
Abstract
Background:
Understanding the caregivers’ experiences of aggressive persons with mental disorders is very important from the public health point of view. Only a few Indian studies have focused on this. No Indian studies could be found that explored the caregivers’ experiences of aggressive persons with schizophrenia. This study was conducted to explore the same.
Methods:
A qualitative phenomenological study was conducted in the outpatient and inpatient settings at a tertiary care mental health institute at Bengaluru, Karnataka. Ten participants meeting the eligibility criteria were selected using purposive sampling. Data collection was done by individual, in-depth, face-to-face, semi-structured interviews using topic guide along with subjective observation and field notes. Each interview was audio-recorded, transcribed, translated, and coded. A total of five master themes and 22 subthemes were derived from the codes by using the qualitative research software ATLAS-Ti.
Results:
The themes derived based on the experiences of caregivers living with their aggressive persons with schizophrenia were the aggressive behaviors of the patients, reasons for the aggression of the patients, dealing with the aggression of the patients, the impact of aggression on the caregivers, and the coping methods of the caregivers.
Conclusion:
This study explored the experiences of the caregivers living with the aggressive patients. The results show the need for care and support to the caregivers. The themes can guide mental health professionals while developing culture-specific tools and interventions for future research as well as suggest them standard operating procedures for prevention and management of aggressive patients in the psychiatric hospitals.
Caregivers of aggressive persons with schizophrenia experience negative impact because of the different types of aggression from the patients. The reasons for the aggression vary from patient to patient. The caregivers adopted different coping strategies to deal with their patients’ aggression.Key Messages:
The World Health Organization estimates that 40%–90% of persons with schizophrenia live with their relatives. 2 Even though caring for a person with schizophrenia may be a positive experience for some, it is also frequently associated with a negative impact on the caregivers’ life. 4
In addition to the positive symptoms associated with schizophrenia, patients also present with other associated symptoms such as aggression, agitation, and anxiety. 5 According to a study, verbal aggression and violence were the behaviors that caused most difficulty to the caregivers. 6 Even though aggression among persons with schizophrenia is a major problem faced by the caregivers, limited qualitative studies have been done to explore the experiences of caregivers of aggressive patients with schizophrenia. A large majority of these studies were conducted in Western countries. 6 – 17 It is difficult to generalize the results to caregivers in India because of cultural differences. Therefore, this study was undertaken to describe the caregivers’ experiences of aggression by their family member with schizophrenia. This study would provide a more holistic and rich description of the phenomenon of caring for the aggressive persons with schizophrenia. The results could provide insights to mental health professionals while developing need-based interventions to empower family caregivers in handling aggression in persons with mental illness.
Materials and Methods
This phenomenological study was conducted at a tertiary care mental health institute at Bengaluru from April 2017 to April 2018. The study was approved by the ethics committee of the institution.
Ten participants were selected from psychiatric wards (n = 5) and the outpatient department (n = 5) using purposive sampling technique. Primary caregivers, both male and female above 18 years of age, living with the patients with schizophrenia for the past six months, who had experienced aggressive behavior during the last one year were selected. Caregivers other than family members of persons with schizophrenia and caregivers suffering from any kind of sensory deficits or mental illness were excluded. The adequacy of the sample size was evaluated by the quality and completeness of information provided by the participants. Data collection continued till saturation occurred.
The caregivers who signed the informed consent were enrolled and then sociodemographic information was collected using a brief participant profile prepared by the researcher. A semi-structured interview using a topic guide, which was prepared by the researcher and validated by five experts, was done with each individual. The topic guide included the following questions:
What could be the reasons for the aggressive behavior of your patient?
How do you feel when your patient becomes aggressive?
How did you react when your patient became aggressive?
What do you do to reduce the aggressive behavior of your patient?
How do you manage the feelings evoked by the aggressive behavior of your patient?
What are the changes you experienced in your life due to the aggressive behavior of your patient?
Each participant was interviewed for approximately 30–45 minutes in one session. Interviews were audiotaped and field notes were written by the researcher to complement the audiotaped interviews. After clarification of the themes, the researcher (NA) gave psycho-education on homecare management that can be applied when the patient becomes aggressive.
Results
The sociodemographic details of the participants and the clinical details of the patients are given in Table 1.
