
Abstract
Background:
Very few Indian studies have explored disability among patients with somatoform disorder and the burden experienced by their caregivers. We aimed to assess the levels of disability among patients with somatoform disorder and the levels of burden among their caregivers and compare these parameters against patients with schizophrenia.
Methods:
Participants included adults with a diagnosis of somatoform disorders (F45.0–F 45.9) (n = 28) or schizophrenia (F20.0–F20.9) (n = 28) diagnosed as per the International Classification of Diseases, Tenth Revision (ICD-10), clinical descriptions, and diagnostic guidelines, as well as their caregivers. The WHO Disability Assessment Schedule 2.0 and Family Burden Interview Schedule were used to assess patient disability and caregiver burden, respectively. Independent Student’s t-test or chi-square test was used to compare relevant sociodemographic and clinical parameters.
Results:
Out of 56 patients, the mean (±SD) age of the sample was 38.6 (±10.5) years. Females constituted a slender majority of the sample (n = 29, 51.8%). The mean disability score of patients with somatoform disorders was slightly higher (83.6 ±20.9) than that of patients with schizophrenia (82.3 ±16.7). Similarly, the mean burden score of caregivers of patients with somatoform disorders was nominally higher (18.96 ±9.9) than that of caregivers of patients with schizophrenia (15.7 ±9.7). Neither of these differences approached statistical significance (P > 0.05).
Conclusion:
Patients with somatoform disorders experience considerable levels of disability, and their caregivers go through various levels of burden in their daily life that is comparable to schizophrenia.
Patients with somatoform disorder suffer from a considerable degree of disability that is comparable to severe mental illness like schizophrenia. Caregivers of patients with somatoform disorder experience a considerable burden that is also comparable with schizophrenia.Key Messages:
Schizophrenia is a severe chronic mental disorder with a relapsing course that is associated with disability and functional decline. 3 Furthermore, the functional decline can lead to disability in several aspects of an individual’s personal life, job, and socialization, and there are major deficits in employability, marriage, and taking care of their children. 4 In most societies, family members play a pivotal role in taking care of mentally ill individuals. Chronic mental illness imposes significant burdens on caregivers on various aspects while caring for the patient. Burden strains the physical, psychological, social, spiritual, and emotional components of the caregiver. According to Treudley, “burden on the family” refers to the consequences for those in close contact with a severely disturbed psychiatric patient. Objective burden concerns not only the patient’s symptoms, behavior, and sociodemographic characteristics but also the changes in household routine, family or social relations, work, leisure time, and physical health. The subjective burden refers to the caregiver’s attitude or emotional reactions while taking care of patients and subjective distress among family members. 5 Hence, it is essential to explore burdens faced by caregivers of patients with chronic mental illness to gain insight into their problems and to improve the treatment outcome.
Many researchers have investigated the consequences and problems that are faced by the caregivers of patients with schizophrenia.6–8 But, there is a paucity of data regarding the problems faced by the caregivers of patients with somatoform disorder. A prior Indian study had found that patients with somatization disorder suffer substantial disability and caregiver burden, comparable with severe mental illness. 9 As these findings were rather counterintuitive and contrary to extant literature10–13 and given the paucity of such studies from the Indian setting, this study was undertaken to investigate the level of disability of patients with somatoform disorders and the level of the burden in their caregivers, and the results were compared with patients with schizophrenia and their caregivers.
Moreover, disability associated with somatization has been investigated by few researchers.14–17
Materials and Methods
A cross-sectional, comparative study was carried out among adults with a diagnosis of somatoform disorders (F45.0–F 45.9) (n = 28) or schizophrenia (F20.0–F20.9) (n = 28) as per the International Classification of Diseases, Tenth Revision (ICD-10), clinical descriptions, and diagnostic guidelines, as well as their caregivers. Patients with a diagnosis of somatization disorder, pain disorder or undifferentiated somatoform disorder were included under somatoform disorder. Participants were recruited from the Department of Psychiatry, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pudhucherry, India, using the purposive sampling technique, in the period between August 2018 and December 2018. The department runs a separate exclusive weekly special clinic for newly diagnosed patients with somatoform disorder as well as for schizophrenia.
With an expected difference in means of 9.60 on World Health Organization Disability Assessment Schedule (WHODAS) disability scores (SD1 12.50 and SD2 12.82) between the two groups and keeping power at 80% and two-sided confidence interval at 5%, the sample size was calculated as 28 in each group.
A caregiver, in this study, refers to a family member or a close relative (unpaid) who had been regularly staying with the patient for more than six months and played a major role in his/her daily activities, health care, and socialization. Patients who were diagnosed to have either somatoform disorder or schizophrenia, aged 18 years and above, of both genders, as well as their caregivers with similar criteria, were included as study participants. Caregivers who were known to have any psychiatric illness were excluded.
