
Abstract
Background:
Psychotherapists, while treating clients with a history of traumatic experiences, are exposed to vicarious trauma, which affects their mental health as well as their quality of caregiving. The present research tries to gain an insight into the lived experiences of psychotherapists while treating clients with traumatic experiences.
Methods:
In-depth individual interviews were conducted with five psychotherapists (two males and three females) with a minimum duration of continuous professional practice of 3.5 years and all of them above 30 years of age. The interviews were conducted for 30–45 minutes and recorded after taking informed consent from the participants. The data was analyzed and interpreted using the interpretative phenomenological analysis. Investigator triangulation was done to ensure the trustworthiness of the research.
Results:
The analysis reveals that the participants have experienced vicarious trauma from their therapeutic interaction with their clients on their traumatic issues, particularly during the initial phases of their career as a psychotherapist. Some of them feel that such experiences, despite being distressing, have also empowered them psychologically. The participants have reported using constructive coping strategies to deal with such vicarious trauma, such as emotional distancing, journaling, seeking personal therapy and social support, reading, physical exercise, and self-care activities.
Conclusions:
Psychotherapists working with trauma survivors often face vicarious trauma, but these experiences can also foster growth and resilience. Self-care and professional support help therapists manage these effects and sustain practice.
Keywords
Therapists experience vicarious trauma while working with trauma during initial years of practice. Therapists use various constructive coping strategies such as emotional distancing, journaling, seeking personal therapy and social support, reading, physical exercise, and self-care activities to deal with vicarious trauma.Key Messages:
Psychotherapists are supposed to provide a safe space to their clients by allowing them to share their experiences and agonies. However, there is a psychological cost of taking care of other people’s emotional ordeals, making the psychotherapist vulnerable to experiencing emotional burdens. 1 A critical component of psychotherapy is being compassionate and empathic and, in the process, helping clients get relief from distressing and intrusive thoughts and emotions. Repeated exposure to negative emotional experiences of clients and the confrontation with human frailties may take a toll on the mental health of psychotherapists, which in turn may manifest in terms of physiological and interpersonal disturbances, leading to the decline of overall well-being in psychotherapists. 2 One such construct is compassion fatigue (CF). The construct of CF is analogous to constructs such as “burnout” and “vicarious traumatization,” all of which represent the “cost of caring” in mental health professionals, that is, absorbing the agony of clients. 3 “CF is the negative aspect of providing care, which manifests exhaustion, frustration, anger, and depression typical of burnout, or a negative feeling driven by fear and work-related trauma.” 4
Further, in the process of alleviating the distress of their clients, psychotherapists cannot expect reciprocation, and the rewards of successful psychotherapy are thus elusive. 5 Such a detrimental effect on the psychosocial functioning of psychotherapists may also pose risk factors for adequate care of clients. 2 However, research on the psychological stress emanating from long-term exposure to the suffering of others is not adequate and has yielded ambiguous results. For example, research findings are inconsistent in terms of the risk factors associated with emotional exhaustion in healthcare professionals, such as the role of gender, age, experience, workload, and personality of the psychotherapist.6, 7 Also, there are contradictory findings about the physical and psychosocial impact of such emotional exhaustion, such as gastrointestinal problems, sleep disturbances, fatigue along with increased irritability, cynicism, depression, disturbed interpersonal relationships, compromised patient care, substance dependence, etc.8–10 In such a scenario, it is important to understand the personal experiences of psychotherapists while they conduct psychotherapy. This will open up avenues to explore the many nuances of shared experiences of trauma and to delineate the risks and protective factors associated with such experiences for psychotherapists. Hence, the present study endeavors to use a phenomenological analysis to explore the lived experiences of vicarious trauma in psychotherapists.
