
Abstract
Background:
People with alcohol use disorders (AUDs) have varied needs while they seek treatment. Understanding and focusing on the needs will improve treatment outcomes. The objective of the study is to qualitatively assess the treatment-related needs of patients with AUDs admitted to a tertiary care treatment center.
Methods:
A semi-structured questionnaire with anchor questions was developed based on a literature review and key informant interviews. All the interviews were audio recorded, transcribed, and color-coded manually. Two reviewers reviewed the codes. Themes and subthemes were generated using thematic inductive analysis.
Results:
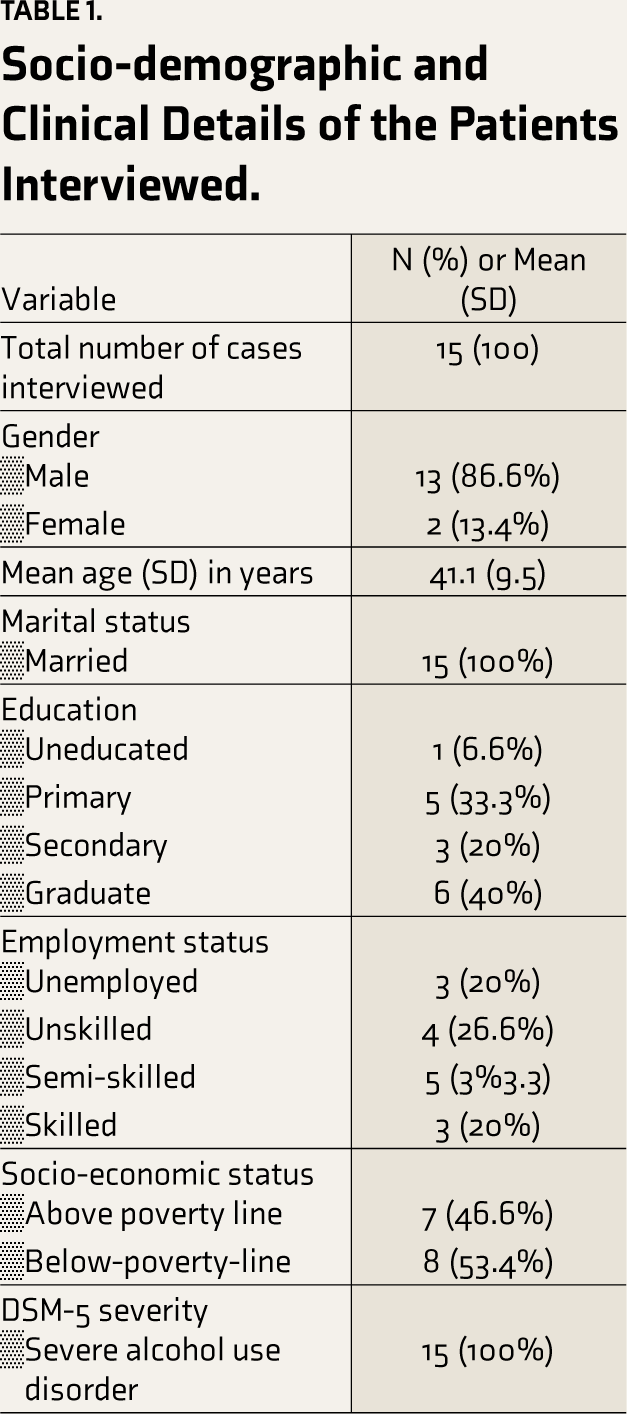
Among 15 patients interviewed, all the patients had severe AUD (100%), were married (100%), were primarily males (86.6%), and more than half below the poverty line (53.4%), with a mean age of 41.1 years (SD = 9.5). Four major themes of treatment needs were identified: (a) individual, (b) family-related, (c) hospital-related, and (d) community-related. Among individual needs-medication-related, psychological, and occupational were prominent. Addressing family conflict and supporting the family are the significant subthemes for family-related needs. The behavior of the treating team, environmental needs, and diverse services were significant hospital-related needs. Awareness, accessibility, availability, and affordability of treatment services were the major community-related needs.