Ethical approval was obtained from the Institute Ethical Committee. Family Burden Interview Scale (FBIS) by Pai and Kapur was used to assess the level of the burden faced by the caregivers. The tool consists of 24 items that are grouped into six domains: financial burden, disruption of routine family activities, disruption of family leisure, disruption of family interaction, effects on the physical health of others, and effects on the mental health of others. Each item is rated on a three-point scale (0 = No burden, 1 = Moderate burden, 2 = Severe burden). Based on the interpretation of the scores, the participant’s level of burden was assessed (Mild: 1–16: Moderate: 17–32; Severe: 33–48). 18 This scale has been used in many research studies conducted in the Indian set-up and is suitable according to the socioeconomic and the cultural conditions prevailing in India. Inter-rater reliability and coefficient were calculated to be 0.9 and 0.8, respectively, and it is valid and reliable for both clinical and research purposes. 18
The adult self-administered version of WHODAS (2.0) was used to assess disability. It has 36-items that include six domains: understanding and communication, getting around, self-care, getting along with people, life activities-household/school/work, and participation in society. Each item is rated on a five-point scale (1 = No disability, 2 = Mild, 3 = Moderate, 4 = Severe, and 5 = Extreme or cannot do). It is well validated, and the Cronbach’s alpha reliability score ranged from 0.75 to 0.94 for domains and 0.93 for the total score. 19 In addition, WHODAS 2.0 has good psychometric qualities, including good reliability and item-response characteristics, and its robust factor structure remains the same across cultures and in different patient populations. Further, it shows concurrent validity when compared with other measures of disability or health status or with clinician ratings.20–23
Besides, the Clinical Global Impression Scale was used to assess the severity of illness. Severity is rated on a seven-point scale, and the range of responses varies from 1 to 7 (1 = Normal, 2 = Borderline mentally ill, 3 = Mildly ill, 4 = Moderately ill, 5 = Markedly ill, 6 = Severely ill, 7 = Amongst the most severely ill patients). The intra class-correlation coefficients were about 0.9. 24
