
Abstract
Background:
Mental health literacy among lay community health workers (CHWs) is crucial to ensuring that mental health services are accessible to all. This research explores the mental health literacy of community health workers in Indonesia.
Methods:
A cross-sectional study was carried out among 454 female community health workers from various villages. Their understanding of mental illness was assessed through questionnaires, exploring their overall belief about the cause and consequence of mental illness, the symptom and the treatment of mental illness, and their perception of relapse.
Results:
Most participants have false beliefs about the causes and consequences of mental illness. For instance, the majority of respondents agreed that severe stress leads to mental illness (80%), while 60.4% believed personal weakness to be a cause. Cognitive impairments and brain disease were associated with mental illness by 67.2% and 57.3%, respectively, although only 32.6% attributed it to hereditary factors. Regarding treatment, 83.9% of respondents believed that consistent medication could fully cure mental disorders, while 81.1% associated mental illness with strange behavior. Additionally, 90.7% of respondents emphasized the importance of regular medication to prevent relapse, with 81.5% stating that lack of medication leads to relapse.
Conclusion:
A significant level of misinformation and misconception among participants regarding mental illness was unveiled. This misunderstanding can contribute to the stigmatization of individuals experiencing stress, as it may lead to unwarranted assumptions about their mental health. These findings underscore the importance of targeted mental health education campaigns to address misconceptions.
CHWs facilitate connections between community health services and service users, providing essential and practical support to those seeking healthcare. CHWs have limited knowledge about mental illness and have the potential to cause stigma toward people with mental illness CHWs need mental health literacy to increase community understanding in supporting the patient and to decrease the stigma.Key Messages:
In Indonesia, around 9.8 million people experience mental disorders; however, because of stigma and limited access to mental health services, most of the population is unaware of these issues. 1 Community health workers (CHWs), often the first point of contact for health services in rural areas, play a crucial role in bridging this gap.2,3 However, many CHWs lack proper mental health training, resulting in misconceptions that can hinder their ability to support individuals in need effectively. Mental health literacy—knowledge and beliefs about mental health—significantly shapes community perceptions and responses to mental disorders.4,5 It includes understanding symptoms, treatment options, and the importance of seeking timely care, which is essential for accessible mental health services.
Improving mental health literacy among CHWs is key to promoting equitable access to mental healthcare across diverse populations. As facilitators between health service and community members, CHWs provide essential support, but stigmatizing attitudes among some CHWs can obstruct this role. A recent review highlighted their limited mental health knowledge and stigma toward people with mental illness. 6 Nevertheless, there is little understanding of whether CHWs themselves encounter psychological challenges related to interaction with patients and families.
In Indonesia, CHWs, also known as “health cadre,” are often the closest source of health information for their communities. Although they receive formal training, such as 22 hours for Posyandu cadres, the curriculum primarily emphasizes specific health programs, leaving other health topics, like mental health, underexplored.7–9 Community expectations for CHWs to assist patients with mental illness, coupled with their limited mental health literacy, highlight a critical gap. Research shows that both CHWs and health professionals in Indonesia have low mental health literacy, yet few studies address this issue.10,11 This study seeks to fill this gap by examining the mental health literacy of female CHWs in Indonesia, focusing on their understanding of mental illness, treatment options, and relapse prevention. Findings will inform training and policy to empower CHWs as vital resources in mental health support.
Methods
This cross-sectional study was conducted among female CHWs in villages across Aceh, East Java, and Jogjakarta provinces in Indonesia. A cross-sectional design was chosen to capture a snapshot of mental health literacy among CHWs in varied geographic areas. Using convenience sampling, both urban and rural respondents were recruited through local CHW networks and community health centers. Participants were eligible if they were aged 18 years or older and actively engaged in community health-related activities.
Setting and Sample Size Justification
The study included 454 participants, selected based on logistical feasibility and anticipated participation rates to enable descriptive and associative analyses. Recruitment took place in Puskesmas (community health centers) and similar accessible locations across urban and rural areas in the study provinces, ensuring the representation of diverse socio-demographic profiles.
Data Collection
Data were collected from June to July 2023, with structured questionnaires administered face-to-face at Puskesmas or nearby community locations to facilitate understanding and access. The questionnaire included sections on socio-demographic characteristics (age, ethnicity, education level, and CHW service duration) and mental health literacy.