Conclusion:
The study highlights diverse needs extending from individual to community among people with AUDs. A holistic treatment model to address these needs will improve the quality of care and treatment outcomes.
The treatment needs of patients with severe alcohol use disorders (AUDs) were assessed using a qualitative study design. Interviews revealed four major themes: individual, family, hospital, and community-related needs. The study underscores the importance of a holistic approach to enhance care and outcomes for individuals with AUD.Key Message:
Globally, alcohol use is the seventh leading risk factor for both deaths and DALYs (disability-adjusted life years). 1 In India, per-capita consumption of alcohol has increased over time, along with the risk of its public health impact. 2 Besides, the treatment gap for alcohol use disorders (AUDs) is 86%. 3 The relapse rates among untreated patients with AUDs are high. 4 Although the relapse rates are lower among those treated, they remain significant. In India, a recent systematic review of the relapse rates across treatment centers reported a range of 3.4%–90%. 5
AUDs are associated with problems in multiple life domains, including physical, psychological, family, social, and legal. This leads to a vicious cycle of problems. 6 Among treatment-seeking populations, these domains form the “treatment-related needs.” “Need” is the requirement of the individual that enables them to achieve, maintain, or restore an acceptable level of social independence or quality of life. 7 “Need” is the discrepancy between the current and desired states. 8
Globally, and more so in low-middle-income countries like India, a smaller number of studies have been conducted to understand the needs of people with AUD. In an Indian study exploring the treatment needs, Thomas et al. 2018 found that women with AUD have unique treatment needs and barriers. 9 In the study, the authors identified (a) the quality of therapeutic relationships, (b) addressing the stigma and discrimination from the health care system, (c) support needs, and (d) informational needs as major needs for women with AUD. Addressing these issues may help design or develop specific psychosocial interventions for women with substance use disorders (SUDs). 9 Focusing on the needs of people with AUD improves treatment outcomes. Besides the Indian study mentioned above, there has been no qualitative evaluation of the treatment needs for AUDs. Hence, this study will address the research gap in understanding the treatment needs among people seeking treatment for AUD. The objective of the study is to qualitatively explore the treatment-related needs of individuals with severe AUD admitted in a tertiary care setting.
Material and Methods
A qualitative, in-depth interview was conducted to assess the treatment needs of patients with severe AUD. The study was conducted at the National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, a tertiary care treatment center in southern India.
Participants admitted to the treatment center were invited to participate in the study using a purposive sampling method. The sample size was kept flexible, and the study was stopped once the thematic saturation was attained. Both currently admitted and patients admitted in the past were interviewed for the study. Patients diagnosed with severe AUD as per DSM-5 were included in the study. Patients who were acutely sick and unable to provide consent were excluded from the study.
A semi-structured questionnaire with socio-demographic details, clinical profile, and anchor questions was prepared for the qualitative interview. An extensive literature review and key informant interviews were conducted with addiction experts to prepare the questionnaire (see supplementary text). After written informed consent, patients were interviewed by VLN alone in a standard interview format. VLN is a male psychiatrist by training (MD in Psychiatry), had a Post-Doctoral Fellowship in Addiction Medicine, and had 3 years of Addiction Medicine experience following post-graduation at the time of the study. VLN had a special interest in Addiction Psychiatry, undergoing specialty training in Addiction Psychiatry. The questioning pattern was flexible to accommodate different responses and observations that were noted to enhance the interview quality further. The interviews were audio recorded to avoid loss of data/recall bias, to get exact data as experienced by the subjects, and to avoid interpretation bias of the researcher. The participants had yet to have prior contact with the researcher before the study.
The recorded interviews were initially transcribed in the language of the interview and then translated into English. Following translation, the interviews were re-read, and color coding was done to synthesize factors. The coding was done manually. Representative quotes were selected for each of these factors. The quotes and codes were reviewed independently by the researcher and one of the co-authors to reduce bias. The thematic inductive analysis was done as follows: the researcher examined the verbatim coded files generated independently by two reviewers, and the data triangulation was done. Themes and subthemes were generated and categorized for interpretation.
The institutional ethics committee approved this study (No. NIMH/DO/IEC(BEH.Sc.DIV)/2018 dated 12.04.2018), and written informed consent was taken from all the patients interviewed.
