
Abstract
Background:
Intimate partner violence (IPV) is one of the major public health problems. Little is known about the extent of violence experienced, its severity, or history of childhood abuse or exposure to intergenerational family violence in women with mental illness.
Methods:
One hundred women seeking in-patients (IP) or out-patients (OP) services at a tertiary care psychiatric setting were recruited using consecutive sampling. IPV Questionnaire and Danger Assessment Questionnaire were administered.
Results:
The data revealed a moderate level of IPV experienced by the women. In their childhood, more than one-third had undergone physical abuse by their fathers and witnessed violence by fathers toward mothers.
Conclusion:
Screening for intimate violence is essential in women attending mental health settings.
Three-fourth of the women developed the psychiatric illness after marriage, and IPV could have been one of the stress factors for developing mental illness secondary to ongoing violence. Mental health professionals must routinely screen for IPV, provide the needed help, and connect the survivors to service organizations in the community.Key Messages:
The current research aimed toward assessing forms of IPV, severity, lifetime victimization, history of witnessing family violence, and services expected from mental health professionals at a tertiary care psychiatric hospital by women with mental illness (WMI).
Materials and Methods
The research was a cross-sectional study, and exploratory analysis was carried out to analyze the data. The study was carried out at National Institute of Mental Health and Neurosciences (NIMHANS), a tertiary care hospital located in Southern Bengaluru, India. The study was carried from January 2017 to June 2018. A sample of 100 women was recruited using consecutive sampling and the following inclusion and exclusion criteria: those aged 18–55 years, speak Kannada or English, availing services in OP and IP adult psychiatric care, under remission without active psychopathology, and who are vocal and able to participate in the interview were included. Those with intellectual developmental disorder, neurological disorders, organic psychiatric disorders, or history of substance abuse were excluded. Informed consent was obtained from all the participants at the time of recruitment. Consent was obtained from the family members to interview the patients. The study was approved by the Institute Ethical Committee. The patients were interviewed by a trained social worker of the primary project that aimed to assess the pattern of IPV among WMI and mental health professionals’ knowledge, attitude, and preparedness to respond to IPV. Part of the larger study was published by Vranda et al.31,32
Operational Definitions
Physical violence includes the use of physical force against another—slapping, hitting, throwing objects, pushing, burning, strangulating, and beating, often leading to permanent injuries and sometimes even death.
Sexual violence involves the violation of an individual’s bodily integrity, including coercing sexual contact, rape, as well as any unwelcoming sexual behaviors. This includes forcing unwanted sexual acts, withholding sexual intimacy, making degrading comments about someone’s sexuality or attractiveness, and rape.
Psychological violence includes the use of controlling behaviors, isolating from families and friends, denying social contacts, threatening, humiliating, insulting, manipulating, withdrawing affection, and using abusive language that cause the victim to feel afraid, humiliated, confused, powerless, inadequate, or overwhelmed.
Emotional violence is defined as withholding/controlling the access to financial resources, not allowing the victim to work, and withholding necessities.
Lifetime victimization is defined as multiple traumatic victimization experiences that occur across the developmental periods, that is, in both childhood and adulthood. In this study, we assessed multiple forms of violence experienced from childhood to adulthood by multiple perpetrators.
Materials
Sociodemographic and clinical profile: The researchers prepared a sociodemographic data sheet to collect the background information. It covered demographic information, duration of abuse, history of lifetime victimization, previous help sought to prevent violence, and expectations from mental health professionals.