Instruments
Mental health literacy was assessed using a questionnaire that measured the participants’ understanding of mental illness, including belief about its cause, consequence, symptoms, treatment options, and perception of relapse. This questionnaire has been previously used among healthcare professionals.11,12 Rather than focusing on a specific mental disorder, it examines public understanding of mental illness in general. Developed based on qualitative investigation into public mental health understanding, 13 it has been validated among health professionals, achieving an overall reliability coefficient of 0.89, indicating a high level of internal consistency. 11 The original questionnaire consists of 23 items, 12 with three response options—“agree,” “neutral,” and “disagree”—where the final judgment is based on the agreement indicated by respondents. In this study, we adapted the questionnaire for a lay population, removing several questions related to antipsychotic medications due to the assumption that non-professionals would have less familiarity with these topics. The adapted version demonstrated a moderate level of internal consistency (Cronbach’s alpha) of 0.75, indicating reasonable reliability in measuring the underlying construct.
Bias Consideration and Handling of Missing Data
As convenience sampling was used, there is a potential for selection bias, which may limit the generalizability of findings beyond the sampled CHWs. Additionally, the questionnaire’s self-reported nature could introduce response bias, particularly in sensitive questions related to mental illness perceptions. For missing data, incomplete cases were excluded from specific analyses without imputation.
Statistical Analysis