Results
Socio-demographic and Clinical Profile
Fifteen patients were approached for participation in the study, and all of them agreed to take part. Interviews lasted for 45–60 minutes each. Most of the patients were male and below the poverty line, and clinically, all the patients had severe AUD. The socio-demographic and clinical details are described in Table 1.
Socio-demographic and Clinical Details of the Patients Interviewed.
Qualitative Data Synthesis
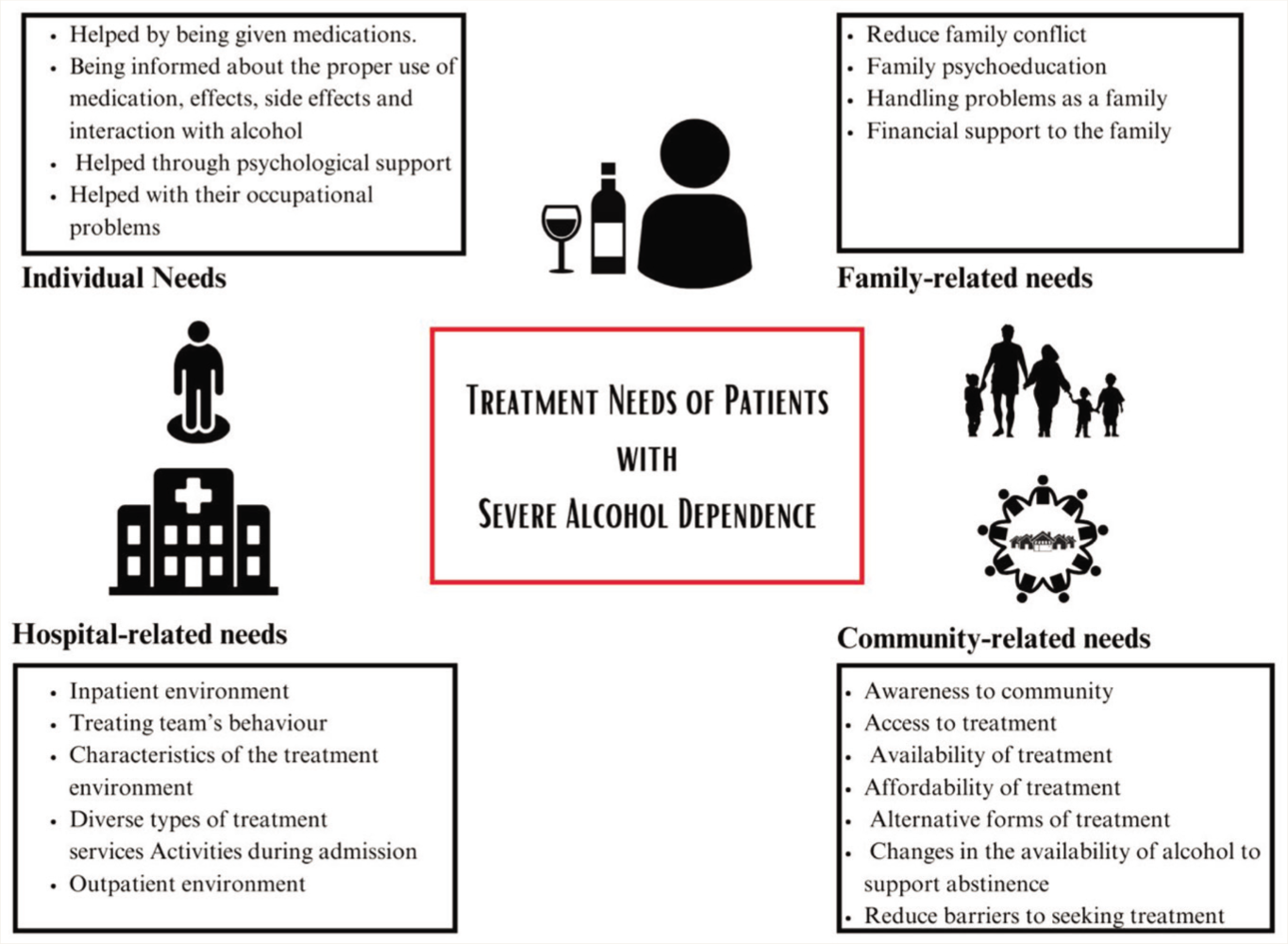
The thematic inductive analysis of the qualitative interviews identified four predominant themes regarding their treatment-related needs. These include:
Individual related needs Family-related needs Hospital-related needs Community-related needs
Individual Related Needs
The patients expressed multiple needs regarding their individual problems. They expressed the need for medication and its appropriate use, as well as psychological and occupational needs (see Figure 1 subthemes under individual needs).
