Tele-MANAS) or telepsychiatry services is recommended to reach underserved populations.9,22,23 Post-coronavirus disease (COVID), the development of Tele-MANAS services and their utilization has been a significant leap forward and appears to be a great alternative to increase accessibility. 23 However, Tele-MANAS or any telepsychiatry intervention cannot offer free medications for which many poor patients can depend on the government-run facilities in the MP, such as medical colleges or district hospitals where free medications are offered.9,24–27 Lastly, psychiatrists in private practice cannot offer free consultations and free medications for most of their clientele, including consultation to poor people who might not be able to afford private health services, which should also be recognized.28–30 Overall, combining geo-mapping data with population data can provide a more comprehensive understanding of the country’s mental health service delivery needs and help policymakers plan and implement effective interventions.
Limitations
Given the sampling strategy and lack of a registry of specialists in the state, the study may reflect a different number of psychiatrists currently practicing in MP. Mental health services provided by Tele-MANAS services and other mental health professionals, including psychologists, social workers, trained medical officers /practitioners of alternative medicine, and non-psychiatrists, are not considered in this study. The census used was 2011 because the recent update in the census numbers is awaited. Another limitation would include the overlapping accessibility to services across the border districts that cannot be captured through nearest-neighbor analysis; such an approach is a methodological limitation. However, with mental health being an integral part of health service delivery in a state, we recommend establishing the minimum possible number of psychiatric services in each district. This survey did not provide the qualitative inquiry to reveal the psychiatrists’ perspective on the urban concentration of mental health services. Psychiatrists working in the private sector may also be involved in outreach services through a clinic or camp-based approach, which is not covered in this study.
Conclusion
The district-wise inequality in the accessibility to psychiatrists is perhaps a better indicator than the doctor–patient ratio for mental health care in many states of India. Concerning the high level of inequality, the state of MP needs more service projects, programs, camps, telehealth facilities, and government initiatives through public–private partnerships in many underperforming districts. To achieve the goal of optimum mental health, stakeholders need to review and prioritize the accessibility to different mental health professionals in these regions. Future efforts should map the accessibility of mental health services offered by other professional services, encouraging professional bodies such as the IPS to update the registry of practicing psychiatrists in the different states, make them publicly available, and empower public–private partnerships with task sharing to make easy accessibility of such services in the state.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.