
Abstract
Backgrounds:
Research shows that medical students’ knowledge and skills concerning the assessment of cognition in various neuropsychiatric conditions (e.g., Alzheimer’s disease and schizophrenia) are unsatisfactory. This research aims to conduct a training needs analysis (TNA) for medical students to identify and refer patients with neuropsychiatric conditions.
Methods:
The study comprised two phases. First, developing a TNA toolkit to assess training needs in clinical tasks related to cognitive function assessment (by adopting the Hennessy–Hicks TNA toolkit); and second, through a self-reported survey, their training needs in cognitive function assessment were assessed. Data analysis involved calculating training gaps, importance scores, performance scores, training scores, and organization scores for various clinical tasks-stratified participants’ study year; for training needs and trends, factor analysis and post-hoc analyses were conducted.
Results:
A total of 153 medical students from a tertiary care center participated in the survey. The participants rated their performance lower than the perceived importance of tasks, indicating a need for improvement in all competencies (P < .01). Pre–final-year students had the highest training needs, particularly in accessing literature, planning, and organizing care for patients with cognitive impairment, performing mental status examination, screening patients for cognitive deficits, and counseling them/caregivers about interventions (P < .01). Factor analysis identified a single dominant factor, suggesting a correlation among these skills.
Conclusion:
Pre–final-year students require targeted training, whereas students beyond this stage can benefit from special training modules and awareness of available resources for cognitive assessment. The findings also suggest the importance of a hybrid approach involving training and organizational modifications.
Keywords
Identified significant training gaps in assessing cognitive functioning among medical students, emphasizing curriculum enhancements. Highlighted the need for specialized training for pre–final-year students. Recommended adding a competency on cognitive decline assessment to the curriculum.Key Messages
Out of the 47 million individuals worldwide grappling with dementia, 63% reside in low- and middle-income countries (LMICs). 1 For instance, in India, the current count of individuals with dementia stands at a minimum of 5.3 million, and this is anticipated to double by the year 2035. 2 Diagnostic and Statistical Manual of Mental Disorders, fifth edition categorizes cognitive disorders as mild and major neurocognitive disorders. 3 Mild cognitive impairment (MCI) has an adjusted overall prevalence of 16%, is highly prevalent in the elderly, and increases with age over 60 years. 4 A systematic review involving 35 studies examining the association between MCI and deficits in instrumental activities of daily living (IADL) showed that patients with MCI exhibit IADL deficits, particularly in areas requiring higher neuropsychological functioning, with financial capacity being consistently affected. 5 Cognitive impairment in young individuals can often be associated with medical conditions like anemia or psychiatric conditions like major depressive disorder. 6
Mental health conditions often involve cognitive dysfunction, which can be overlooked in clinical practice. 7 In today’s rapidly evolving healthcare landscape, equipping medical undergraduate students with the necessary skills for clinical evaluation is paramount. The Indian National Medical Council (NMC) has proposed a new competency-based curriculum for undergraduate medical students (henceforth medical students). 7 The curriculum for psychiatry describes competency for the mental status examination (MSE) by the Mini-Mental State Examination (MMSE). 7 Additionally, the curriculum for physical medicine rehabilitation enlists the ability to describe and discuss cognitive decline. 8 While the curriculum is appreciated for enlisting cognitive dysfunction assessment as one of the important competencies that medical students should master, it is vague in that it does not describe specific competencies in evaluating cognitive functioning.
The MSE of a patient is an amalgamation of evaluation of general appearance and behavior, psychomotor activity, speech, thought process and content, perception, sensorium, attention, concentration, memory (basic cognitive functions), intelligence, executive functioning, abstraction, judgment, and insight (higher cognitive functions). 9
Training needs analysis (TNA) is a powerful tool to identify the needs of the students, professionals, or service staff concerning a task and arrange adequate training for them so that their learning or work efficiency can be enhanced, including preventing unnecessary training in some areas. Such research has brought valuable insights into the business, marketing, engineering, and health sectors.10-12 For instance, a study from a multispecialty hospital in India assessed the training needs of the nursing staff concerning patient care, human resources, inventories, and reporting system management, and found out that the health personnel were well trained in all the domains; however, they needed training in the effective use of technology in the medical field. 10 Another pan India research involving the managers of the noncommunicable disease (NCD) program identified that the managers required training on communication skills, inventory and finance management, standard protocols on illness management, and reporting and referral system. The authors emphasized that such analysis helps perform need-based effective staff training for effective program implementation. 12
Despite the robustness of the TNA-based assessment and intervention, this tool has been used sparingly in medical education in India. This prevents access to the pupils’ training needs, thereby ineffective teaching and training or competency attainment.
As mentioned above, cognitive function assessment is a vital competency for medical students as it cuts across disciplines to assess and treat individuals suffering from neurocognitive problems effectively. To address the gap in medical training, we propose the addition of “Screening, Assessment, and Referral of Patients with Cognitive Decline” as a competency (encompassing psychomotor, knowledge, and attitude domains) in the NMC’s medical students curriculum. To determine the specific training needs and curriculum requirements, we conducted a TNA using the Hennessy–Hicks TNA toolkit developed by the World Health Organization (WHO). 13 This toolkit, widely recognized for its psychometric robustness and adaptability, allows us to tailor the training module to meet clinical needs effectively (detailed below). The primary objective was to develop a TNA toolkit to assess medical student’s competency in assessing cognitive function in an individual. Second, conduct a self-reported survey with medical students to identify their training needs for assessing cognitive functioning.