Danger Assessment Questionnaire: This is a six-item questionnaire developed by this research team (
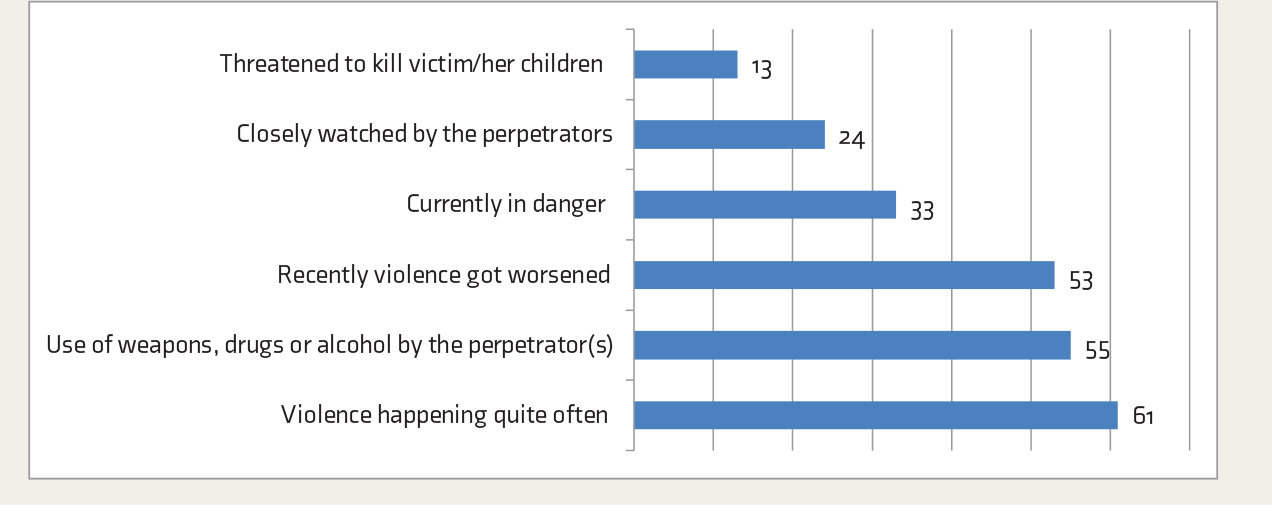
Nature of Danger Experienced by Women on the Danger Assessment Scale
Screening of IPV Questionnaire 8 : This consists of 58-items, with four domains: physical violence (18 items), psychological violence (23 items), economic violence (seven items), and sexual violence (ten items). It assesses the different forms of violence experienced by women from their partners. The responses for each item are “Never,” “Rarely,” “Sometimes,” “Usually,” and “Always,” on a 5-point Likert scale. Higher scores indicate a higher level of violence. The scale has good face validity, and as for consensual validity, the scale was validated by ten mental health experts from NIMHANS (i.e., three additional professors of psychiatry, four assistant professors of psychiatric social work, and three assistant professors of clinical psychology) who found it to be useful in assessing domestic violence among women.
Statistical Analysis
Descriptive statistics was used to analyze the sociodemographic variables. Welch’s ‘t’ test was used for categorical variables and Pearson’s correlation coefficient was used to examine the relationship between continuous variables. For analysis, Statistical Package for the Social Sciences (SPSS) version 20 was used.
Results
Descriptive Statistics
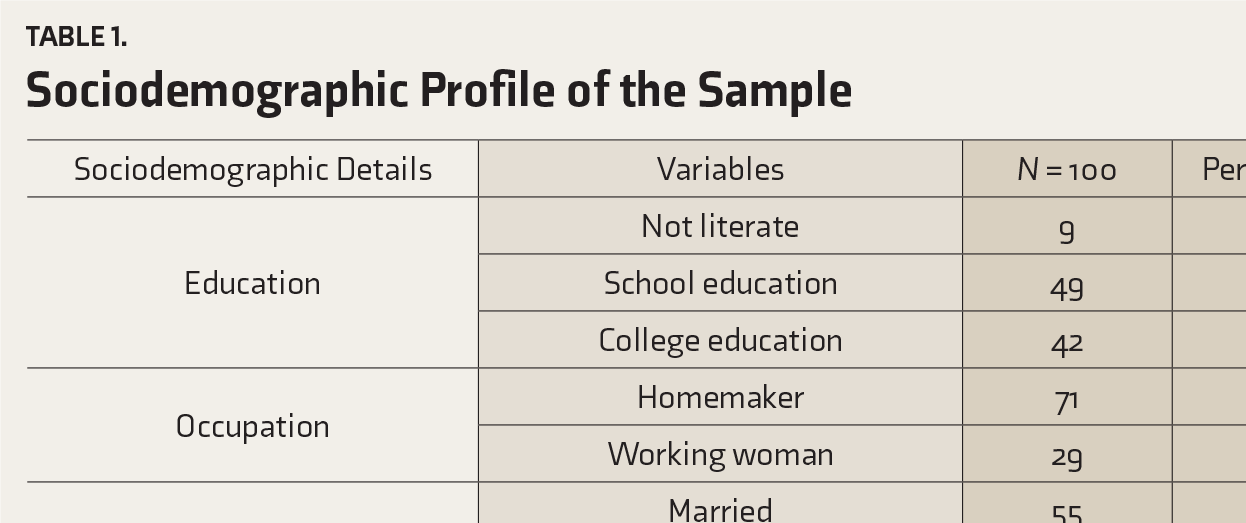