Themes and Subthemes Generated During the Thematic Inductive Analysis of Qualitative Interviews.
A well-educated woman said-
Librium helped me to relax. Otherwise, I would keep on pacing here and there. I had read that Librium can be addictive. I would like to know the side effects.
A young patient who was admitted for his alcohol-related health emergency expressed
I need treatment such that even during parties, if I take alcohol, I should not get any problems. I know that there is a tablet that produces vomiting, but I do not want such kinds of tablets. Once a week, they will make nonveg. (non-vegetarian). At that time, I might take alcohol, so I should not get any problems.
A patient who works as a truck driver said
When we go with friends, there will be a party, as we are drivers. Then, it is difficult to say NO. We might take some alcohol for my friends’ satisfaction. In counseling, they should discuss this. They should tell us how to avoid the situation, like how to avoid invitations.
Another patient highlighted the need for help related to work
If I am tensed, then I feel depressed… then I go for alcohol… then I will not go to work. I used to go to work regularly and earn 900 rupees daily. Now, I am not earning. For six months, I have not been working. I have debts, so I wonder whether financers will come and scold me or beat me. Because of this tension, I take alcohol early in the morning. I would be waiting for morning; even before I brush, I take alcohol. I need help to go back to work again.
Another patient who felt some help is required to prevent relapse due to anger reported:
Counselling is needed to control anger. Whenever I feel tense and go with friends, I will take alcohol. So, I need alcohol to control this.
A patient with multiple relapses and admissions expressed about the group therapies:
Evening group meeting is needed, as it will help people to open up, they will tell their experiences, we will tell ours. When they share, we will feel that such problems happen to us. Then some people will listen, some may not, but it will help.
Under each subtheme, patients expressed multiple needs that they felt were important to them during the process of recovery from their AUD (see supplementary text). For example, under the subtheme help with medications, sub-subthemes like help related to withdrawal, physical symptoms, and psychological symptoms were expressed.
Family-related needs
Several patients raised the need to address family-related issues while addressing their alcohol-related problems, as they contribute a major part during their recovery. Patients expressed a need to reduce family conflict, which includes improving trust, communication, and love and reducing worries in the family; educating family members about the problem; helping the family as a whole; and addressing financial concerns (see Figure 1 subthemes under family needs).
During the interview, a woman said
I expect my family members to trust me. Nobody is perfect. I can have a relapse. Just one incident should not make them lose their trust. We understand it is an illness and must be treated. They do not understand. My mother stopped talking to me. She would talk to the kids when I was around so I would hear. Nevertheless, she would not talk to me. I told them- this is not going to help. It is going to make it more difficult.
Another patient who was worried about the frequent relapses said
It is very important for you to tell my family members about treatment. They know that we should not stop taking tablets even if we drink. Doctors have talked about these things to all my family members. Sir, if I take medication even after I drink, the next day, I will be fresh and go to work. if I do not take medication, then I will have some withdrawal symptoms, so it is important to take medication… you have to insist to my family not to stop medications.
A woman concerned about her husband taking alcohol highlighted his treatment as an essential part of her recovery
Give treatment to my husband. Please give courage to my husband about stopping alcohol. Also, advise my husband to stop violence against me, like beating and scolding.
One patient who comes from a long distance and a below-poverty-line family expressed
Whatever might be the difficulty, you bring to treatment immediately… that needs to be said to the family… It would help if you gave subsidized treatment … sometimes you need confidence to give treatment even without money… Oh! I do not have money…. tomorrow we will go… that is why they do not come… it happened to me twice… what will happen is if they do not come early, their health will worsen.