Methods
Participants
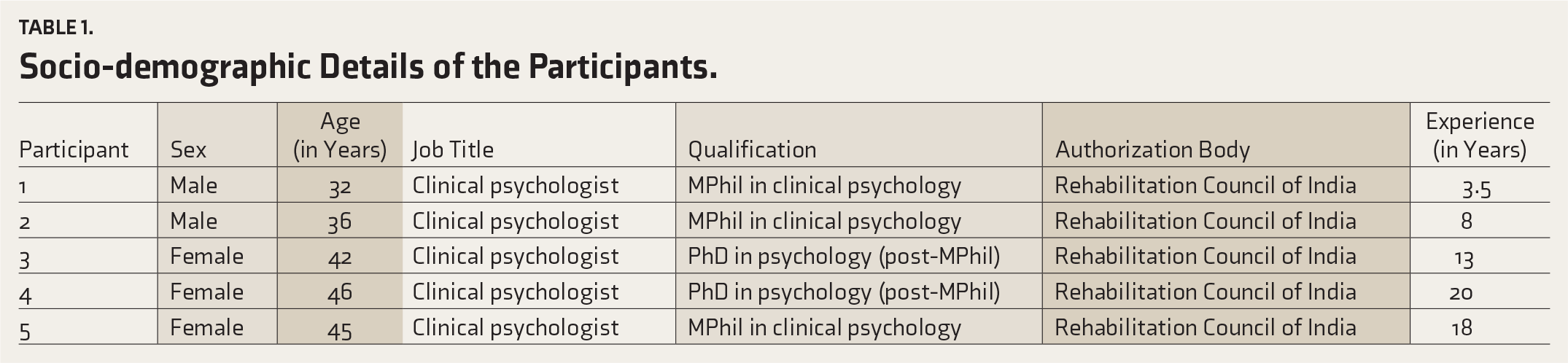
The participants of the study consisted of five psychotherapists. As defined by the APA Dictionary of Psychology, an individual who has undergone professional training and is licensed to treat problems of an emotional and behavioral nature by psychological means is a psychotherapist.¹¹ The current study participants have a minimum qualification of MPhil in clinical psychology from institutes affiliated with the Rehabilitation Council of India. All the participants are in continuous professional practice and use integrative psychotherapy. None of the participants specialized in any particular form/mode of psychotherapy or identified the treatment of any particular group of disorders as their area of expertise. The duration of practice was seen to range from 3.5 years to 20 years. Two male participants and three female participants were 32–46 years old (Table 1). The participants did not report any history of traumatic experiences in the last six months prior to the study. The nature of sampling was “purposive” and “snowball.” The principle of “variation” was kept in mind while selecting the participants; the participants varied from each other in terms of their age, sex, and duration of practice. It was ensured that each participant varied from the prior participant on at least one of the tenets of variation (age, sex, and duration of practice) chosen in the study. For instance, the second participant varied from the first regarding experience, while the third participant varied from the second concerning age, sex, and experience. The study was conducted in Kolkata, and data was collected between January and April 2021.
Socio-demographic Details of the Participants.
Tools Used
Socio-demographic data sheet: The socio-demographic data sheet was prepared for the study to elicit socio-demographic information about the participants, such as age, sex, profession, educational qualification, and years of working experience.
In-depth interview: A semi-structured interview schedule was constructed based on the literature review on psychotherapists’ experiences in conducting therapy. The questions were mostly open ended, giving the interviewee the flexibility to answer on their terms. The questions centered on areas such as the duration of being actively in this profession, general experiences of being a psychotherapist, etc. and other questions related to skills and coping styles used to cope with vicarious trauma. However, these questions were framed contextually based on the interview flow.
The interview schedule is provided in Appendix A.
Procedure
The goals and purpose of the study were explained to the participants, and written consent was obtained from all of them after ensuring confidentiality and anonymity of the data obtained. The first author contacted the participants and conducted interviews. Each participant was given prior notice before the interview, and it was scheduled with the participants’ comfort and preferred time kept in mind.