The age of the participants ranged from 18 to 55 years, with a mean of 34.2 (SD = 8.97). The majority (91%) were educated. A total of 49% had a primary school education. Three-fourths of the women were homemakers. The mean family income was Rs 8620.69 with SD 10910.88. A total of 55% of women were married, and two-thirds (33%) were either separated/divorced. The majority (76%) had children. The mean number of children was 1.79 with SD: 0.66. A total of 62% of women were diagnosed with affective disorders (such as bipolar affective disorder, postpartum psychosis, and depression) and the onset of the psychiatric illness was after the marriage for the 83% of the women (
Sociodemographic Profile of the Sample
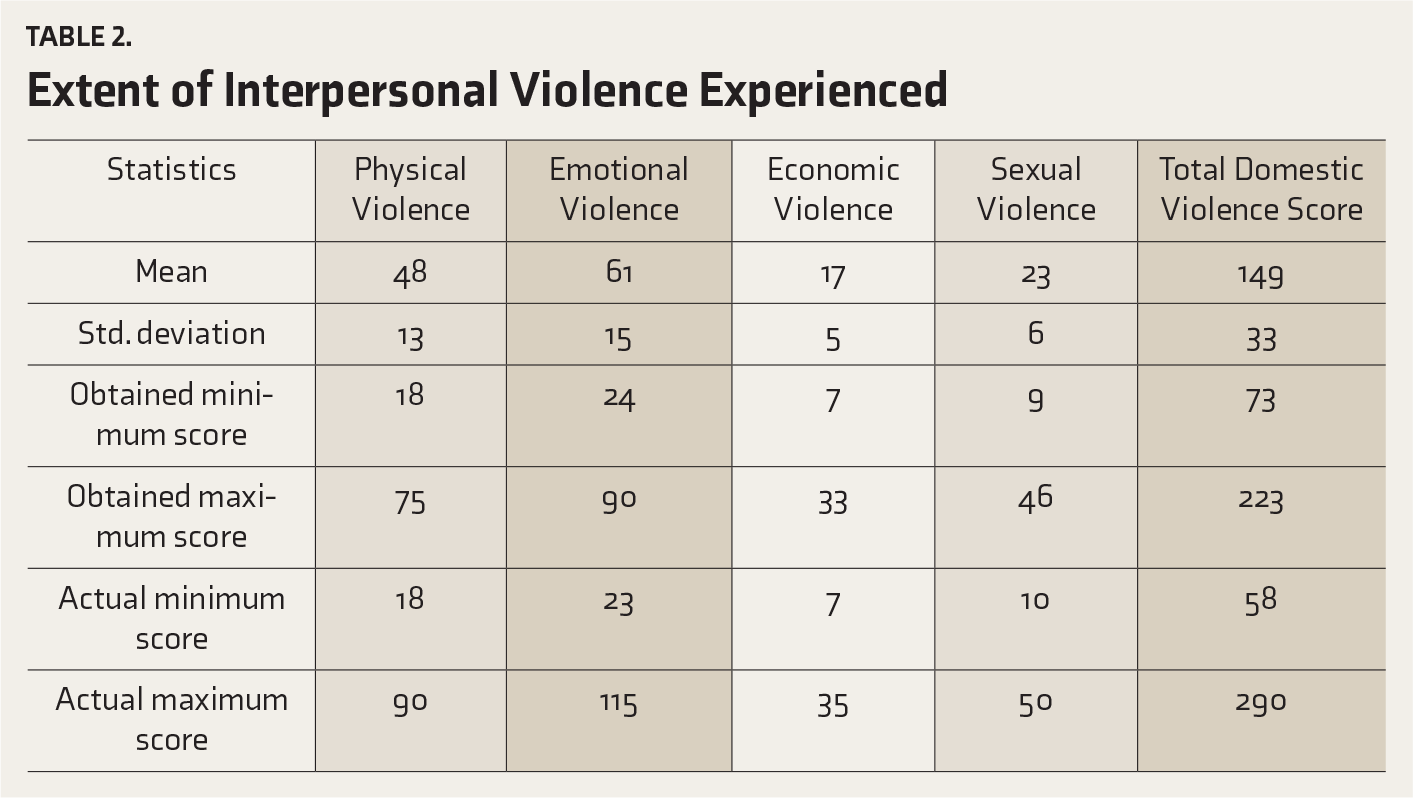
The mean scores and SD of domains of IPV Questionnaire revealed that all the women experienced moderate to severe levels of physical, emotional, economic, and sexual violence by their partners (
Extent of Interpersonal Violence Experienced
More than one-third (40%) had witnessed physical violence toward their mothers from their fathers in their childhood, which was reported to be traumatic in nature for the women. More than 58% had undergone physical abuse by their fathers during their childhood. A small proportion (9%) had undergone childhood sexual abuse, and the perpetrators were known family members. Half of the women with IPV reported that their children were subjected to violence by the perpetrator.