Material and Methods
This study was conducted at a tertiary care teaching institute in central India from June to August 2023, with approval from the Institutional Human Ethics Committee (IHEC No. IHEC/2023/LOP/IL0108). Participants included MBBS students from the second, pre-final year, final year, and interns, all of whom had clinical exposure from at least the third semester (from the beginning of the second year in the MBBS course). However, students before their third semester and without informed consent were excluded. They were recruited through an orientation session about the study, after which they obtained their informed consent. The survey, distributed via Google Forms post psychiatry classes, collected no demographic data and focused instead on the year of study.
Process of the Toolkit Development
We used the “Clinical Task” domain of the Hennessey–Hicks TNA toolkit in our study to address tasks specific to cognition assessment (Table 1). There are six items under the “Clinical Task” domain; under each item, there are four questions (Table 2). The toolkit allows for modifying items without compromising the questionnaire’s validity and allows the researcher to add 10 items or change 25% without compromising validity. We adopted all six items from the “Clinical Task” domain and modified them for tasks about cognition. 13 Our adaptation process involved collaboration with mental health professionals, including psychiatrists and psychologists, and public health experts from our institute. The framework for this customization drew inspiration from the cognitive assessment module in the Oxford Handbook of Psychiatry and the mental health examination module from AMBOSS.14,15
The response rate was calculated by comparing the number of survey respondents to the total enrolment in the MBBS program. To identify training needs, the research team analyzed the survey’s average scores using two primary methods: (a) detecting statistically significant differences between importance and performance scores and (b) calculating the average training gap across all items, defined as the positive difference between importance and performance scores. 13
Adapted WHO Hennessey–Hicks Training Needs Analysis.
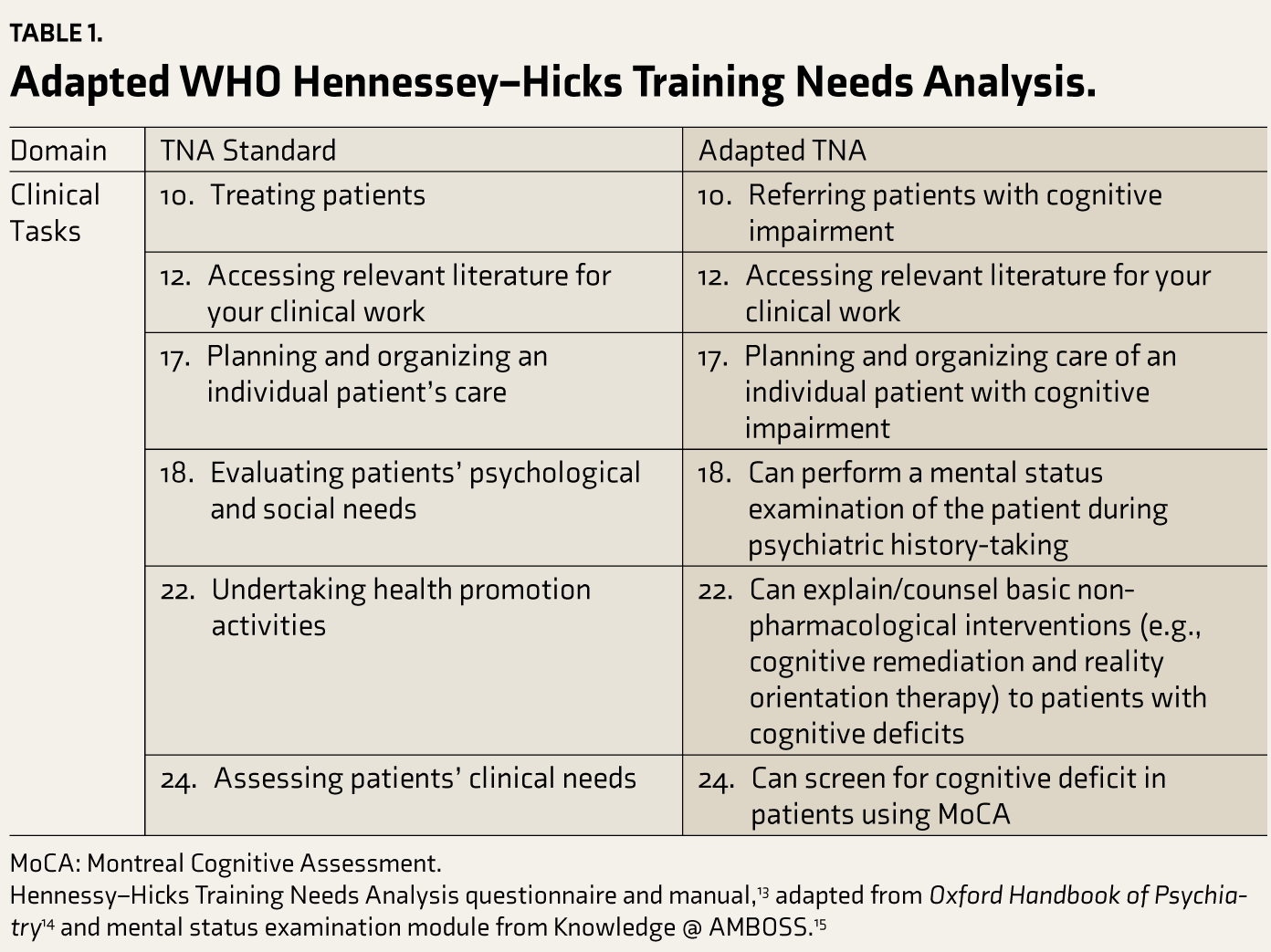
MoCA: Montreal Cognitive Assessment.