Hospital-related needs
Among hospital-related needs, many patients expressed the need for specific features in inpatient and outpatient services. More specifically, they highlighted the importance of treating team behavior and having activities during admission to the hospital (see Figure 1 subthemes under hospital-related needs).
A patient who had multiple episodes of relapses and hospital admissions expressed
Privacy is a major issue. Last March, I was talking about family issues, and another doctor was talking to a patient in the same room. I said that I would not tell; there is a patient here. Then she said that he was also a patient and that talking was okay. I do not want to tell in front of him! Doctors should respect patient privacy. If you sit and talk and make a joint decision, then 90% guarantee it will work. If you understand us, then it will work. If you do not collaborate, then it will not work.
Another patient said
Treating should be cool. Understand the patient’s condition slowly, not fast. It may be over 15 days or over one month, and slowly discuss it with the patient. Coolness is more important.
One patient visiting OPD after discharge from the hospital reported
If there is a contact person when we come to OPD, then I will get some help. I came to OPD at 8:30 and was sitting in the OPD. I was quarreling with my mother; my mother gave me 100 rupees. I went to the shop, had alcohol, and went. When I am distressed, if there is one number to contact, it would help me.
Community-related Needs
The patients expressed availability, accessibility, affordability, and awareness related to treatment at the community level. Further, the need for alternative forms of therapy and changes in the availability of alcohol were also highlighted (see Figure 1 subthemes under community-related needs). Finally, they also expressed a need to reduce barriers to seeking treatment, like stigma among women and fear of being judged while seeking treatment.
During the interview, a patient expressed the following about the local treatment
At my home, there is Dharmasthala sangha (local treatment) … where they will make us stop alcohol, they do not allow us to go home. There, I might escape from there. It is a good place. Many people change. It should be there everywhere. We need to stay there for 1.5 months. It is a stable place. Some people stopped alcohol and restarted again. I was about to join the Dharmasthala Sangha. There, they will give medication, it seems. My friend told me to go there multiple times. However, I did not go there. I believe more of these kinds of treatment (like dharmasthala sangha) should be provided.
One patient expressed his views on policies related to alcohol and said
The government should ban alcohol. Drinks should be costly! Fifty rupees of alcohol should be sold for 500. If you sell liquor cheaply rather than drinking tea, people drink alcohol.
A patient who did not have a treatment facility at his local place mentioned
At my local hospital, if there are similar kinds of doctors, then it will be helpful to me. At my place, doctors will be fearful of treating alcohol patients as they think we cause some harm. They do not see regularly.
Discussion
This study adds to the limited research on treatment needs perceived by patients with AUD. Four themes were prominent. These include the needs expressed by the patients for their problems, the needs expressed by the patients for problems related to their family, the needs expressed by the patients related to the hospital environment, and the needs expressed by the patients related to the community in which they live.
Individual Related Needs
This was the most common theme that emerged during the interview. Interviews highlighted the need for handling withdrawal and craving with pharmacological support. It has been well understood that these symptoms are distressing and can affect the motivation to stop alcohol. Both animal and human research indicates that allostasis (due to chronic use of alcohol) in the brain requires pharmacological treatment to prevent lapses and relapses.10,11 Further, the participants also expressed a need to know about the side effects of the medications and their interaction with alcohol. A known practice in the Indian context is the surreptitious administration of disulfiram and consequent disulfiram-ethanol reaction. 12 Hence, it is essential to explain to patients about the effects, side effects, addictive potential, and interactions of the medications prescribed. This would improve compliance with the prescribed treatment. 13 and discourage use without medical advice. The need for psychological support and occupational help has been emphasized by many participants, especially to handle craving for alcohol to control their emotions like low mood, anger, and day-to-day stress, etc. A range of psychological interventions (evidence-based) should be made available for patients with AUDs. 14 Furthermore, incorporating occupational therapy components in the interventions can improve outcomes among alcohol users. 15
Family-related Needs
The needs related to family, like family conflict, family psychoeducation, increasing support for the family members, and treatment of spouse alcohol use, especially in husbands of women with AUDs, should become a part of the treatment programs. Wide use of family-focused interventions to address family-related needs in routine practice has been recommended. 16 The family-related needs expressed in our study echo those of Copello et al. 2005, including helping the family access treatment, addressing family issues jointly, and intervening in the family members’ concerns. 16 In India, where families are close-knit, having a member with AUD largely affects the family. Chronicity of the problem results in a state of codependency in the family. The prevalence of codependency is seen in half of the spouses in the Indian context. 17