Sociodemographic Profile of Participants
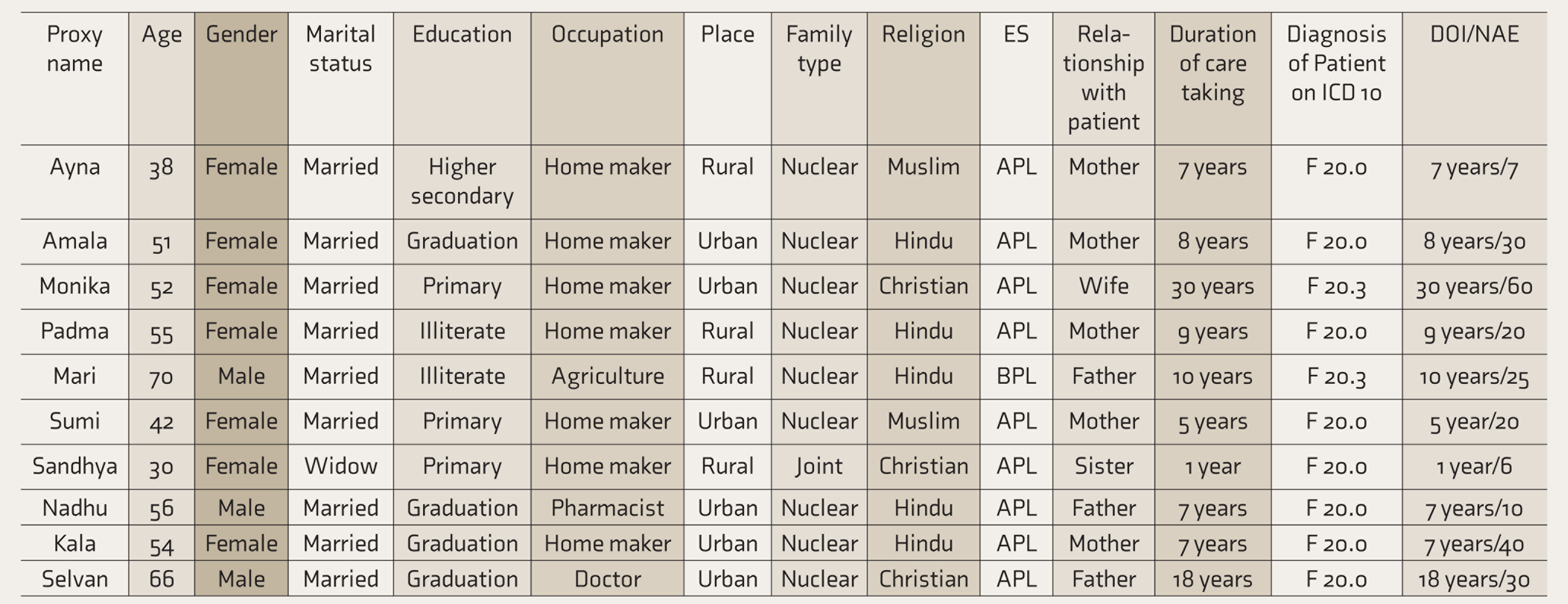
ES: economic status, DOI: duration of illness of patient, NAE: number of aggressive episodes of patient, APL: Above Poverty Line, BPL: Below Poverty Line.
One of the researchers (NA) interpreted the data initially by making filters about own concepts or ideas regarding the data without diminishing the quality or significance of the analysis.
Individual Case Analysis
Each interview was individually analyzed in depth. All audio recordings were translated from the languages Malayalam, Tamil, and Hindi to English and transcribed verbatim. The two researchers (NA, PN) read the lines of text by listening to the recording several times and corrected the text for any errors. After this, coding was done to identify topics, issues, similarities, and differences revealed through the participants’ narratives and they were interpreted by the researchers with a hard copy of the transcript. The qualitative data management software, ATLAS-Ti was used to analyze the transcriptions and code the data. The credibility of the coding was maintained by involving three naive coders. It was also supervised by two research experts (**SG, MM). This helped in the revision of the codes and to clarify the results. 18
Emergent Themes
Each code and transcript were thoroughly examined and brought together as the patterns emerged. These emerging patterns were stated as themes. Some of the themes clustered together and some emerged as master themes.