The tools were translated from English into the local language (Tamil) by following the World Health Organization (WHO) scale translation protocol. 25 The rater underwent initial training under the faculty in Psychiatry Department to use these measures.
Statistical Analysis
Continuous variables were expressed as mean with standard deviation and discrete variables as frequencies with percentages. A comparison of variables between groups was done using the chi-square test for discrete variables and Student’s t-test for continuous variables. For comparison of demographic factors between groups, and for comparison of clinical factors, a P-value of <0.05 was considered as significant.
Results
Out of 56 patients, 29 (51.8%) subjects were female. The majority of the subjects (n = 35, 62.5%) were married. The mean±standard deviation age of the patients in the somatoform disorder group was 39.45±11.26, and that of the schizophrenia group was 37.68±9.89. Most of the subjects (n = 34, 6.7%), were unemployed; 51 (91.1%) of the subjects hailed from the rural area.
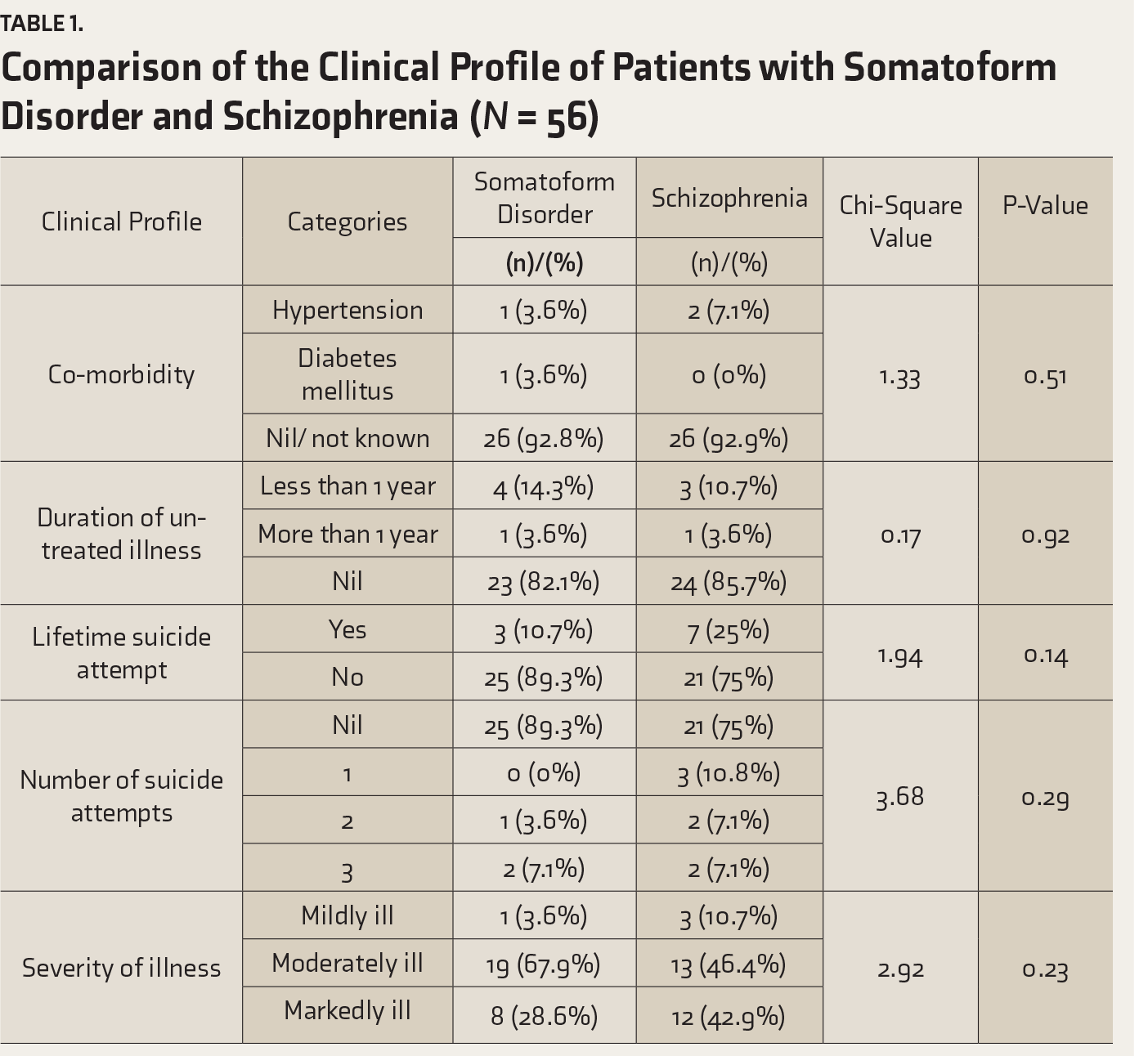
Illness characteristics such as age at onset, duration of illness, duration of treatment, comorbidity, duration of untreated illness, and the presence of lifetime suicide attempts were also assessed. This indicated that 52 (91.8%) subjects did not have any comorbidity; 3 (5.4%) had hypertension, and 1 (1.8%) had diabetes mellitus. A total of 47 (83.9%) subjects were taking treatment continuously. The majority of the subjects (somatoform disorders: n = 25, 89.3% and in schizophrenia: n = 21, 75%) did not have any suicide attempt in the past. The severity of illness as assessed by the Clinical Global Impression Scale indicated that 4 (7.1%) patients had a mild illness, 32 (57.1%) had a moderate illness, and 20 (35.8%) were markedly ill.
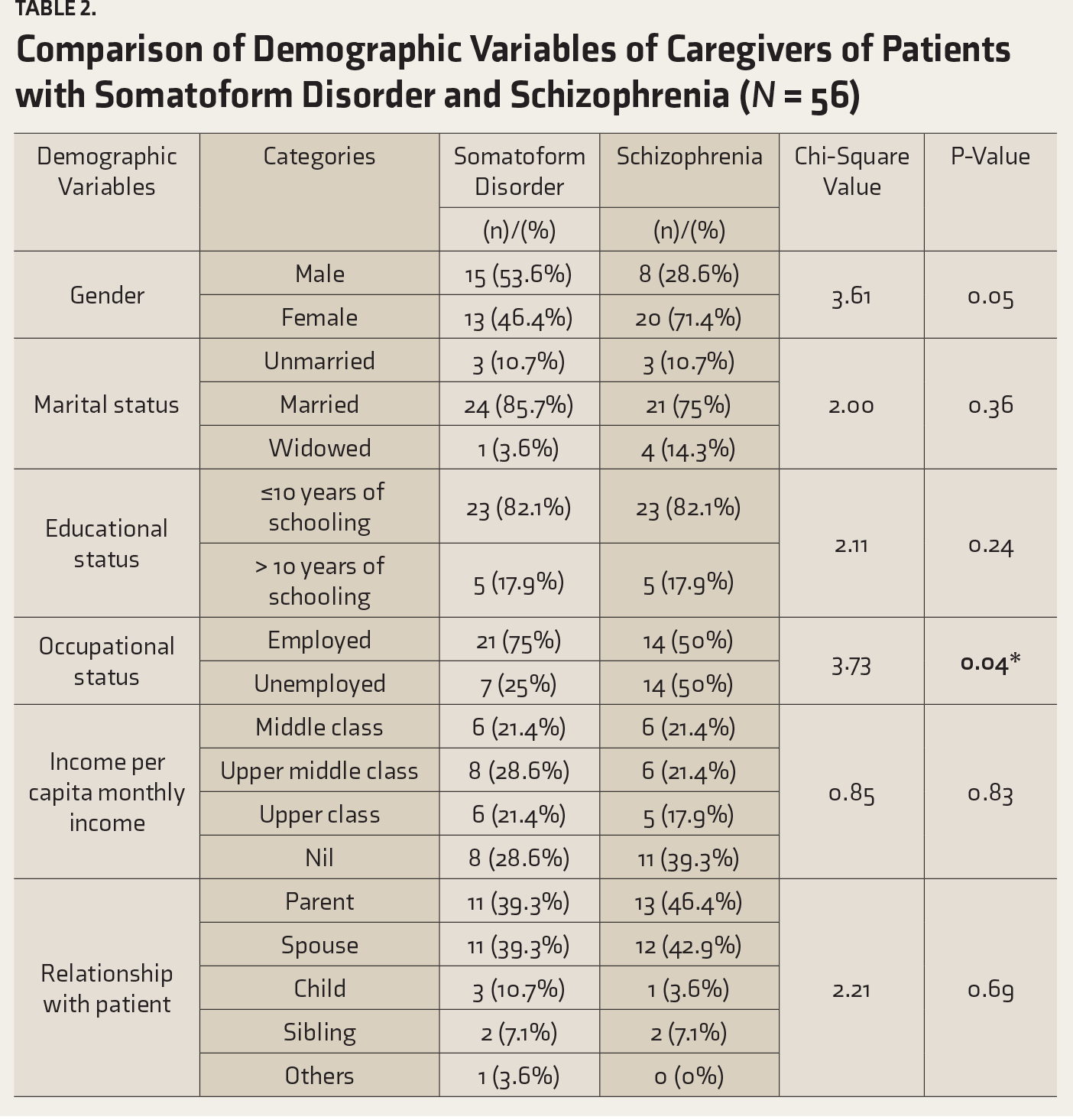
The analysis of demographic variables of caregivers showed that the mean age, in years, of the caregivers of patients in the somatoform disorder group was 45.54±15.56 and that of schizophrenia group was 51.46±12.79; 33 (58.9%) were females and 23 (41.1%) were males; 45 (80.4%) were married; 46 (82.1%) had finished schooling up to 10 years; most 35 (62.5%) were employed; 19 (33.9%) had no income. The majority of the caregivers were parents (n = 24, 42.9%) and spouses (n = 23, 41.1%). Children and siblings as caregivers were less in number (n = 5, 8.9%) and 4 (7.1%), respectively.