Hennessy–Hicks Training Needs Analysis questionnaire and manual, 13 adapted from Oxford Handbook of Psychiatry 14 and mental status examination module from Knowledge @ AMBOSS. 15
Clinical Task Domain Self-Assessment Likert Rating Scale.
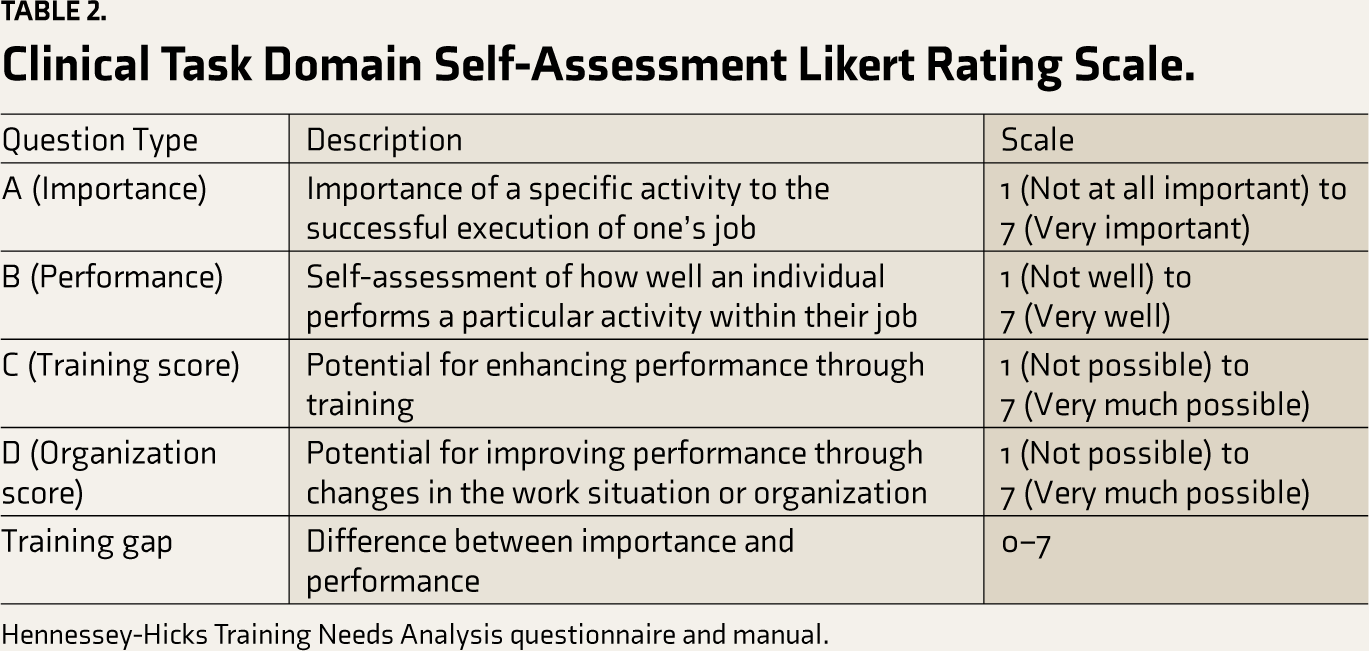
Hennessey-Hicks Training Needs Analysis questionnaire and manual.
A subgroup analysis was also performed to examine the relationship between training needs and the academic year, employing the analysis of variance (ANOVA) test. Student’s t-tests were applied to normally distributed data, while Mann–Whitney U tests were used for data that were not normally distributed. Factor analysis was then performed specifically on the training gap data. The purpose of using factor analysis was to ascertain whether the adapted items could be grouped under a single curriculum topic or if they represented distinct competencies, necessitating separate instructional approaches. χ 2 and Barlett’s tests were done to confirm the appropriateness of the data for factor analysis and to validate that the extracted factors meaningfully represent the structure of the data.
Further analysis aimed to determine the need for organizational changes in addition to addressing training needs. This involved (a) evaluating the significance of the differences between perceived training scores and organizational scores and (b) using grids for a visual comparison of these scores. Training needs were assessed by comparing importance–performance and training-organization scores through these grids, which helped identify significant training gaps. 13
Results
Demographic Overview and Career Characteristics
The questionnaire was distributed to 600 students of which 25.5% (n = 153) formed the part of the study. The demographic data present a diverse range of preferences and career goals among medical students. Among the preferred types of medical practice, academic roles (n = 60, 39.22%) and private practice (n = 54, 35.29%) stood out. Interns, final year, pre–final (third year), and second-year MBBS students constituted 13.07% (n = 20), 5.23% (n = 8), 49.02% ( n = 75), and 32.68% (n = 50), respectively. Regarding practice location preferences, 16.34% (n = 25) preferred to be abroad, whereas 83.66% (n = 128) chose to be in India.
Training Needs Analysis of the Adapted Toolkit
Across all items, there is a consistent pattern where participants rate their performance lower than the perceived importance of tasks, suggesting that there is room for improvement in all competencies and that training needs analysis should be done. The difference between the “Training Score” and “Organization Score” is insignificant, necessitating a change in both (Table 3).
Training Needs Analysis of the Adapted Toolkit.