Cross Case Analysis
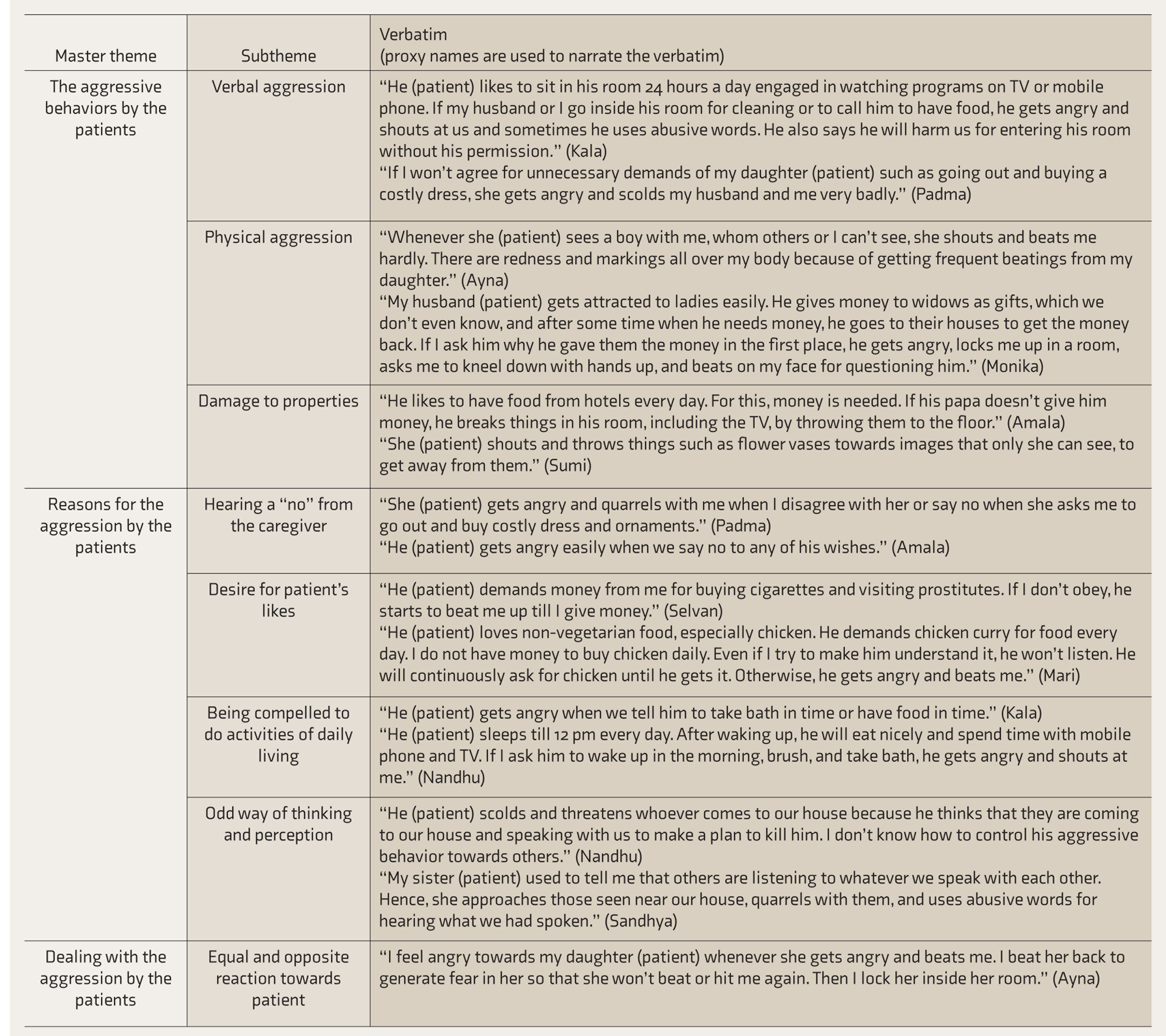
A list of the themes for all the ten interviews was drawn up and patterns were identified across the themes. These were then clustered into master themes and subthemes (Table 2).
