
Abstract
Background:
For women with perinatal mental illness, phone helplines may be a useful way of accessing help. This study assessed the feasibility, acceptability, limitations, and usage patterns of a helpline service for mothers discharged from a mother-baby psychiatry unit.
Methods:
Mothers discharged from a mother baby unit during an 18-month period were provided with a helpline number. A social worker answered the calls. Details of the calls, including the reasons and the interventions provided, were recorded. Feasibility and acceptability were assessed by calling all users and nonusers. Satisfaction with the helpline was recorded among users, and reasons for not calling were assessed among nonusers.
Results:
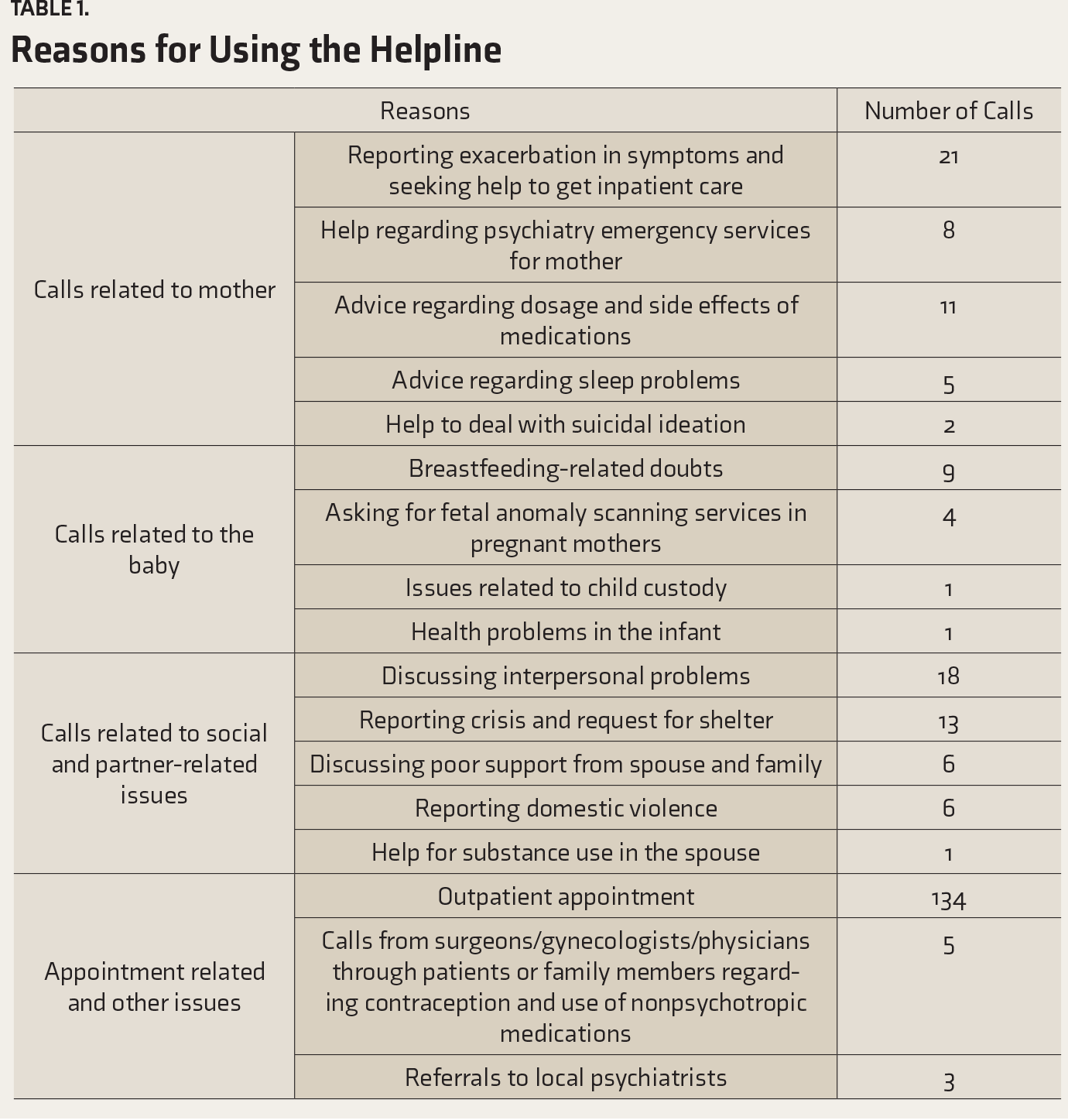
Among 113 mothers, 51 (45%) made 248 calls. Calls were regarding medication, sleep problems, planning pregnancies, symptom exacerbation, appointments, and suicidal ideation. Some calls were related to domestic violence (n = 13, 5.24%), and infant health and breastfeeding (n = 11, 4.44%). Seventy-six (67%, 44 callers and 32 noncallers) were contacted. The majority (41/44) of the callers found it useful: 91% said they got help, and 95% said they would recommend it to others. However, language difficulties (9%) and technical problems (5%) were reported. Among the noncallers, the majority reported having experienced no problem related to mental health or had contacted a doctor. However, of the noncallers, one woman died of suicide, did not have access to a phone, and the family did not choose to call.