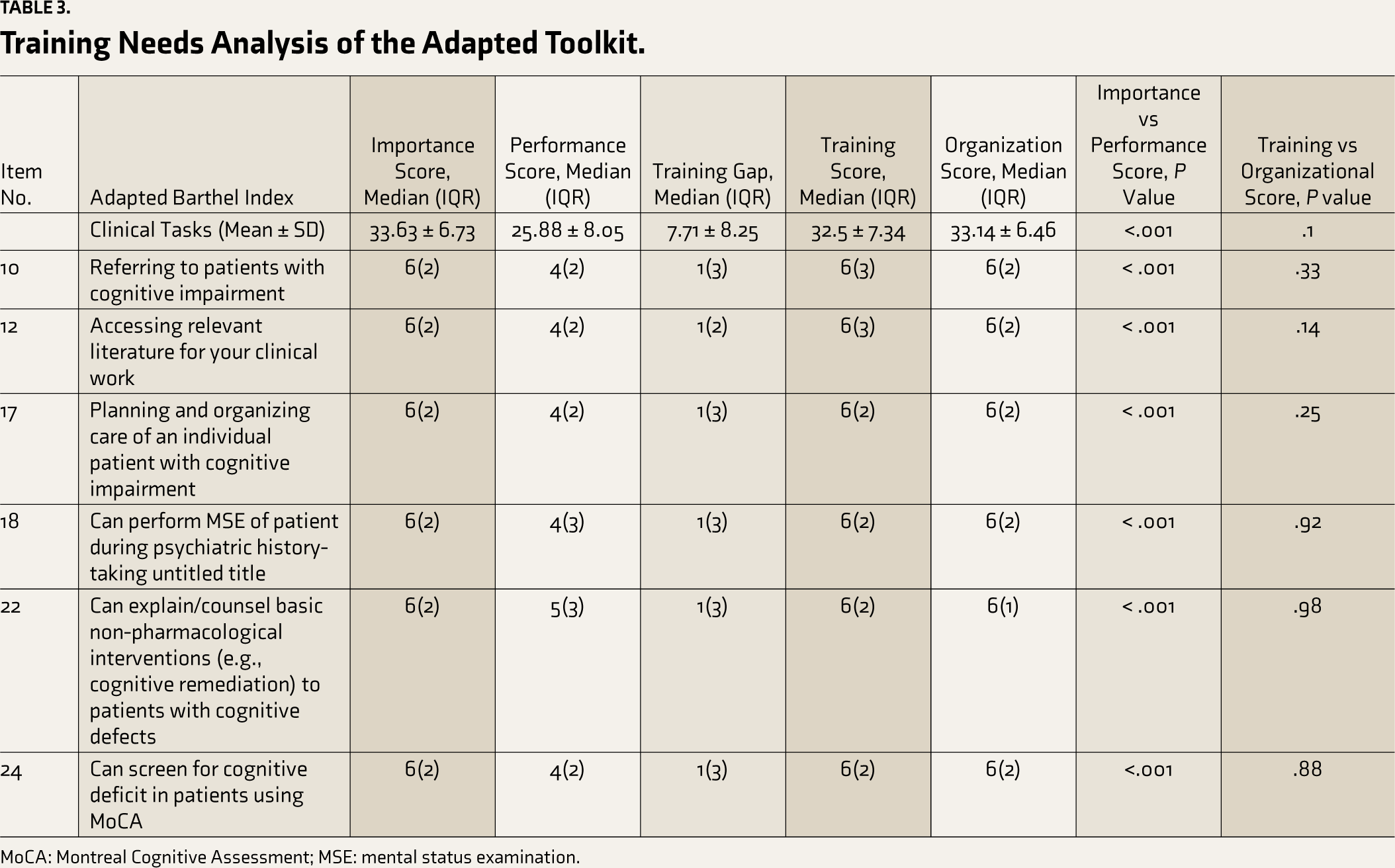
MoCA: Montreal Cognitive Assessment; MSE: mental status examination.
Importance–Performance Analysis and Training Score Versus Organization Score Analysis on Training Needs Analysis
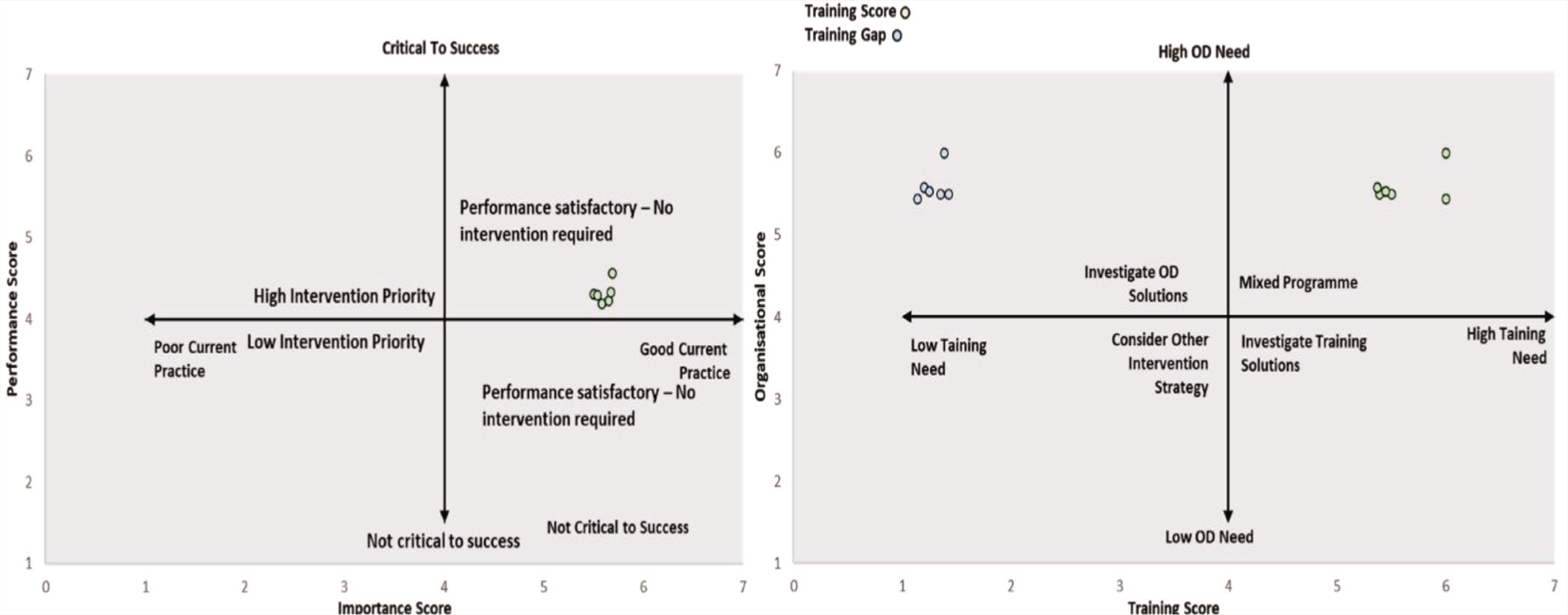
When constructing the “Importance–Performance Grid” based on the average scores of all 30 items, it was evident that all items exhibited elevated importance and performance scores. This finding suggests that no immediate training intervention is required. Conversely, when generating a grid between training and organizational aspects using the average of all six items, it became evident that all items received high training and organization scores (Figure 1). This indicates a hybrid approach requiring organizational modifications and training programs. Furthermore, a sequence of statistical tests conducted between the categories of importance and performance demonstrated significant differences for all the items, underscoring a notable training need (Table 3).