The comparison of demographic variables of patients with somatoform disorder and schizophrenia by using chi-square analysis revealed that females outnumbered males among patients with somatoform disorders; whereas, male patients outnumbered females in schizophrenia. In the somatoform disorder group, 22 (78.6%) were married, and in the schizophrenia group, 13 (46.4%) were married; it was also statistically significant (P = 0.03). A total of 14 (50%) patients with the somatoform disorder had no income, whereas the number was 18 (64.3%) among patients with schizophrenia; it was also statistically significant (P = 0.04).
The comparison of the clinical profile of patients with somatoform disorder and schizophrenia is summarized in
Comparison of the Clinical Profile of Patients with Somatoform Disorder and Schizophrenia (N = 56)
Comparison of Demographic Variables of Caregivers of Patients with Somatoform Disorder and Schizophrenia (N = 56)
Assessment of different levels of disability among patients with somatoform disorder and schizophrenia, using WHODAS, revealed that 20 (71.4%) patients with somatoform disorder and 19 (67.8%) patients with schizophrenia had a moderate disability (n = 6, 21.4%) patients with somatoform disorder and 7 (25%) patients with schizophrenia had a mild disability, and 2 (7.2%) patients with either disorder had a severe level of disability.
Assessment of various levels of family burden among patients with somatoform disorder and schizophrenia, using FBIS, demonstrated that the mean value of the level of burden among caregivers of patients with the somatoform disorder was more (18.96+9.93) when compared to the burden among caregivers of patients with schizophrenia (15.71+9.67).
The comparison between the level of disability and caregivers’ burden indicated that the mean value of the level of disability in patients with somatoform disorder was slightly higher (83.57±20.91) than in those with schizophrenia (82.32±16.65), but the difference was not statistically significant. Similarly, the mean score of level of burden among caregivers of SD was more (18.96±9.93) when compared to schizophrenia (15.71±9.67) and it also did not approach statistical significance.
The mean value of age at onset of illness was 33.04±9.86 in the somatoform disorder group, and for the schizophrenia group, it was 33.04±10.51. The mean value of the duration of illness was more 71.07±82.59 (months) in somatoform disorder than schizophrenia (61.07±70.04).
The domain-wise comparison between the level of disability of patients with somatoform disorder and schizophrenia showed that the mean level of disability of patients in understanding and communicating domain was slightly more in the schizophrenia group (15.32±3.58) than the somatoform disorder group (14.46±5.13). In the participation in the society domain, patients with somatoform disorder had more disability (22.17±5.65) than those with schizophrenia (20.0±4.39). The results of burden analysis based on FBIS, revealed that in the financial domain, caregivers of the somatoform disorder group had a higher score (5.07±2.22) than those with schizophrenia (4.85±2.69). The mean values of the burden score in disruption of the family interaction domain showed that caregivers of patients with somatoform disorder had more burden (4.07±2.95) than the schizophrenia caregivers (2.85±2.20) and it was statistically significant (P = 0.008). Likewise, in the domain of the effect on the physical health of others, more burden was observed in somatoform disorder (1.50±1.13) than schizophrenia (0.928±1.01), and it was also statistically significant (P = 0.004).