Conclusions:
Helpline phone service appears to be feasible and acceptable and can be adapted in other mother-baby psychiatry units in low and middle-income countries. However, in some women, the nonavailability of a phone may be a limiting factor.
Keywords
Mobile phone helplines are feasible, acceptable, and useful to deliver mental health services following discharge from acute care in mothers with mental illness. In low- and middle-income countries, where mobile technology is expanding, phone helpline services can help women with mental illness to access services on their own. Phone helplines can help provide collaborative care from a multidisciplinary team for women with perinatal mental health problems. Despite the gender gap in the ownership of mobile phones in India, nearly 50% of women in this study were able to use the helpline.Key Messages:
In South Asia, mobile ownership in women was 38% less, in comparison to men, at the time of this study.16 Moreover, not much information is available about the feasibility of using phone helpline services among women with severe mental illness (SMI) in LAMIC. Mothers admitted with SMI during postpartum are a particularly vulnerable group. A previous study from the mother baby unit (MBU) at the current study site found that mothers were often readmitted due to poor treatment adherence, social issues, and marital problems.17 While helpline services have been reported as being useful among postpartum women in the community who have concerns about breastfeeding, a similar study has not been done among those with mental health problems, at least in a LAMIC setting.18
While designing a service model, we need to consider the limiting factors for mobile phone based interventions in a low resource and culturally diverse country like India. Cost of the phone service, language and literacy barriers (with the patient and the care provider sometimes speaking different languages), lack of electricity supply, data security, and privacy issues are potential barriers and limiting factors for mobile-technology-based mental health services in these countries.9 Further, even though mobile phone ownership is high, there is a gender disparity in this ownership, and fewer women have access to their own mobile phone.19 In this context, it is important to understand the usage and feasibility of such a service.
This study aimed to assess the feasibility, acceptability, limitations, usage patterns, and users characteristics of a free 24-hour mobile phone helpline for mothers and families discharged from an MBU.
Materials and Methods
This was an exploratory, cross-sectional study conducted in an MBU at National Institute of Mental Health and Neurosciences, Bangalore, India. The MBU is a five-bedded inpatient unit where mothers are admitted with their infants and one caregiver. It is staffed by a multidisciplinary specialist team that provides individualized care based on the complex needs of each mother–infant dyad and the family. All mothers have a caregiver staying with them, usually a female relative. Predischarge counseling and information regarding handling crises and attending follow-up appointments form an important component of care. Mothers are advised to follow-up at the perinatal outpatient service until the infant is two years old.