Descriptive statistics were employed to summarize the demographic characteristics and mental health literacy. For each of the 12 literacy statements, binary logistic regression analyses were conducted to explore the association between socio-demographic information and participant responses. To facilitate analysis, responses were coded as follows: “Agree” was assigned a value of 1, while “Neutral” and “Disagree” were combined and assigned a value of 0. No adjustments for confounding variables were made as the analysis was exploratory in nature. Statistical significance was set at P < .05 and analyses were performed using Stata 13. 14
Ethics Approval and Consent
The institutional Ethics Committee approved the study before data collection (Reference Number: 2921). All participants provided informed consent, with assurances of confidentiality, voluntary participation, and the right to withdraw at any time. The participant consent (assent from those 18 years of age) already had the consent from parents.
Results
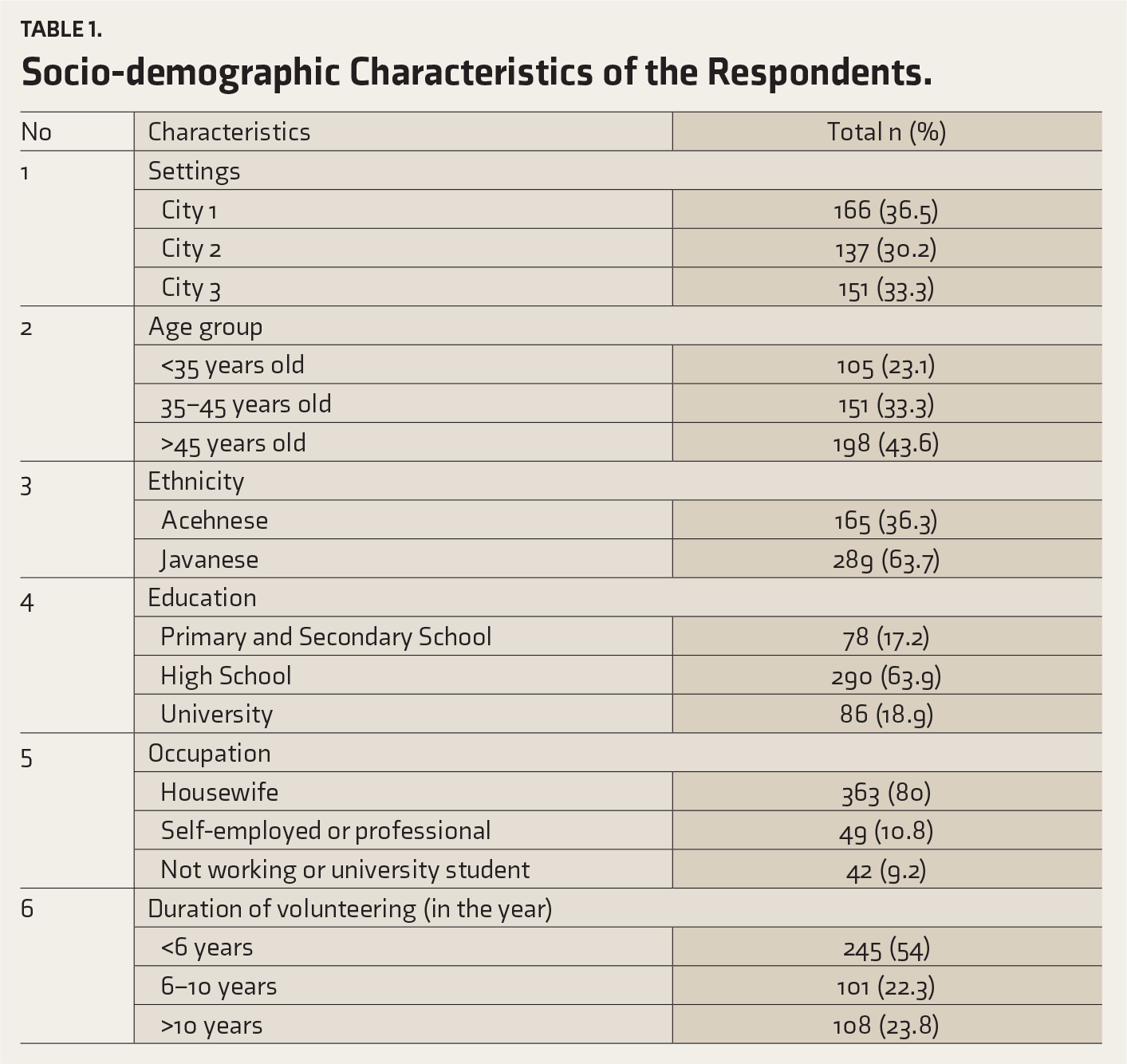
Out of 454 female CHWs who participated in this study, more than half were Javanese ethnics (63.7%), had a senior high school level of education (63.9%), and had been volunteering as a CHW for less than six years (54%). Almost half were over 45 years old (43.6%), and the vast majority were housewives (80%). A detail of the socio-demographic profile is presented in (Table 1). Regarding the misconceptions about mental illness, a significant majority believe that anyone experiencing intense stress will inevitably face mental health challenges (80.2%). Additionally, over half mistakenly perceive mental illness as a sign of personal weakness (60.4%) and think it can lead to cognitive impairments (67.2%). Conversely, some view mental illness as a brain disease (57.3%) and believe it can be inherited (32.6%).
When it comes to treatment and relapse, many incorrectly think that consistent medication adherence alone can result in complete recovery for individuals with mental disorders (83.9%). A substantial number also believe that people with mental illness often display unusual behaviors and engage in disorganized speech (81.1%). However, there is a strong consensus that regular medication is essential for preventing relapse (90.7%). Details regarding the respondents’ understanding of mental illness are presented in (Table 2).