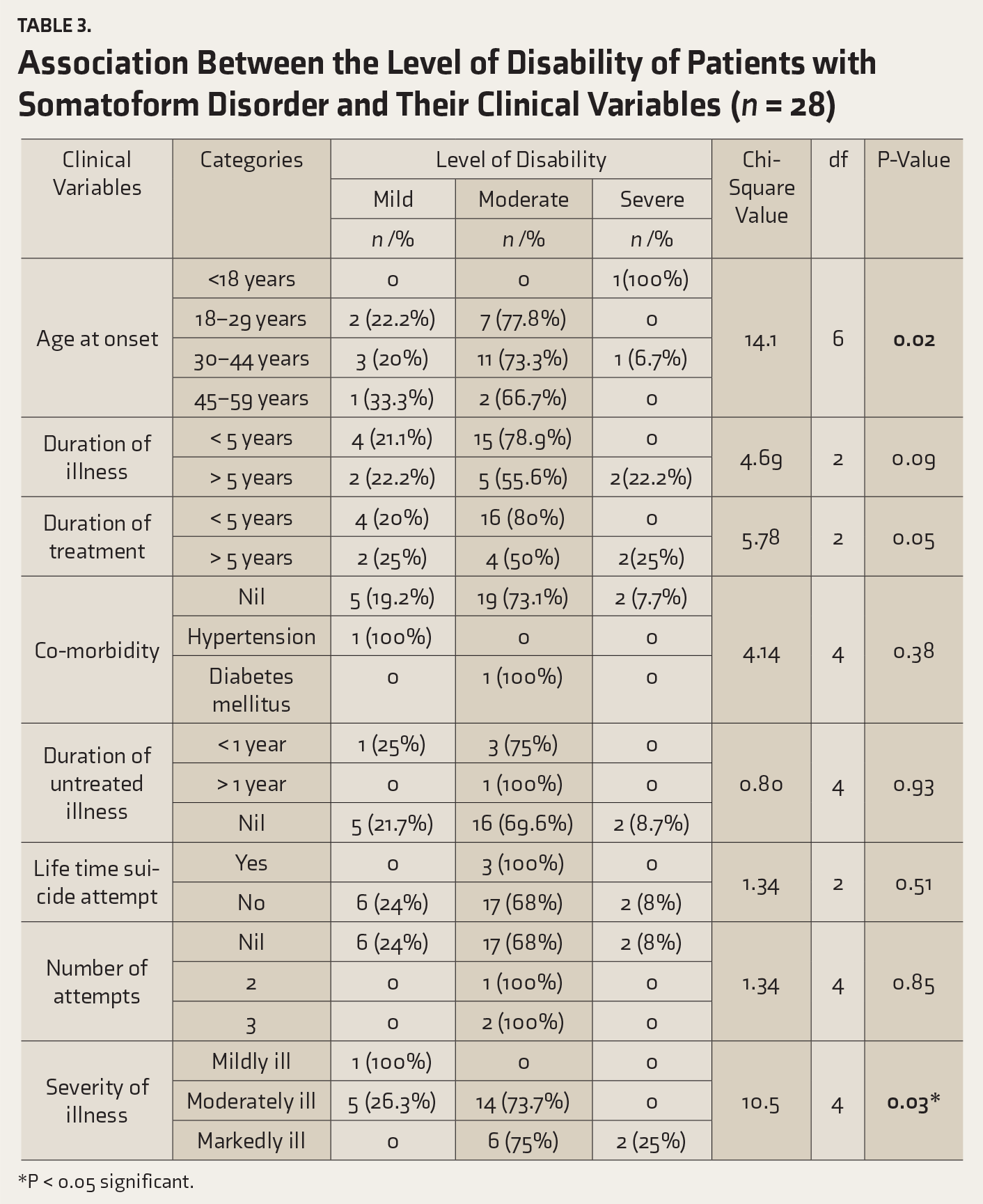
There was no significant association between the levels of disability of patients with either disorder with their demographic variables. In contrast, a significant association was found between the level of disability among patients with a somatoform disorder with their clinical variables such as age at onset, duration of treatment, and severity of illness (
Association Between the Level of Disability of Patients with Somatoform Disorder and Their Clinical Variables (n = 28)