The mobile phone helpline was started in the month of April 2015. During predischarge counseling, all mothers (both pregnant and postpartum) were given the helpline number in a printed card. The mother and her relatives present at the time of predischarge counseling were provided information about how and when to use the helpline. They were encouraged to use the service during working hours (9:00 am to 5:00 pm) as far as possible, unless it was an emergency. The phone was held by the psychiatric social worker of the perinatal psychiatry team. The psychiatric social worker in the MBU team is part of all clinical discussions and participates in perinatal mental health teaching and training as well. The reason for assigning this task to the psychiatric social worker was related to the prior experience that most of the calls received from this population through the hospital telephone switchboard were for psychosocial support. If the psychiatric social worker was on leave, another team member took over the task. An algorithm (Appendix S1) developed by the multidisciplinary team was used for handling the call, and other team members were contacted in case of need. The algorithm included standard responses for possible questions and standard operating procedures for handling crises such as risk to the mother or the baby, an exacerbation of symptoms, or a risk of suicidality. Medical queries were discussed with the psychiatrist in the team. In case of self-harm or other health risk, mothers or their family members were advised to contact the local psychiatric emergency services or reach our hospital psychiatric emergency service. Mothers who reported domestic violence and required shelter and safety were either advised to come to the perinatal psychiatry clinic and/or appropriate services and referrals were provided to other agencies. Those who did not have any acute or serious issues related to health were provided advice over the phone or asked to come for an early follow-up at the perinatal psychiatry clinic.
Call Logs and Records
Details of each call were systematically documented. Following each call, details recorded included the identity of the caller, relationship to the patient, the reason for the call, and details of the advice provided. The Institute Ethics Committee approved the study. All mothers provided informed consent.
All the mothers (113) admitted from June 2015 to December 2016 (18 months) were contacted six months after their discharge. The first author prepared a list of the callers and noncallers. To assess the acceptability of helpline mobile phone services, all the mothers (113) who were provided the helpline number during the study period were contacted. Callers were asked a set of questions related to usefulness and satisfaction, and the noncallers were asked the reasons for not using the helpline. To assess the feasibility of helpline services, the psychiatric social worker from the team attending the calls was asked a set of open-ended questions (Appendix S1).
Data Analysis
All call details were tabulated, and each item of the reasons for calls and interventions provided was coded to form categories, independently by first and last author. Any differences were resolved by consensus and discussion with the second author.
The sociodemographic and clinical data and the responses to the acceptability and satisfaction questions were reported as frequencies.
Results
At the time of admission in the MBU, the mean (±SD) age of the mothers in years was 24.59 (±5.24), and the age of infants ranged from 7 days to 1 year 2 months. Of the 113 mothers, 107 were in the postpartum period, and six mothers were pregnant. Also, 38% (n = 43) were from urban and 62% (n = 70) from rural areas. One-third of the mother–infant dyads were from Bangalore, a third from other districts of the state of Karnataka, and 36.28% (n = 41) from other states of India. Half the mothers belonged to the below poverty line (BPL) category as per the Government norms. Nearly 50% of the mothers had low literacy (illiterate or primary level education, i.e., ≤7 years), 38.94% (n = 44) had secondary education, and 14% (n = 12) had a college education. All mothers received an International Classification of Diseases (ICD) 10 diagnosis. Acute and transient psychotic disorder (ATPD) was seen in 32% (n = 36), 20% (n = 23) had bipolar affective disorder (BPAD), 20% (n = 23) had depression, 15% (n = 16) had schizophrenia or other nonaffective psychosis, 5% (n = 6) had obsessive compulsive disorder, 4.5% (n = 5) had organic psychosis, and 3.5% (n = 4) had dissociative disorders.
Usage Pattern of the Helpline Mobile Phone Services
The total number of calls received on the helpline was 248. Of these, 42% (n = 104) were made by the mothers themselves, 48.3% (n = 120) were made by the spouses, and the rest, by other family members.