Importance vs Performance Grid, B: Training Score vs Organization Score (OD) Grid.
Year-wise Subgroup Training Needs Analysis
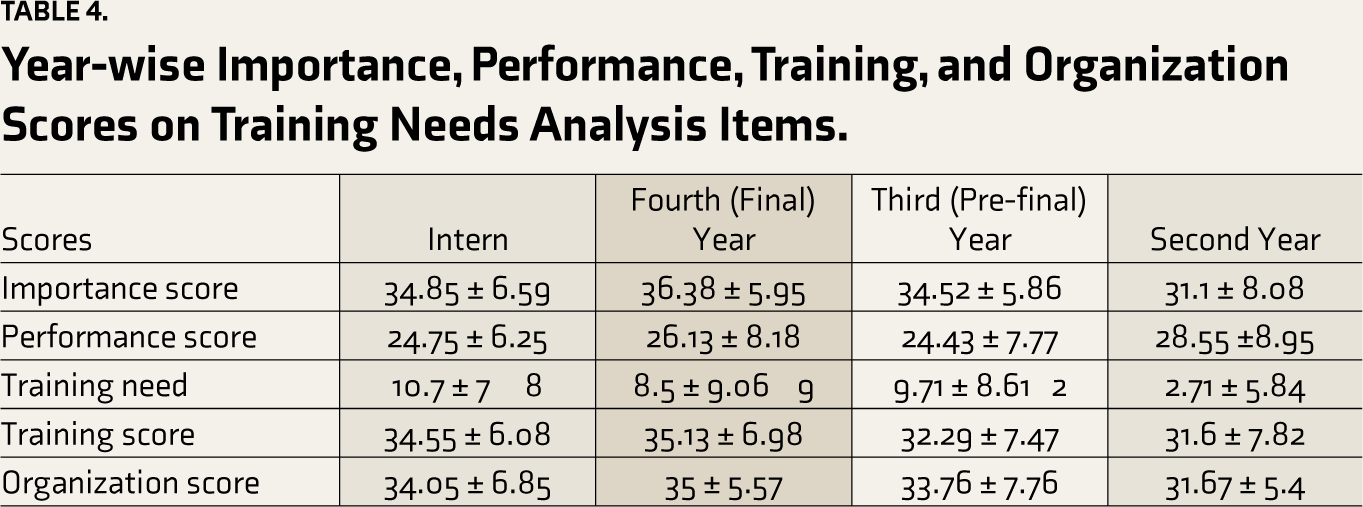
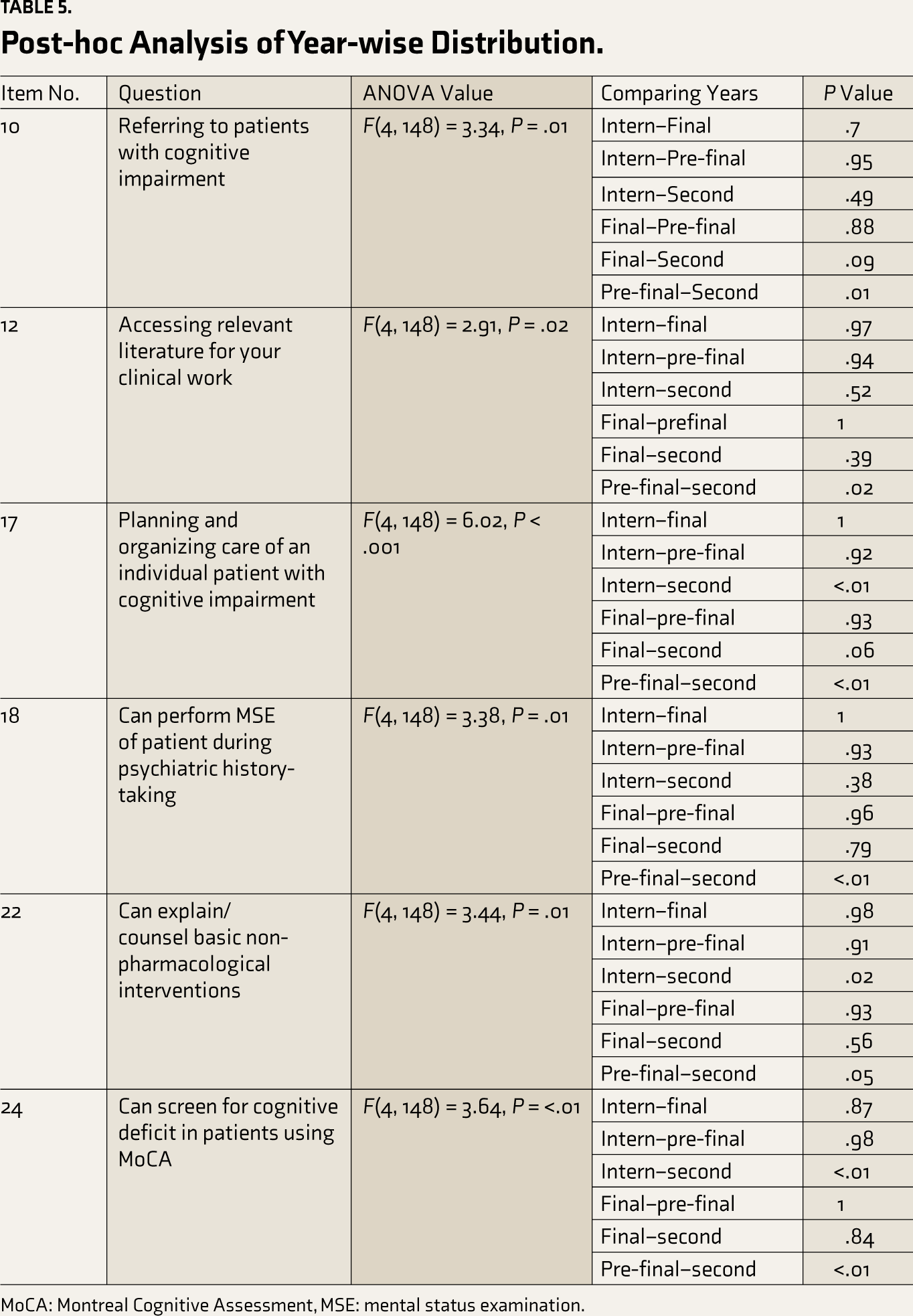
In all clinical tasks, fourth-year students again emphasize the importance, whereas second-year students reportedly perform well in performance scores. Pre–final-year students show higher training needs, indicating an area for potential skill development (Table 4). Final-year students and interns report higher training and organization scores. The training gap varies significantly among second- and pre–final-year students (Table 5). Significant differences in the training gap between different years of medical school were present for planning and organizing care of an individual patient with cognitive impairment, which can screen for cognitive deficit in patients using Montreal Cognitive Assessment (MoCA). No significant organizational difference has highlighted a need for more specific curricula and incentivization.
Year-wise Importance, Performance, Training, and Organization Scores on Training Needs Analysis Items.
Post-hoc Analysis of Year-wise Distribution.
MoCA: Montreal Cognitive Assessment, MSE: mental status examination.
Factor Structure of the Training Needs Analysis
Bartlett’s test confirmed the suitability of training needs for factor analysis (χ² = 604.31, df = 15, P < .001), with subsequent chi-squared tests showing statistical significance (χ² (9) = 20.57, P = .01), validating the factor analysis model. Analysis, including both unrotated and rotated solutions, identified a single dominant factor (Factor 1) explaining a significant variance (proportion variance = 0.66), suggesting the assessed skills are interrelated and could be consolidated into one module (Table 6).
Factor Loadings of Training Needs.