*P < 0.05 significant.
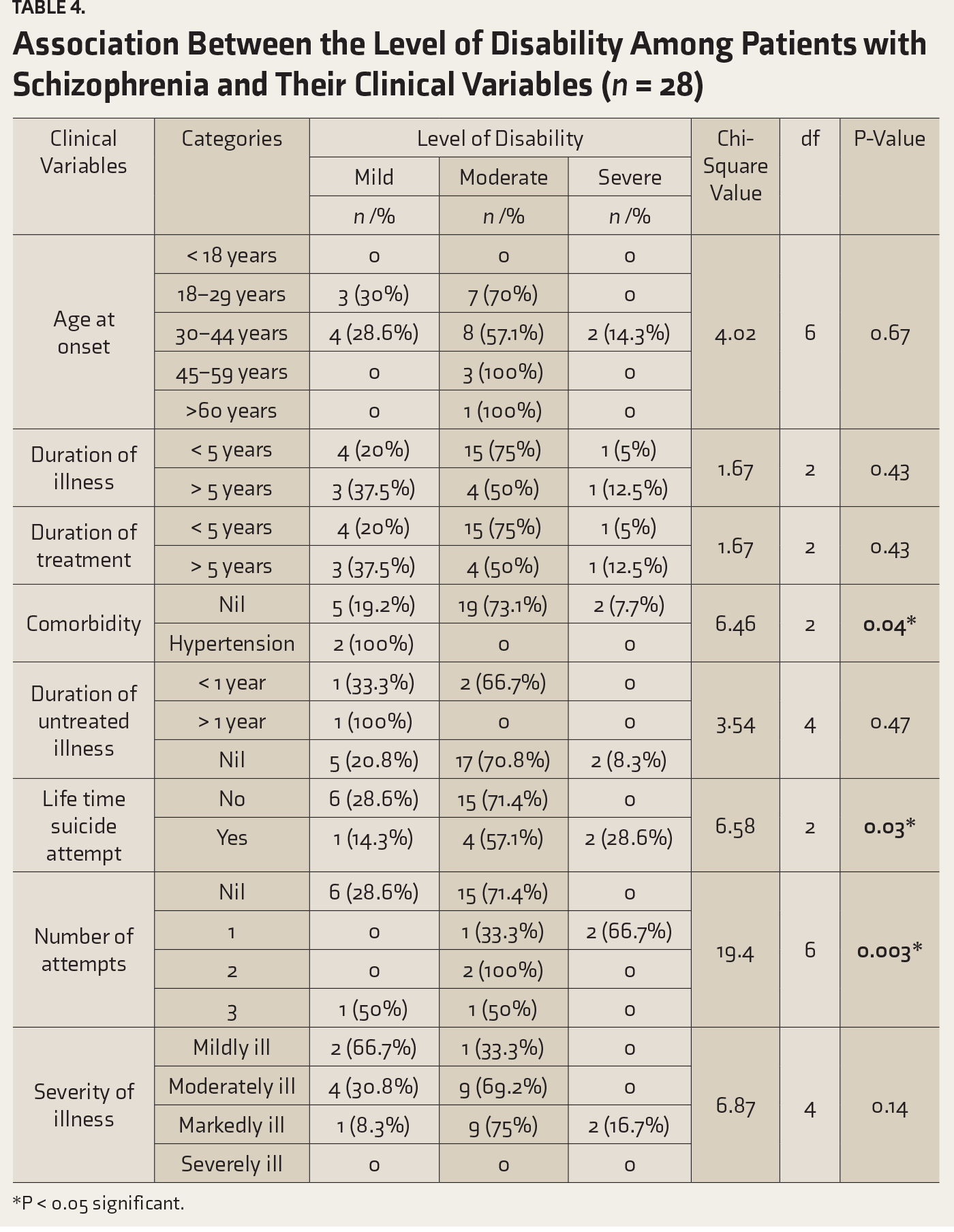
Association Between the Level of Disability Among Patients with Schizophrenia and Their Clinical Variables (n = 28)
*P < 0.05 significant.
The association between the levels of burden with demographic variables among caregivers of patients with schizophrenia is illustrated in
Association Between the Level of Burden Among Caregivers of Patients with Schizophrenia and Their Demographic Variables (n = 28)
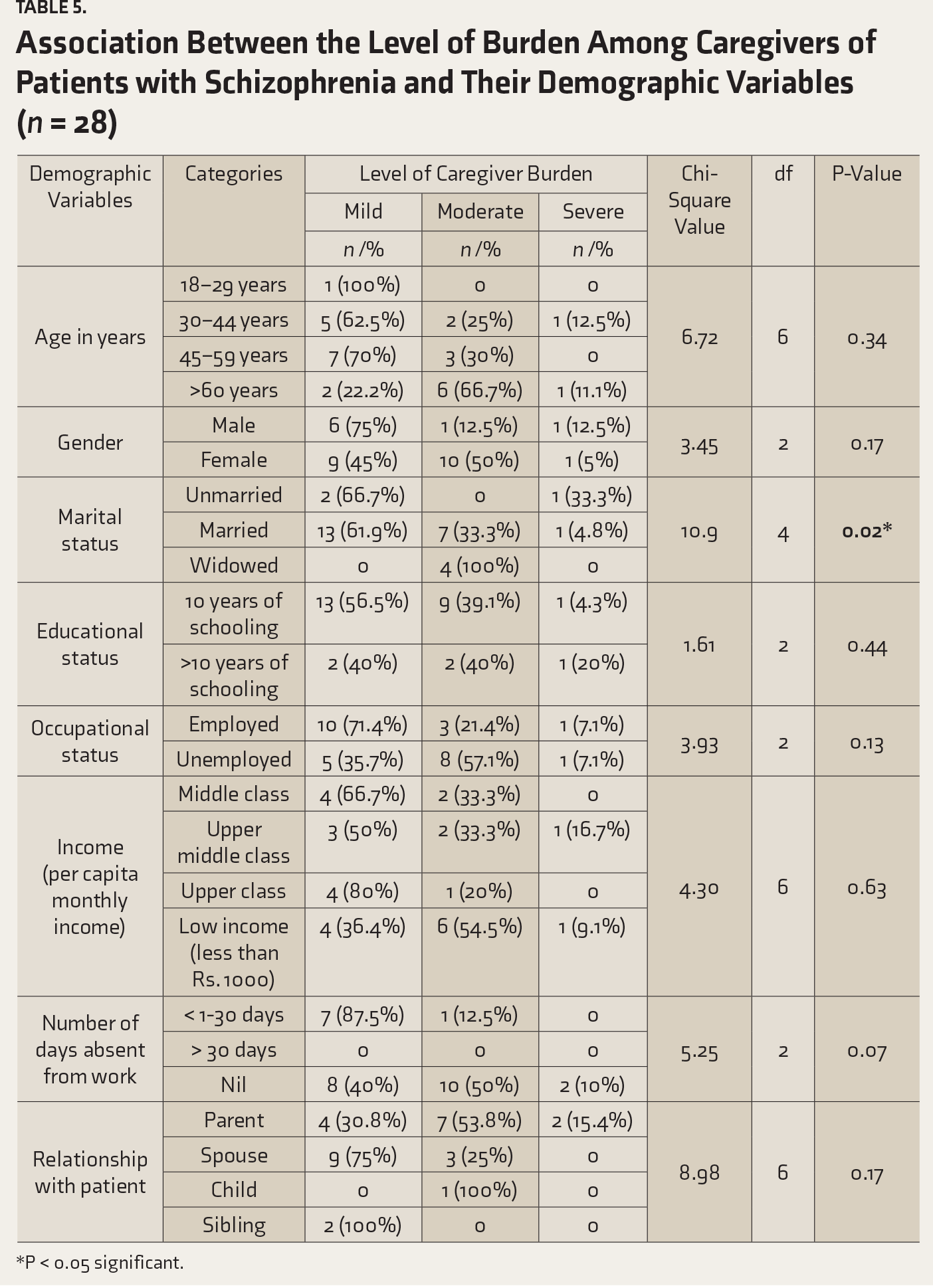
*P < 0.05 significant.