Two interviews were conducted in person, while the other three were via video call. All the participants were given the same set of questions, but the order of the questions asked varied according to the flow or direction of the interview. The researcher was mindful of the sensitivity of the research topic, and the participants were reminded to leave if they felt any discomfort during the interview process.
All five interviews lasted between 30 and 50 minutes. All the interviews were audiotaped with the participants’ consent. The participants were not interrupted and were given scope for clarification when required between the interview sessions. Data for each individual was collected until the questions revealed no new information from the participant, thus attempting data saturation.¹² The interviews were anonymized and transcribed word-to-word by the first author, including pauses, gestures, and changes in pitch and tone, to catch the overall feeling and tone. Field notes were taken by the first author during the interviews, with the consent of the participants. The field notes aided the researchers during data analysis as they lent further nuances to the data.
Choice of Qualitative Analysis and Its Rationale
Interpretative phenomenological analysis (IPA), proposed by Smith et al.,¹³ analyzes and interprets the lived experiences of individuals who are considered meaning-making agents. Psychotherapists, in their work with clients’ trauma, can be considered to be dealing with ambiguous, emotionally laden, and multilayered phenomena that demand personal meaning-making. Hence, IPA was deemed suitable for this study.
Analysis
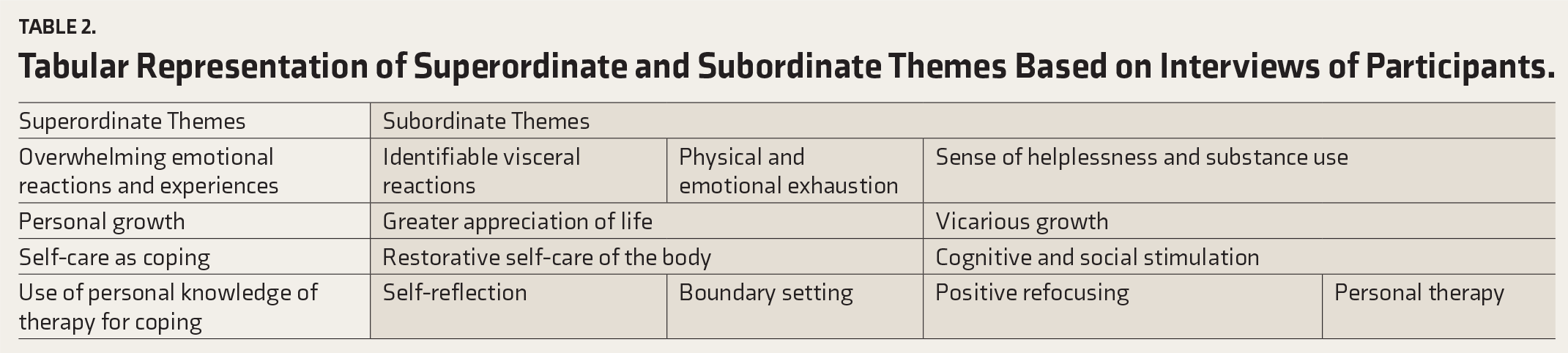
At first, all five interviews were recorded and transcribed. The analysis of the transcription was done manually to make the researchers familiar and engage themselves with the participant data. Subordinate themes were constructed by following the principles of “double hermeneutics” espoused by IPA. Subordinate themes were listed chronologically based on their appearance in the transcript. Then, they were organized together in terms of content similarity. Then, at the final stage, the superordinate themes were created by seeking the commonalities between the themes that emerged across the participants’ transcripts (Table 2).
Tabular Representation of Superordinate and Subordinate Themes Based on Interviews of Participants.
The Trustworthiness of the Data
“Investigator triangulation” was used to increase the credibility of the data. The data were interpreted by three researchers (all three authors), and only themes based on mutual consensus among the researchers were considered. In the case of disagreement among researchers, the emergent theme was discussed, its relationship to the data was examined, and then those endorsed by at least two researchers were retained in keeping with the tenets of the method of investigator triangulation.