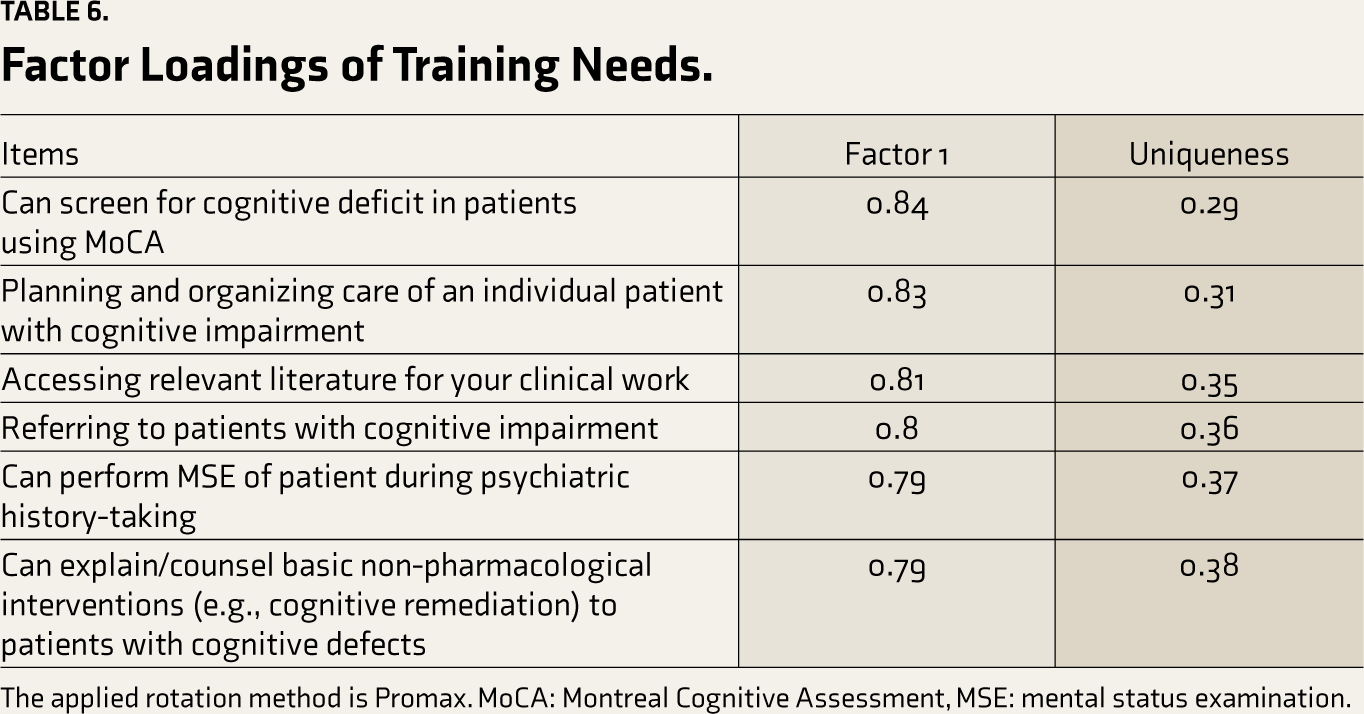
The applied rotation method is Promax. MoCA: Montreal Cognitive Assessment, MSE: mental status examination.
Discussion
In this study, our primary objective was to assess the training or organizational need to prepare medical students for the clinical evaluation of cognitive dysfunction in individuals. By doing so, we aim to enhance their confidence, knowledge, and readiness for the complexities of cognitive evaluation in healthcare. 16 To achieve our objective, we used the Hennessy–Hicks TNA Questionnaire, which has demonstrated robust psychometric validity and has been widely utilized.17-25
Medical students demonstrated substantial gaps between their self-assessed performance and the perceived importance of clinical tasks related to cognitive function assessment. This gap indicates a critical need for enhanced training in all assessed competencies, particularly for pre–final-year students with the highest training needs. Factor analysis identified a single dominant factor explaining a significant proportion of variance (66%). This suggests that the assessed skills are interrelated and could be consolidated into a comprehensive training module. The analysis found training needs and organizational changes, indicating that more than addressing the training gaps is needed.
There is a paucity of studies on knowledge, attitude, and practice among Indian medical students on assessing cognitive decline. Despite the clinical significance of the topic, students need to be trained in this area and possess the necessary skills. Although the NMC has rolled out a new competency-based curriculum for medical undergraduates, it does not explicitly contain a competency on cognitive assessment. However, it does include an MMSE; notably, MMSE has low sensitivity (30%–60%) in the assessment of cognitive dysfunction when a cutoff score of 19–23 is used for cognition dysfunction. 26 Also, it does not consider visuospatial and frontal executive functions. 14 In general practice, therefore, using the MoCA as a screening tool provides quick guidance for referral and further investigation of MCI. 27 In a meta-analysis assessing MCI detection among individuals aged over 60 years, the MoCA exhibited superior sensitivity (80.48%) and specificity (81.19%) than the MMSE with a cutoff of 27/28, which showed lower sensitivity (66.34%) and specificity (72.94%). 28 A curriculum for dementia assessment has been previously outlined, and students were subjected to multidisciplinary training for assessing dementia, cognitive decline, caregiver burden, behavioral issues, and impact. They included training on the Modified Mini-Mental State Examination (3MS), MoCA, and Saint Louis University Mental Status Examination (SLUMS). 29 It has been agreed that MMSE could be more responsive to cognitive changes over one year that impact functional capabilities than SLUMS. 30 Agreeably, in our toolkit, we have explored the training needs on the MoCA and any tool for mental status examinations (3MS, MMSE, or SLUMS).