Association Between the Level of Burden Among Caregivers of Patients with Somatoform Disorder and Their Demographic Variables (n = 28)
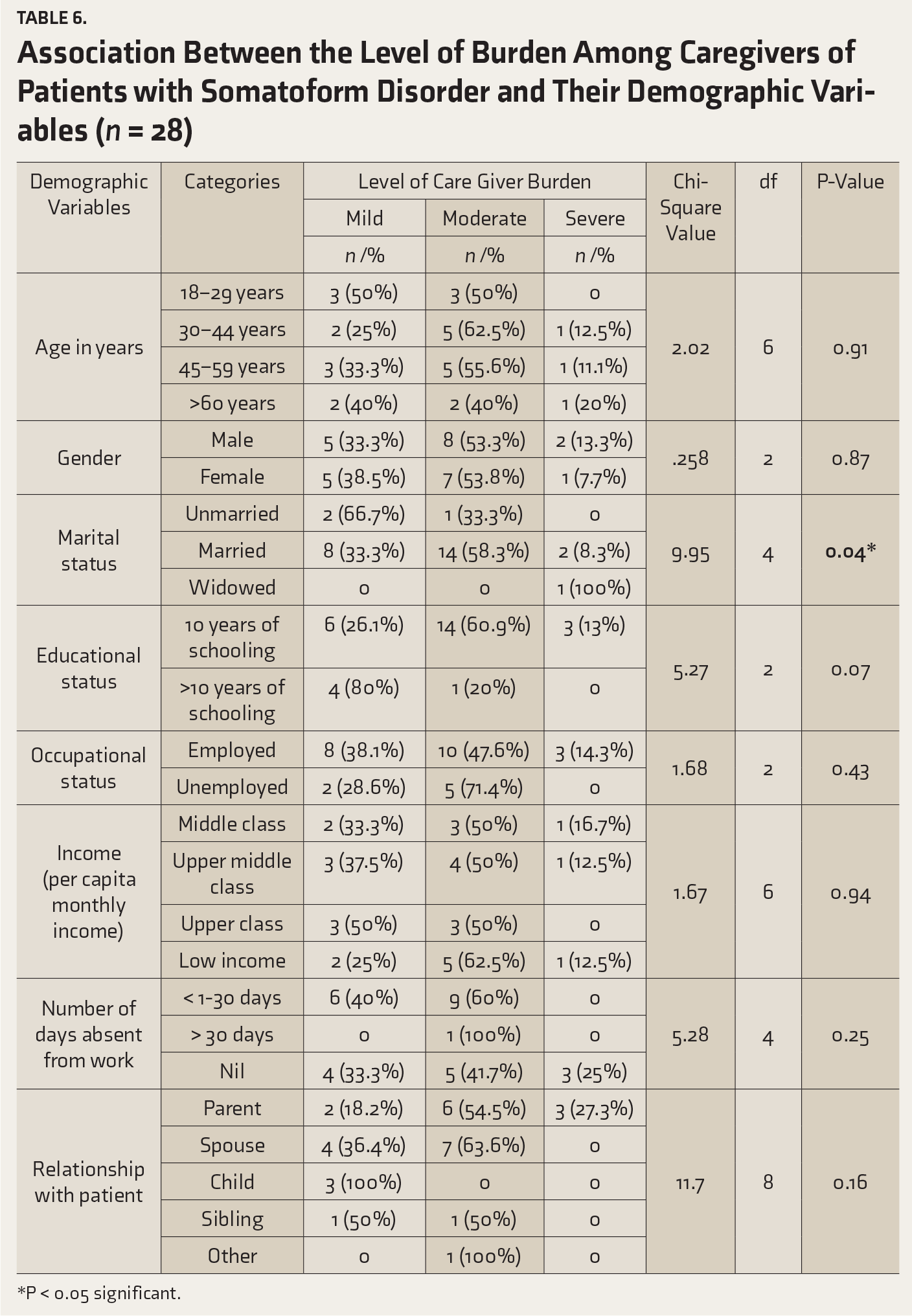
*P < 0.05 significant.