Notably, among women with AUDs, addressing family needs determines the treatment outcomes. While women’s psychological needs differ from men’s, needs relating to child care and protection are additional unique needs that require attention. 18 Furthermore, the relapse prevention model of treatment, identifying and treating the interpersonal determinants of relapse, is an essential component of therapy. 19
Treatment Environment-related Needs
Participants needed a conducive treatment environment during admission and outpatient visits. The climate of the treatment environment is minimally studied in SUD research. Previous research suggests that organizational factors are important in determining treatment effectiveness. 20 Further, service structure, staffing, physical environment, psychological safety, and handling issues such as sexual assault have been identified as important needs. 21 Supportive staff and a goal-directed work environment were associated with better treatment engagement, patient satisfaction, outcomes, and enhanced follow-up care. 22
A consistent relationship has been established between therapeutic alliance and treatment outcomes. 23 As a part of the therapeutic alliance, participants highlighted the need for privacy and confidentiality while on treatment. In multiple examples cited by the respondents, such as interviewing two patients in the same room, calling out their names publicly can lead to a breach of privacy and increase the stigma. Further, confidentiality brings another dilemma for clinicians in the Indian context, as most patients do not want to disclose AUD-related problems to their family members or significant others. These include breakups in relationships, suicidal or homicidal thoughts, criminal history, history of sexual abuse, the status of blood-borne infections, and substance use among professionals carrying weapons (like border security forces). Compared to the Western population, where treatment is through the state and legal services, the family is the primary caretaker in seeking treatment in India. 24 Especially when family members bring persons with AUD for treatment, their expectation of being aware of and involved in the person’s care further complicates issues of this nature.
Respondents also mentioned the need for non-coercive treatment with collaborative decision-making, which brings in the issue of “Autonomy,” the core ethical principle. In India, it was noted that patients were forcefully admitted to rehabilitation centers, were beaten up if they did not comply with the rules and regulations, and were asked to do the chores they otherwise did not want to do. These highlight the need for following ethical principles (including autonomy, beneficence, non-maleficence, justice, and respect for people) while treating patients with AUD. 25 Following these principles becomes quite challenging for clinicians in certain situations. Some of the respondents, when admitted during the alcohol withdrawal delirium, would wish to end their consent to care once they are better physically. Still, the family insists on treating their AUD due to fear of relapse. Despite motivational interviewing, most patients tend to withdraw their consent. In such a scenario, the dilemma between respecting the patient’s autonomy vs continuing care for AUD based on the family’s request is not uncommon. The onus of implementing an ethics-based treatment falls on the treating team, which has a collaborative relationship with the patient and family. Although it is a common scenario for family members to request admission against the patients’ will or request for surreptitious medication, this will breach the autonomy when treatment is given without the patient’s informed consent. It is common practice that patients receive disulfiram or related drugs (prescribed by the faith healers, through television advertisements, from local pharmacists) without their knowledge. Most patients reported that they do not wish to take such kinds of drugs or do not want their family members to give them such kinds of drugs surreptitiously. This is supported by the evidence that involuntary treatment is not associated with increased post-treatment abstinence from alcohol. 26 Overall, reformulating the needs of persons with AUD reminds healthcare professionals to provide ethics-based treatment.
Women expressed the need for separate treatment facilities rather than combined treatment facilities. The expressed needs resonate with the global appeal for providing gender-sensitive and woman-only treatment services.21,27 Among the few Indian studies that assessed the needs of people with SUDs, Thomas et al. 2018 qualitatively assessed the needs of women seeking treatment for SUDs. 9 Though our study echoes the previous one, some differences in themes emerged. Addressing stigma at the level of healthcare providers and emotional and informational needs during treatment was emphasized in the previous study. The need for subsidized treatment, therapeutic relationships, and quality of treatment were common themes in both studies. However, individual physical needs were greater in our study. One reason for this difference is that our study included primarily men, whereas the previous one included only women. This difference may be due to variations in the pattern of substance use and the specific needs of different genders.