Our toolkit is unique because it does not explore the training needs for cognition under the umbrella of dementia training. Instead, it has a targeted focus on cognitive impairment training. Before developing the curriculum and assessments, we conducted a TNA to guide evidence-based educational intervention development. The toolkit was developed after careful consideration of the training needs of medical students, considering the differences in the year of training while retaining the standards of training from expert literature. The final toolkit was developed iteratively by reaching a consensus, with the involvement of psychiatrists, family medicine, and public health experts. Notably, our toolkit upholds the role of a primary care physician, that is, screening, diagnosis, care planning, and referral, and it will promote task force development at the primary level. 31
Final-year students have consistently demonstrated the highest emphasis on the importance of clinical tasks involving cognition (mean score of 36.38 ± 5.95). This indicates that, as they complete their medical education, they recognize the significance of assessing cognitive functions and managing cognitive dysfunctions in clinical practice. The research investigated medical students’ attitudes toward people with dementia, revealing generally positive attitudes across different years and locations, with year 3 and year 5 students showing more positive attitudes than year 1 students. 32 Another national survey investigated final-year medical students’ attitudes and perceived competence regarding end-of-life care for individuals with dementia. While positive attitudes were noted, challenges in specific clinical tasks were identified, indicating potential benefits from additional basic training. 33 However, a Croatian study on final-year medical students found neutral attitudes toward working with persons with dementia and poor theoretical knowledge of dementia. Results highlight the need to enhance education on dementia to ensure that future healthcare professionals can provide optimal care for persons with dementia. 34
Second-year students have shown notable competence in the performance of clinical tasks, as reflected in their mean score of 28.55 ± 8.95. This might be due to the false estimation of one’s abilities as they are just introduced to clinics due to their lack of awareness of the subject matter, including complexities in assessing and managing cognitive dec. Pre–final-year students stand out with higher training needs (9.71 ± 8.61). This observation implies that this stage could best target the discussed training. The item-specific post-hoc analysis reveals similar findings. Pre–final-year students have significantly higher training needs than second-year students and require significant attention in all areas, including accessing literature, planning and organizing care for patients with cognitive impairment, performing MSE, explaining/counseling interventions to patients with cognitive defects, and screening for cognitive deficits. In a pilot study from Florida State University, fourth-year medical students’ charting of older persons’ cognition and functional status during non-geriatric clerkships showed higher documentation than reported in the literature, potentially due to geriatrics integration in the four-year curriculum, which is not adopted in India. 35 In another study from Nepal, it was observed that medical students, in general, had an average level of knowledge about dementia, whereas students being exposed to Continuing Medical Education (CMEs) and classes performed better. 36 The difference observed between the second-year and pre–final-year students indicates the potential for enhancing awareness of cognitive dysfunctions through early exposure to clinical rotations in psychiatry or physical medicine and rehabilitation, starting as early as the second year. This can be achieved through simulated teaching–learning methodologies, including tutorials and small group discussions (SGDs), and novel approaches like movie clubs, which are crucial for effectively instructing students in this domain.
Significant differences in the training gap between different years of medical school education suggest that certain competencies are taught in medical school, and the training gap changes over the years, whereas other non-significant competencies may indicate that the training gap is not influenced by years in medical school and, thus, needs separate addition to the curricula. Initially, the contrast between the importance and performance scores of students in Figure 1 from the TNA suggests that specific interventions may not be necessary. However, the notable difference between the importance and performance of each item highlights a training need. It is crucial to recognize that this plot could lead to misleading conclusions due to the disparity in rating scales—performances were rated as 4s. In contrast, importance was rated on scales of 6 and 7. Despite both plots appearing in the upper-left corner, there is still a discernible gap. This is further substantiated when examining the training score versus the organizational score; both scores are elevated, indicating a requirement for a dual approach.
Final-year students emphasize training, as their training scores are slightly higher (35.13 ± 6.98) than interns (34.55 ± 6.08). This could indicate that even though neurological and psychiatric curricula cover cognition in pre-final and final years, the students in the final year and internship still perceive a lack of knowledge and necessary skills in performing these tasks. This finding underscores that such competencies should have a level of “show how” or “perform” independently as per Miller’s pyramid and should be taught through demonstration in SGDs or bedside teaching. A similar trend is reflected in the need for an organizational score for final years (35 ± 5.57) and interns (34.05 ± 6.85). Therefore, incorporating cognitive assessment as a mandatory component of formative assessment through an objective structured clinical examination during final-year ward leaving exams and internship completion is recommended.
Study Limitations
The current study’s limitations include a modest response rate of 25.5%, with lower rates among first- and final-year students, possibly due to exam stress and the timing of the study just before the summer vacation. The lack of incentives, reliance on self-reported surveys, and potential biases from students’ motivations and experiences may also affect results. This pilot study, based at a single center in India, also faced limitations due to limited demographic data, thereby limiting the generalizability of the findings.
Conclusion
In conclusion, a learning intervention that incorporates “screening,” “assessment,” and “referral of patients with cognitive decline” is required for medical students. Exposing students as early as the second year could improve awareness. A targeted curriculum must be outlined for the pre–final-year (third-year) students, while final-year students and interns should be exposed to assessments. For students beyond a pre-final year, special training modules such as CMEs, guest lectures, and clinical demonstrations, including simulation-based training, can be made to cover the training gap if not trained initially. Students can also be informed of free MoCA training and certification at
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
We acknowledge the training support from the Psychiatric Research Infrastructure for Intervention and Implementation in India (PRIIIA). Led by the principal investigators Dr. Vishwajit Laxmikant Nimgaonkar (University of Pittsburgh), Dr. Smita N. Deshpande, and Dr. Mary Elizabeth Hawk, PRIIIA focuses on India to address mental and neurological health challenges from 2014 to 2024. This project, in partnership with the Fogarty International Center and aligned with the goals of NIMH and NINDS, aims to improve mental disorder treatments. Special thanks to Dr. Triptish Bhatia for her invaluable support in research training coordination. Mission of PRIIIa includes improving cognitive research training, engaging recent graduates, fostering implementation research, establishing training hubs, and influencing psychiatric healthcare policies, with a particular emphasis on understanding cognitive dysfunction in psychiatric diseases (
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
The authors assumes full responsibility for the entire content of the manuscript. No parts of this manuscript were generated by any AI tool.
Ethical Approval
The study received the approval of the Institute Ethics Committee (IHEC No. IHEC/2023/LOP/IL0108). Written informed consent from all the participants was obtained before their involvement in the research work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received the training support from the Psychiatric Research Infrastructure for Intervention and Implementation in India (PRIIIA), which was funded by the NIH under Grant D43TW009114 (
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.