Further, the nine-items patient health questionnaire (PHQ-9) was used to measure the level of depression among patients with somatoform disorder and schizophrenia. Exploratory analysis revealed that in somatoform disorder, majority of the patients had a mild level 10 (35.7%), 8 (28.6%) had a moderately severe level, 6 (21.4%) had a moderate level, 3 (10.7%) had a minimal level, and 1 (3.6%) had a severe level. The mean level of depression was 10.75±5.56. Comparably, in schizophrenia, depression was at moderate level in 11 (39.3%) subjects, 7(25%) had a mild level, 4 (14.3%) had a minimal level, 3 (10.7%) had moderately severe level, and fewer patients had severe level (n = 3, 10.7%). The mean level of depression was 10.89±5.91.
Discussion
Worldwide, mental disorders are one of the prime causes of morbidity and disability. As per the global heath report 2001, mental illness accounted for 25% of the total disability and 16% of the total burden. A family member who has been living with the patient constitutes a major support system in meeting the patient’s daily needs and continuing care in the community. The emotional impact of caring can trigger a range of emotional reactions such as fear, sadness, anger, guilt, stigma, and rejection among caregivers. 26
We aimed to assess the caregiver burden and disability of patients with somatoform disorder or schizophrenia. We found that levels of disability and caregiver burden were comparable between somatoform disorders and schizophrenia.
Even though more number of patients with somatoform disorder (n = 20, 71.4%) or schizophrenia (n = 19, 67.8%) had moderate disability, results highlighted that the percentage of patients was slightly high in somatoform disorders. The domain-wise analysis demonstrated that patients with somatoform disorder scored higher disability in the participation in the society domain. Patients with somatoform disorder had a smaller score in the “understanding and communicating” domain as compared to schizophrenia. Another study 27 had revealed that patients with schizophrenia scored higher disability in domains such as “understanding and communicating” and “getting along with people.” Krishnan et al. 9 had found that patients with somatoform disorder scored higher on total disability and on the domains “getting around” and “participation in society” as compared to schizophrenia. The differences could be due to the nature of illness. In schizophrenia, patients often have cognitive deficits and lack of communication skills. In contrast, patients with SD have somatic complaints like not being able to stand for long periods and not being able to walk a long distance.
The comparison of levels of burden among caregivers indicated that caregivers of patients with somatoform disorder had a moderate burden, and caregivers of patients with schizophrenia had a mild burden. Caregivers of patients with somatoform disorder had a higher level of burden in the FBIS domains financial burden, disruption of family interaction, and effects on the physical health of others. This might be due to the maintenance of the remission period by patients with schizophrenia, leading to better functioning and less disability, causing lesser burden. In contrast, another study 28 reported that caregivers of patients with schizophrenia had a higher level of burden in the mentioned FBIS domains and the overall family burden. A couple of studies found that in schizophrenia, the financial burden was the most common burden among the six domains.29, 30 Disruption of family activities has also been reported to be more in schizophrenia. 31
Krishnan et al. 9 reported that marital status had a significant association with the level of caregiver burden of patients with either of the disorders. This study also revealed the same. Even though it was not statistically significant, the results of the current study indicated that female caregivers experienced more burden than males. Other studies reported a similar finding. 32 Prior authors have shown that the level of psychosocial disabilities in patients suffering from somatoform disorders were similar to those seen in other mental disorders such as depression, anxiety disorders, and affective disorders. 33
It is possible that since the study setting was a tertiary care cum teaching hospital and because the mean duration of illness was longer in patients with somatoform disorder when compared to schizophrenia, there may have been an over-representation of severely ill SD patients in the sample. These may explain the comparable levels of disability between schizophrenia and somatoform disorders in our study.
Further, Clinical Global Impression—Severity scale ratings for the somatoform disorder were comparable to schizophrenia. This finding is counterintuitive and may be explained by a few reasons: first, the study setting was a tertiary healthcare center, and therefore, the patients selected might have been more severely ill at baseline. That the mean duration of illness was higher for somatoform disorders than schizophrenia in our sample may support this assertion. Second, the presence of comorbid depression, seen in many patients, may have contributed to the increased ratings of severity of illness by the clinicians.
The mean age of onset of schizophrenia was higher than reported in the literature. In the absence of a structured instrument to assess age at onset, possible reasons for this finding may include the report of proxies for age at the onset by caregivers, such as the age at first hospitalization or the age at first contact with healthcare professionals, both of which have been referred to in the literature. A couple of studies have reported the age of onset as “the age at which first clear psychotic symptoms were observed.”34, 35 The age at first hospitalization for psychiatric illness has been considered as the age at onset in many other studies.36–38 The age at first contact with psychiatric service has also been reported as age at the onset by other researchers.39, 40
Based on the results of this study, it can be inferred that patients with somatoform disorders experience considerable disability and their caregivers, too, experience levels of burden comparable with severe mental illness such as schizophrenia. Hence, the difficulties faced by these individuals need to be addressed effectively to improve the treatment outcome, along with other strategies.
Limitations
The study was carried out in a tertiary care cum teaching hospital, and the results may not be generalized to other centers. Due to the study setting, it is possible that more severely ill patients may have got selected. The study employed convenience sampling. Both disability and burden were assessed through self-report measures, and this may limit their accuracy. Since it was an exploratory study, some of the associations could be chance findings. Therefore, these findings may be considered as preliminary and tested in confirmatory studies.
Conclusion
The disability caused by somatoform disorders is comparable with schizophrenia, and the burden experienced by the caregivers is also comparable. Further investigations are needed to explore the difficulties faced by these individuals to plan and implement effective treatment strategies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.