Socio-demographic Characteristics of the Respondents.
Respondents’ Literacy in Mental Illness and Treatment.
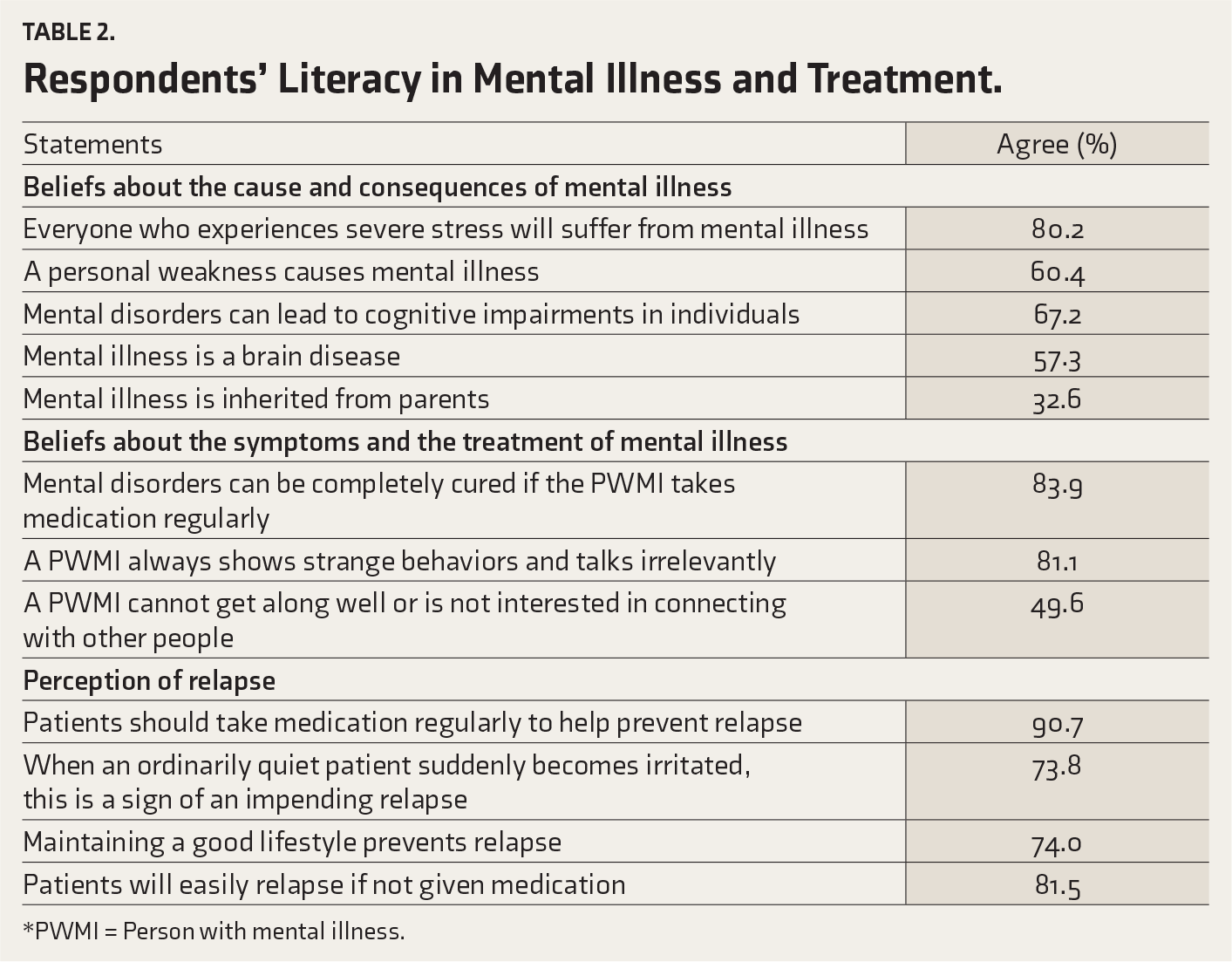
*PWMI = Person with mental illness.
Further statistical analysis confirms that the Javanese were more likely to believe that individuals who experience severe stress will suffer mental illness (OR = 1.8, P = .012) compared to the Acehnese. The Javanese were also more likely to believe that mental illness is caused by a personal weakness (OR = 2.1, P = .001) and that mental disorders can be completely cured if they take medication consistently (OR = 1.9, P = .012).
The age group was also found to be associated with several statements. Compared to those aged < 35 years old, the respondents aged > 45 years old were more likely to believe that individuals with severe stress will also suffer mental illness (OR = 3.6, P = .001), that mental illness is caused by a personal weakness (OR = 2.4, P = .001), that mental disorders can be completely cured if the patients take medication consistently (OR = 2.3, P = .007), and that patients should take medication regularly in order to prevent relapse (OR = 3.9, P = .001).
The duration of volunteering also plays a significant role in individual mental health literacy. Compared to those who had been volunteering for less than six years, those who had been volunteering for more than 10 years were more likely to perceive that mental illness is caused by a personal weakness (OR = 1.8, P = .012), that it is inherited from the parents (OR = 1.7, P = .024), that it can be completely cured if the patient takes medication consistently (OR = 3.1, P = .004), that patients should take medication regularly in order to prevent relapse (OR = 14.9, P = .008), and that patients will easily relapse if not given medication (OR = 3.3, P = .002). Lastly, we found a poor association between education and occupation with any statements of literacy toward mental illness (P > .05).