Patients with AUDs suffer from a higher range of physical and mental health co-morbidities.28–30 Most patients expressed a need for handling physical and psychiatric co-morbidities and managing alcohol dependence. Consistent with the needs expressed, evidence suggests that the integrated treatment for SUDs is superior to individual problems separately. 31
Study participants below the poverty line expressed a need for free and subsidized treatment funded by government agencies. Based on preliminary evidence, most people do not seek treatment due to financial constraints. Some respondents expressed a need for an insurance facility to treat addiction. Others believed that having insurance may encourage people to drink alcohol. The availability of insurance improves access to treatment. 32 Policy changes have been associated with an increase in the coverage of insurance for SUDs, but treatment-seeking remained low. 33 Therefore, in developing countries like India, there is a need for more policy studies to generate evidence regarding insurance for addiction treatment. 34
Many patients expressed a need for continuity of care once discharged from the hospital. As observed from the previous studies, substance use treatment is a long-term process that can extend from months to years. 35 Hence, providing continuity of care is important for persons with AUD. 36
Community-related Needs
Respondents expressed a need for improving access to care in the community to seek treatment, with various interventions like improving awareness, making treatment available locally within the community, and affordable care. They also expressed a need for alternative culturally acceptable therapies in the community and conventional treatment. Despite the availability of treatment services, a lack of community awareness prevents treatment-seeking. 37 Therefore, it is crucial to promote the availability of treatment.
Finally, they expressed multiple barriers to seeking treatment and that overcoming these barriers was a critical need that should be addressed to improve access to treatment and care. Some patients expressed a need for interventions at their workplace. Workplace interventions were found to help improve accessibility for treatment. 38 In a workplace prevention program and activity done in a bus organization in Karnataka, it was found that there was a significant reduction in substance use and an improvement in health parameters and work productivity. 39 Most of the needs expressed by the respondents are within the service requirements described by the World Health Organization as Availability, Accessibility, Acceptability, and Quality (AAAQ). 40 People living in below-the-poverty-line communities expressed the need for a change in the policies related to the availability and accessibility of alcohol, which would help them stop alcohol. Higher alcohol outlet density has been associated with excessive alcohol and related harms.41,42 Evidence suggests that reducing alcohol outlet density can reduce alcohol-related harms. 42 Moreover, restricting the increase in sale timings of alcohol by 2 hours was associated with a reduction in alcohol-related harms. 43
Limitations of the Study
The study was conducted in a government tertiary care setting; all the patients interviewed had severe AUDs. Hence, we might have missed understanding the needs of a broader spectrum of AUDs. Even in earlier studies, it was observed that people with severe SUDs had greater needs than those with less severe forms of the disorder. 44 In our study, half of the participants were from below the poverty line, that is, a disadvantaged group. The disadvantaged groups, despite consuming lesser or similar alcohol, suffer higher alcohol-related harms compared to advantaged ones (called the Alcohol Harm Paradox [AHP]). 45 Hence, the number and the dimensions of needs expressed in our study might be high.
Conclusion
The study highlights the diverse needs of patients with severe AUDs. These diverse needs to be considered to improve the quality of treatment services in existing treatment centers. Furthermore, the study provides insights into developing an ideal addiction treatment center and the community’s need for continuity of care. Developing and validating a standardized tool to assess the needs of patients with AUDs will help in individualized interventions. Given the dynamic nature of alcohol use problems, needs should be periodically assessed in the hospital and the community. The treatment approaches should be constantly evaluated and modified to meet the needs of people for whom they are intended- persons with substance use. Finally, policies related to treating AUDs need to be modified based on the community’s needs for the hospital. Further studies are required covering the spectrum of AUD patients to understand their needs better.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
No generative AI was used in the study, and the authors take full responsibility for the entire content of the manuscript.
Ethical Approval
This study was approved by institutional ethics committee (No. NIMH/DO/IEC(BEH.Sc.DIV)/2018 dated 12.04.2018).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.