Ethical Consideration
The purpose of the research is to study the lived experiences of psychotherapists working with trauma. As the research is about human experience, a semi-structured interview was conducted to get an in-depth understanding of the respondents’ beliefs and feelings. A detailed briefing about the nature and purpose of the study was given to the participants before the study was conducted. The participants were informed that there would be no immediate benefit from participating. They were free to refuse or withdraw participation at any point, without any detrimental consequences. The anonymity and confidentiality of the participants were preserved by not revealing their names and identities in the data collection, analysis, and reporting of the study findings. Prior consent was taken from each participant before starting the study, and it was informed that the information would be used purely for academic purposes only. Additionally, the study was approved by the Dept. Ethics Committee, Dept. of Psychology, NSHM Knowledge Campus, Maulana Abul Kalam Azad University of Technology, prior to data collection.
Reflexivity
The primary researcher/first author chose this research topic as part of the requirement of a postgraduate degree. She was interested in the study of trauma and how it affects individuals dealing with it directly or indirectly, namely, vicarious trauma. The researcher was particularly curious to explore the therapists’ experience of working with clients with trauma and how they dealt with their emotions and reactions/thoughts evoked in the process. As a postgraduate student and a sensitive individual learning about theories of causation of disorders and approaches to their treatment, she held the position that therapists would experience mental strain and emotional burden in the course of their work. She contacted the first participant, whom she knew previously through an internship, and found other participants through snowball sampling and the contact of the second author.
The primary researcher felt that the information she gathered from her participants reinforced many of her beliefs regarding the stress and strain experienced by psychotherapists. She also gained new insights about the psychotherapy process.
Though not actively involved in the data collection, the other two researchers were involved in the analysis. One of the co-researchers (co-author), a practicing psychotherapist, felt that many of her feelings and thoughts resonated with the participants’ anecdotes and reflections. The third co-author/co-researcher, though not actively involved in psychotherapy practice, is indirectly involved in supervising trainee psychologists. She also felt that her theoretical knowledge and partial experiences related to psychotherapy concurred with the perspectives of the participants and also helped her reintegrate her understanding of the subject.
Results
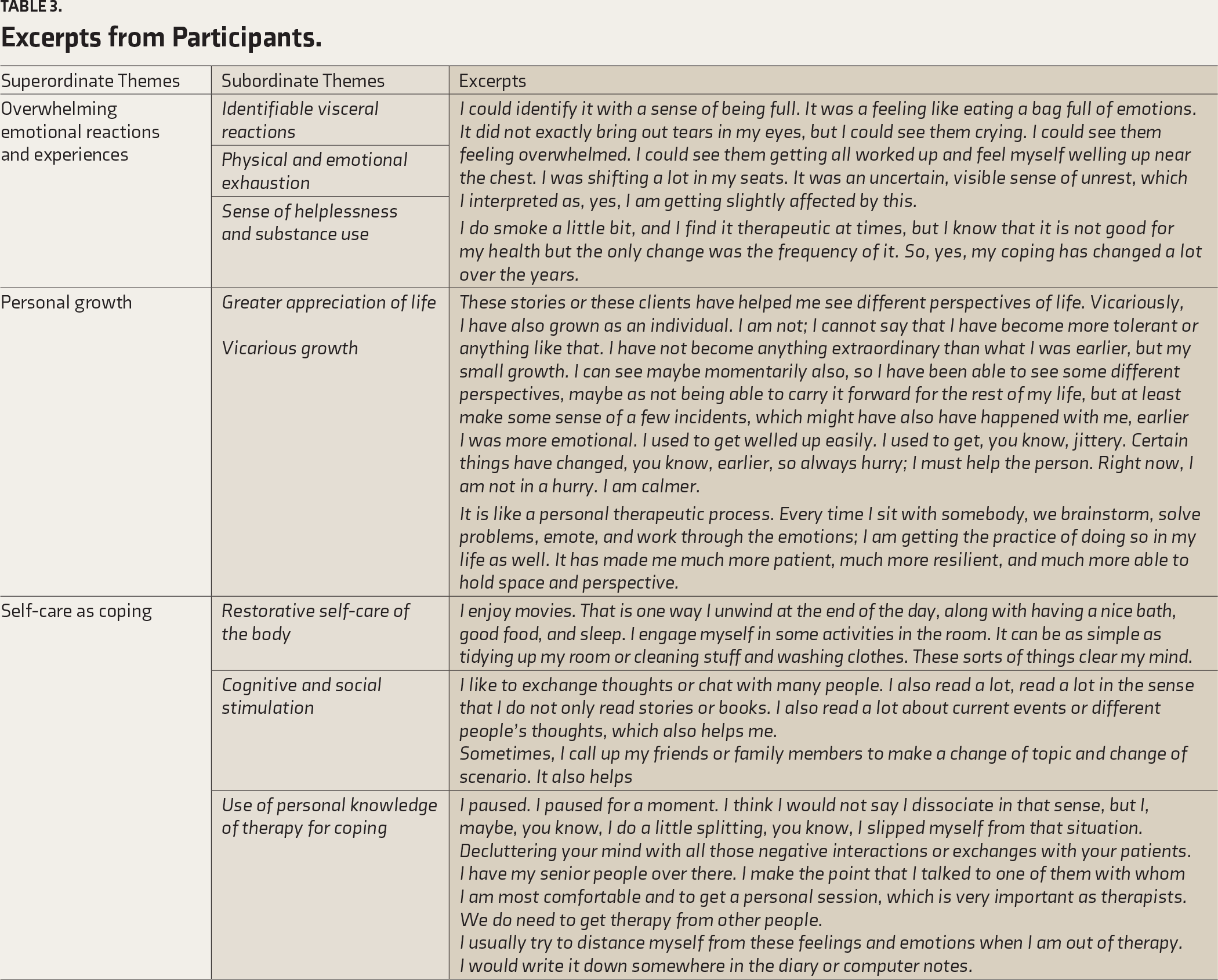
Selected excerpts under corresponding subordinate themes are provided in Table 3.
Excerpts from Participants.
Discussion