Reasons for Using the Helpline
Acceptability of the Helpline Mobile Phone Services
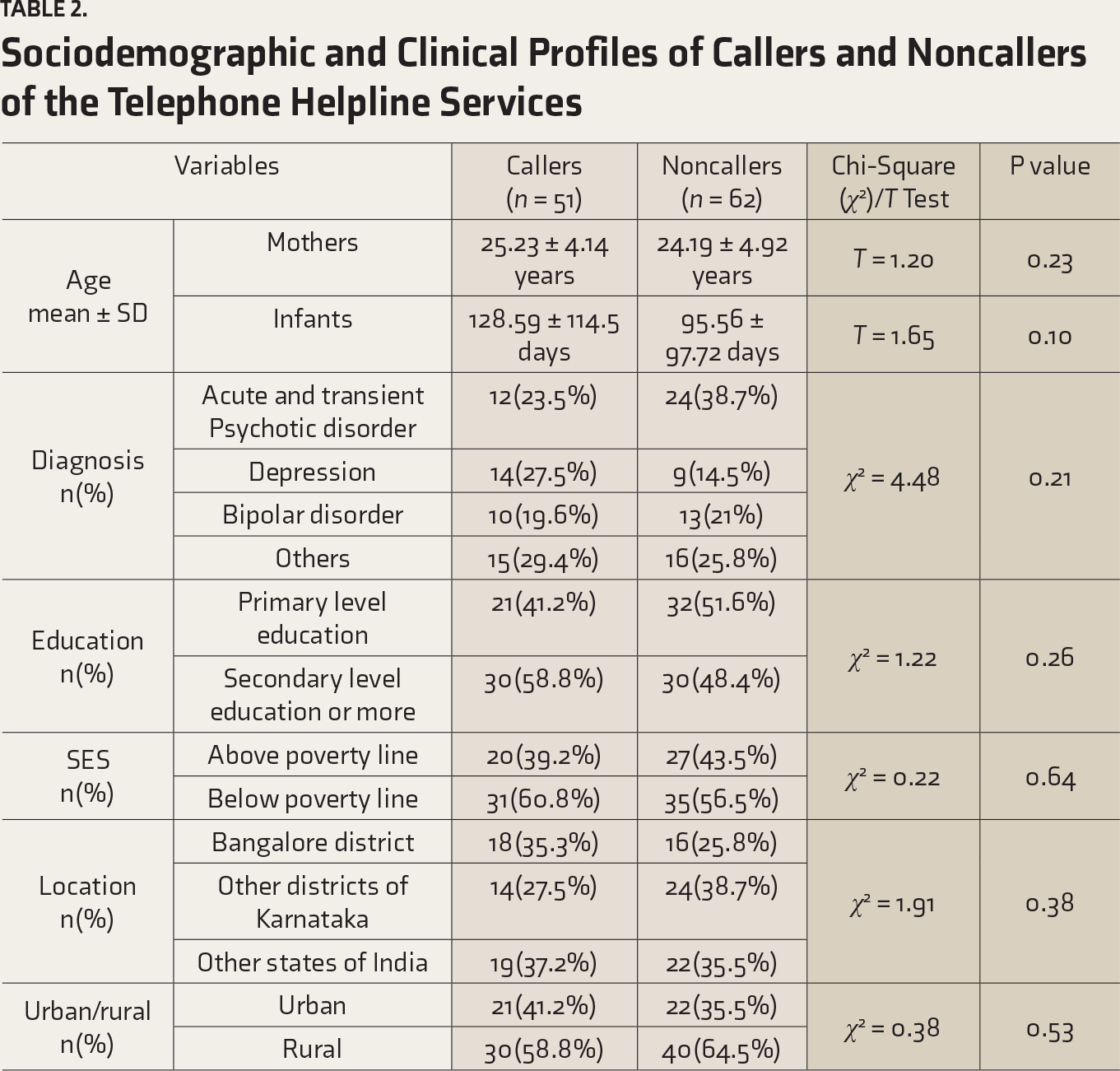
Out of the 113 mothers, we were able to contact 76 mothers or family members to assess the acceptability and satisfaction. Of the 76, 57.9% (n = 44) had used the phone helpline. Fifty percentage (n = 22) of the calls were made by spouses, 40.9% (n = 18) of the calls were by the women themselves, and a minority, by other relatives. There were no differences in the sociodemographic or clinical profile between the callers and noncallers (
Sociodemographic and Clinical Profiles of Callers and Noncallers of the Telephone Helpline Services
When asked about the usefulness of the helpline, of the 44 users, 93% (41) said that it was a useful service, 91% (40) said they got a helpful response, 95% (42) said they would recommend this service to others, 9% (4) reported language and communication difficulties, and 5% (2) reported problems in getting in touch. The average rating of the service was 8.96 (minimum 7, maximum 10).