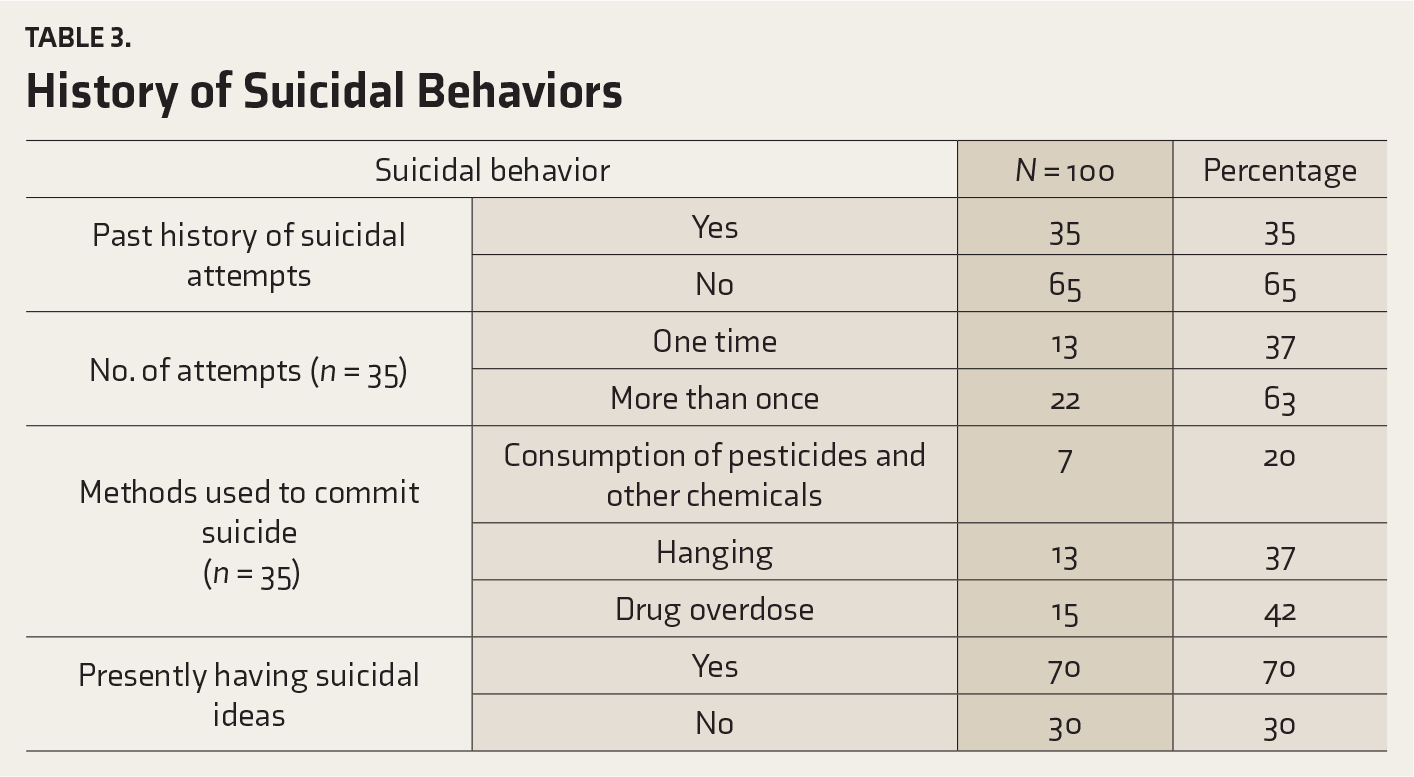
In the past, nearly half of the women (52%) had left the home and lived temporarily with their family members and then returned to their abusive partners. Thirty-one women attempted to leave an abusive relationship. Out of this, presently, 13 women were living separately, three were legally separated, and rest 15 women were temporarily living with family members. One-fourth of the women reported a past history of suicide attempts. Overall, 70% of the women reported to have suicidal ideas secondary to the ongoing IPV (
History of Suicidal Behaviors