Mental health professionals must encounter unprecedented emotional challenges while dealing with clients with critical life experiences to share. The participants of the study, who were all practicing psychotherapists, reported personal experiences of getting emotionally overwhelmed when they were treating clients with a history of trauma. Such emotional experiences were often accompanied by visceral reactions such as an increased heart rate, sweating, tears welling up in the eyes, choking throat, etc. Vicarious trauma, that is, indirect experience of trauma, is a natural response to “trauma work” in therapy. 14 Similar findings have also been obtained more recently. 13 “Trauma work” in psychotherapy can be described as “living in an ocean of stressful emotions.” A significant finding of this study was that psychotherapists reported experiencing stressful emotions while working with traumatized clients more frequently in the early phases of their careers. 15 This finding can be substantiated by findings from other studies, which say that younger healthcare professionals and professionals with fewer years of experience are more susceptible to developing compassion fatigue and burnout.16–18
Though secondary experience of trauma has been reported to have physical and psychological effects, the psychotherapists in this study also acknowledge that they have experienced psychological growth while experiencing indirect trauma in the process of helping their clients. Various research evidence imply that the consequences of “trauma work” in psychotherapy are not invariably negative. Psychotherapists treating trauma survivors also report enhancements in interpersonal relationship skills, greater appreciation of the basic human spirit, and increased spiritual and personal growth.19–21 Calhoun and Tedeschi proposed that positive experiences as a sequel to critical life events can be categorized into (a) changes in self-perception, (b) changes in interpersonal relationships, and (c) changes in philosophy of life. It is noteworthy that psychotherapists also provide anecdotal evidence in favor of perceived growth in the wake of vicarious experience of trauma in the domains of self-appraisal, relationships, and life’s greater purpose. 22 Other researchers have also reported that psychotherapists working with trauma survivors experience newer psychological strengths such as opening to new possibilities, appreciation of life, and spiritual upliftment, as well as enhancement of professional skills and a unique sense of satisfaction and competence in seeing the client heal.23–25
The psychotherapist participants in this study have consistently spoken about using active behavioral strategies to ward off the inevitable stress of dealing with clients’ trauma. Similar findings have also been obtained in other research trying to elucidate the coping strategies used by psychotherapists, such as disengagement, self-distraction, spending time with friends and family, and seeking help from supervisors, which match the anecdotes of the participants of this study.26–28
Psychotherapists in this study have also reported using personal care strategies as soothing techniques during times of emotional over-arousal/personal distress while helping trauma survivors. A study has investigated how mental health practitioners used self-care and found that personal self-care activities include physical self-care, a healthy diet, exercising, watching movies, reading books, spending time with friends, etc., all of which are like the ones reported by the participants of this study. 29
One of the participants also pointed out that a history of personal trauma can intensify the distress that the psychotherapist experiences while having to care for a traumatized client. Similar findings have also been reported, that is, psychotherapists with a history of trauma are more at risk of developing compassion fatigue. 30
CF is frequently prevalent among mental health professionals, and it has been proposed that CF reduces one’s ability to express compassion and bear the suffering of others.31–32 Such a phenomenon has a crucial and detrimental connotation for psychotherapy.