Discussion
The findings of this study highlight a unique interplay between ethnicity, age group, and volunteering duration with mental health literacy among female CHWs. We found that despite working closely with persons with mental illness (PWMI), the CHWs’ understanding and beliefs about mental health remain limited, especially in relation to misconceptions such as viewing mental illness because of personal weakness. Conversely, a majority correctly acknowledged that “Patients should take medication regularly to help prevent relapse.” These findings indicate that despite their relatively close engagement with PWMI, their literacy and beliefs about mental health remain problematic.
The duration of volunteer work is expected to enhance understanding of mental health issues; however, our results show that this does not translate to improved mental health literacy in this population. Previous studies have indicated that longer duration in volunteer roles improves motivation, 15 knowledge, and literacy. 16 However, the experience of this population reveals that even those who have volunteered for over ten years may possess worse mental health literacy than newer volunteers. This poor association between work experience and mental health literacy suggests that other variables, such as education, may play a significant role. 17 The lack of training and knowledge-sharing sessions between health professionals and the CHWs could be the reason for their lower mental health literacy. Providing basic mental health training, such as first aid training, should be initiated to help them understand mental health better.
Additionally, our study reveals the significant role of age in mental health literacy. Respondents aged above 45 years exhibited distinct beliefs, highlighting a heightened tendency to associate severe stress with mental illness, viewing mental health issues as stemming from personal weakness. Those beliefs could be based on their experience rather than formal information from health professionals. Functional health literacy was markedly lower among older age groups, even after adjusting for differences in cognitive function, newspaper reading frequency, health status, and visual acuity. 18 The older age group usually exhibited a robust correlation with reduced levels of mental health literacy.19,20 They also tend to have a higher stigma about mental illness, and it is strongly associated with lower mental health literacy. 21 These insights underscore the importance of tailoring mental health education and awareness campaigns to these age groups, acknowledging and addressing varying perspectives within the community for more effective communication and support systems.
Lastly, our study’s revelation of poor association between education, occupation, and mental health literacy contrasts with some previous reports. The extent of education provided by schools was a strong predictor of understanding and awareness of mental health issues. 22 Higher education was also linked to elevated health literacy scores.23–25 In our study population, however, mental health education has not been provided in formal schools. Therefore, despite higher education levels, their mental health literacy could not be much better than those with lower education levels. These findings challenge conventional assumptions, suggesting that the nuanced understanding gained through extended volunteering may surpass the influence of formal education or professional background in shaping beliefs about mental health. These findings emphasize the need for targeted interventions and educational initiatives within volunteer programs to enhance mental health literacy and mitigate potential misconceptions that may develop over a prolonged volunteer service.
Limitations of the Study
Despite the interesting findings, this study is limited by its non-random sampling methods, which prevent the calculation of the response rate and its cross-sectional design, which inhibits the establishment of causality. Additionally, self-reported data may introduce information bias, and we did not perform the Bonferroni correction in our analyses, which is another limitation of the study.
Conclusions
Our findings contribute to our understanding of the mental health literacy of female CHWs in Indonesia and underscore the imperative for targeted mental health education campaigns. The identified misinformation and misconceptions emphasize the need for interventions that dispel myths, reduce stigma, and enhance mental health literacy within this crucial cadre of health promoters. As this article unfolds, it calls for a concerted effort to integrate mental health education seamlessly into community engagement strategies, fostering a more informed and compassionate approach to mental health within communities.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors want to express gratitude to the participants who have agreed to participate in the study, the CHWs and Nurses in the region area of Community Health Center in Banda Aceh (Kota Baru and Kuto Malaka), in Surabaya (Pacar Keling, Medokan Ayu, and Kalijudan), and Yogyakarta (Bantul and Sleman). We also thank Universitas Syiah Kuala, Banda Aceh, Universitas Airlangga Surabaya and Universitas Gadjah Mada Yogyakarta for all facility during the research project
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None Used.
Ethics Approval
Ethical approval was obtained from the Universitas Airlangga Ethical Review Board before data collection (Reference Number: 2921-KEPK). All participants provided informed consent, with assurances of confidentiality, voluntary participation, and the right to withdraw at any time.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Program Riset Kolaborasi Indonesia (RKI) of Syiah Kuala Universiti, Banda Aceh, Indonesia and Program Riset Kolaborasi Indonesia (RKI) – World Class University (WCU) Lembaga Penelitian dan Pengabdian Masyarakat Universitas Airlangga in 2023 with the number: 974/UN3.LPPM/PT.01.03/2023.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.