Themes Derived
Discussion
This qualitative study explored the lived-in experiences of caregivers of aggressive patients with schizophrenia. The caregivers reported one or the other kind of aggressive behavior from their patients. Most of them experienced multiple types of aggression (verbal aggression, physical aggression, and damage to property). Similar findings were shown by some studies which revealed that aggression could take the form of verbal threats, threats with knives, punches, wrestling, and damage to property. 6 – 8
The reasons for aggression vary from patient to patient. Caregivers reported that their patient’s aggression was mainly because of them denying the patient, their likes, saying no to their demands of wanting to do certain activities, and challenging their own way of thinking and perception. In other studies, the caregivers believed that the patients’ delusions and hallucinations, along with their wish to fulfil their desires and needs, were leading to the patients’ aggressive behavior. 6 , 7 , 9
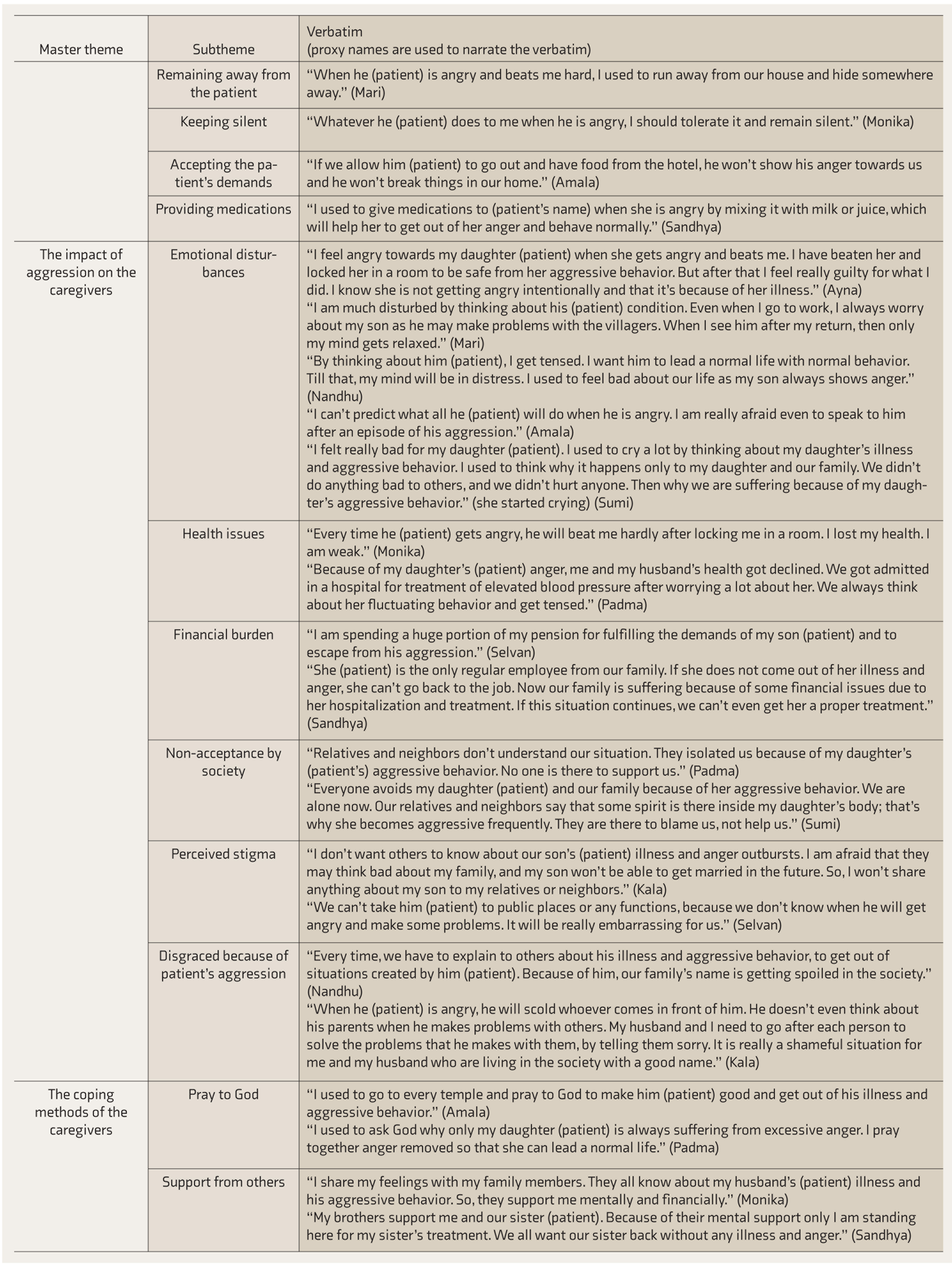
Dealing with the aggressive behavior of patients with schizophrenia was a difficult situation for the caregivers. They were confused about what to do when their patients with schizophrenia became aggressive. They were not aware whether what they did to their patients was right or wrong. Some showed a reaction similar to what the patient expressed to them, while the others became silent, moved away, or accepted the patient’s demands. Others gave medications. Some previous studies too had revealed the practices caregivers adopt to deal with or prevent the aggressive behaviors of their patients, such as close observation, giving advice and reasoning, communication tactics, and taking help from others.9–11
The caregivers experienced emotional disturbances, health issues, financial burden, non-acceptance from society, perceived stigma, and disgrace because of their patient’s aggression. Different studies had revealed similar findings—that the aggression had impact on the caregiver’s emotional, financial, social, and family functioning, including having