However, in this study, interestingly, none of the participants reported psychological distress and associated professional incapacitation in the wake of guiding clients through their suffering, which was intense enough to qualify for CF.
Such a finding may have significant implications related to psychotherapists’ cultural backgrounds. A study has posited that mental health professionals’ ethnic backgrounds may influence how they cope with vicarious traumatization. 33 In this context, some studies have examined the cultural background and individualistic-collectivistic values of individuals about empathy and found that Asian students endorsed more collectivistic values and showed more empathy, in alignment with traditional views on collectivism and perspective-taking.34–36
Conclusion
Caring for others is a conscientious yet difficult task that drains the caregiver’s physical, financial, and emotional resources. This is the same for informal and formal/professional caregivers. In the case of formal/professional caregivers, the cost of caring is uniquely problematic as bound by professional ethics; these professionals are obligated to absorb the trauma and agony experienced by their clients/patients, which, in turn, detrimentally affect their holistic well-being. The present research used a qualitative framework of research to explore the subjective experience of distress in mental healthcare professionals and their ways of dealing with that distress.
The major findings of the research reveal that all of the participating professional psychotherapists experienced overwhelming emotions at times while dealing with their clients’ agonies. They also experienced personal and professional growth in dealing with such emotions. Also, along with using their professional skills to cope with the negative emotions, the participants universally suggested the importance of self-care in maintaining personal well-being.
Ferenczi, at the beginning of the 19th century, can be credited as the pioneer of studying the psychological impact of working with traumatized patients on psychotherapists. Later, in the second half of the 1990s, other clinicians also began to show interest in complex trauma-related disorders and the aftermath of treating these disorders on psychologists.21, 37 Though these clinicians might have varied opinions regarding the explanation of vicarious trauma, they have agreed that in the process of healing traumatized clients, therapists are psychologically affected, and this, in turn, affects their therapy. The findings of the present study can thus be considered an important addition to the existing literature on the psychological aftermath of psychotherapy with clients having a history of trauma.
However, the study would be further enriched with a larger sample size. The ethnic/cultural background of the participants could be considered as a tenet of variation. That would give nuanced perspectives, and findings could be contextualized better in the diverse, multilingual, and multicultural country of India. Data saturation or theoretical saturation could not be achieved as the study’s sample size was too small. Member checks would have further enhanced the study’s credibility but could not be done due to the paucity of time.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethical Approval
The current study was approved by the Ethics Committee, NSHM Knowledge Campus, Maulana Abul Kalam Azad University of Technology.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written consent was obtained from all participants.