Feasibility of Handling the Helpline Mobile Phone Services
The psychiatric social worker who was in charge of answering the helpline and held the phone, reported feeling comfortable in handling the calls. Other team members were perceived as being supportive, and the standard algorithm, as well as standard operating procedures for handling crises, were found to be helpful. A few difficult situations included the following:
Communication issues if the patient and the social worker spoke different languages or dialects. Difficulty in handling matters related to interpersonal relationships over the phone. Difficulty in persuading the family members and the patient about the need for inpatient care if there was a suicidal risk or relapse/exacerbation of symptoms. Difficulty in contacting the local psychiatrist in case of psychiatric emergencies.
Discussion
This study, which looked at the usage patterns of a phone helpline service within six months following discharge, and preliminary feasibility, found that nearly half the mothers admitted to the MBU used the helpline. Another important aspect was that nearly 50% of the calls were made by the women themselves, indicating that even in a society where women with mental illness may not have much agency,20 the availability of a mobile phone increases the chances of them seeking help for a variety of social and medical reasons. However, for the mother who died due to suicide, the phone number provided was that of her brother. This highlights the need for more focused communication with the mothers regarding the helpline, especially if they do not own a phone. The focused communication might include asking the mother to save or note down the helpline number, which she can use at the time of crisis, and discussing a crisis plan for accessing the helpline if she did not have access to her own phone.
Very few studies have assessed the use of postdischarge helpline services in psychiatric settings. A nurse-led telephonic intervention on physical, psychological, and social aspects of care for women with endometrial cancer showed that patient satisfaction was high.21 In India, the government-initiated helplines for reproductive health and HIV/AIDS have been quite popular.22 However, in the field of mental health, before the COVID-19 pandemic, most helplines have been used for suicide prevention,12,19,23–26 and only a few for other aspects of mental health.27
Among postpartum women, the PANDA (Perinatal Anxiety & Depression Australia) National Helpline offers support to callers facing emotional health challenges in the perinatal period.13 A study that analyzed patterns of help-seeking and reasons for contacting the PANDA service found that majority of the women who sought help were either pregnant or having a child ≤12 months of age. The reason for seeking support was depression, anxiety, and thoughts of suicide or self-harm. Women with perinatal mental illness reported positive experiences of accessing support from that helpline, which was described as being accessible and acceptable.13 A study describing a telephonic lactation support program showed that mothers often used the service to clarify breastfeeding-related doubts.28
All these studies among women in the perinatal period, albeit from high-income country settings, indicate the demand for phone helplines for this vulnerable population. Women with mental health problems who have recently given birth, especially in LAMI countries, may find it difficult to travel to avail timely support. The high penetration of mobile phone services and the ability of women to get medical and psychosocial support when they are in need, indicate that such a service is very important.
The strengths of the present study include systematic recording of all the data regarding the content of the calls and categorization by two independent authors and inclusion of women with SMI (most studies on helplines among perinatal women have focused on women with depression and anxiety) and women with low literacy levels (indicating that it can be a useful and cost-effective form of intervention for this group of women).
The main limitation of the study is that we could not get in touch with all the mothers to whom the helpline number was provided.
It is important to call a helpline at times of crisis, and hence the ways in which access to the helpline can be enhanced need to be explored in future studies. Some of the measures to enhance the helpline access include (a) ensuring that the mother and the most important care provider, rather than any relative who is present at the time of discharge, is given the helpline number, (b) ensuring, in all mothers, especially those with low literacy levels, that the phone number is entered into their mobile phones and encouraging them to make a test call before leaving the hospital, and (c) discussing with the mothers the various forms of help that we could provide and the confidential and collaborative nature of the service, so that they feel comfortable using the helpline even in their most distressing moments.
Conclusion
Following discharge, women with SMI who were admitted to MBUs may have complex needs related to their illness, the infant, and psychosocial problems. Telephonic access to a dedicated multidisciplinary team that practices collaborative care and promptly handles the aforementioned needs is necessary. Our helpline users reported a positive experience of using the service and mentioned that they would recommend the service to others with similar issues. A dedicated team member could handle the phone with support from the multidisciplinary team, without feeling unduly burdened. The helpline appears to be feasible, acceptable, and useful in most instances and can be used in other LAMIC settings.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.