to manage disruptions by the patient during family gatherings, stress over decisions to commit the patient to hospitalization, non-acceptance by the society, prejudice, and stigma.7, 12–14 Jose reported that the caregivers expressed off-putting personality elements like asociality or introversion, passive attitude, low frustration tolerance, and low self-esteem and also presented with troubling stressors like comorbidities and familial, financial, and legal issues due to their patient’s aggression. 15
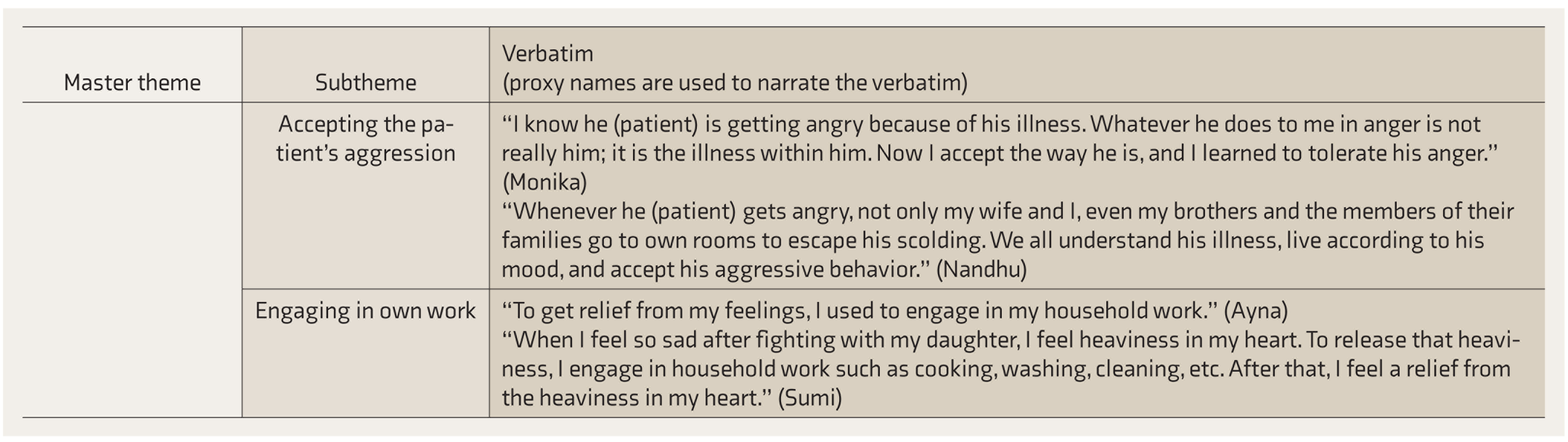
To cope with the aggressive behavior of their patients, they were praying to God, accepting support from others, accepting patient’s aggression, and engaging in their own work. Likewise, other studies had revealed that contacting family, friends, psychiatrists, and neighbors; compassionate feelings; faith in God; self-help approach; acceptance and finding a solution; supportive handling; hopefulness; and religious participation were helpful in coping with the aggression of the patients.12, 16, 17
This was a qualitative research study that resulted in rich data; however, perhaps, a greater depth would have been obtained by adding more exploratory questions. The study cannot claim to represent the full picture of the experiences of caregivers of aggressive patients with schizophrenia.
The study needs to be replicated using a mixed methodology and a bigger sample size, adding the perceptions of professionals, patients, and caregivers of patients with other mental illnesses, and taking into account the patient’s duration of illness and number of episodes of aggression. There is also a scope for further studies with a focus on socioeconomic, demographic, and cultural variations; the difference in perceptions based on the caregivers’ living arrangements; and planning and evaluating interventions to manage the aggressive behavior of patients with schizophrenia.
This study explored the experiences of the caregivers living with their aggressive patients. The results show the need for care and support to the caregivers.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.