Those women who reported IPV from perpetrators who consumed alcohol experienced significantly higher physical violence (P < 0.001), emotional violence (P < 0.001), and economic violence (P < 0.001) compared to those who reported IPV from perpetrators who were nonconsumers of alcohol. Those women with IPV who had attempted to leave the violent relationship in the past experienced significantly higher sexual violence (P < 0.001) compared to those women who made no attempts to leave the violent relationship in the past (
Relationship Between Background Variables and Severity of Interpersonal Violence
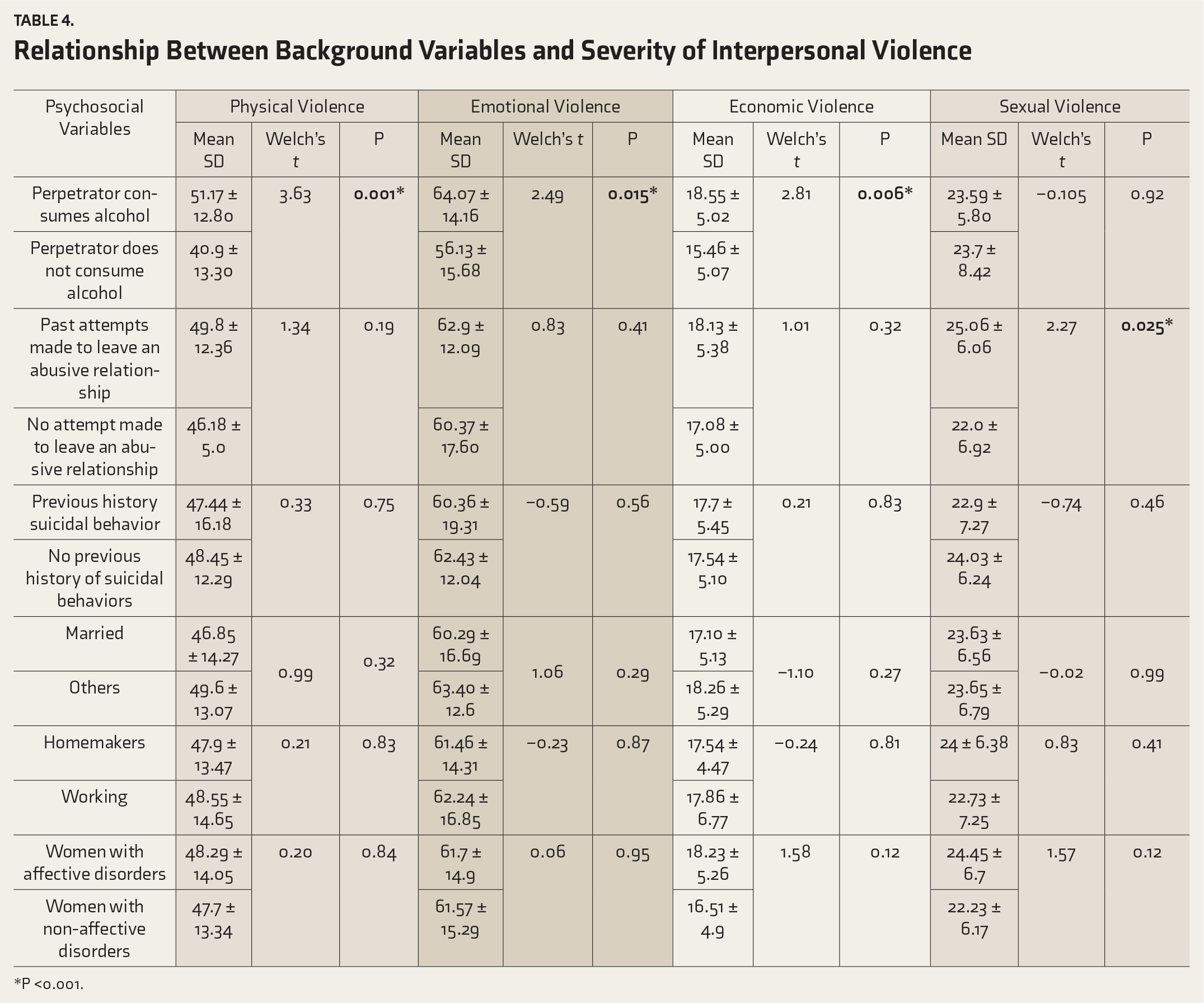
*P <0.001.
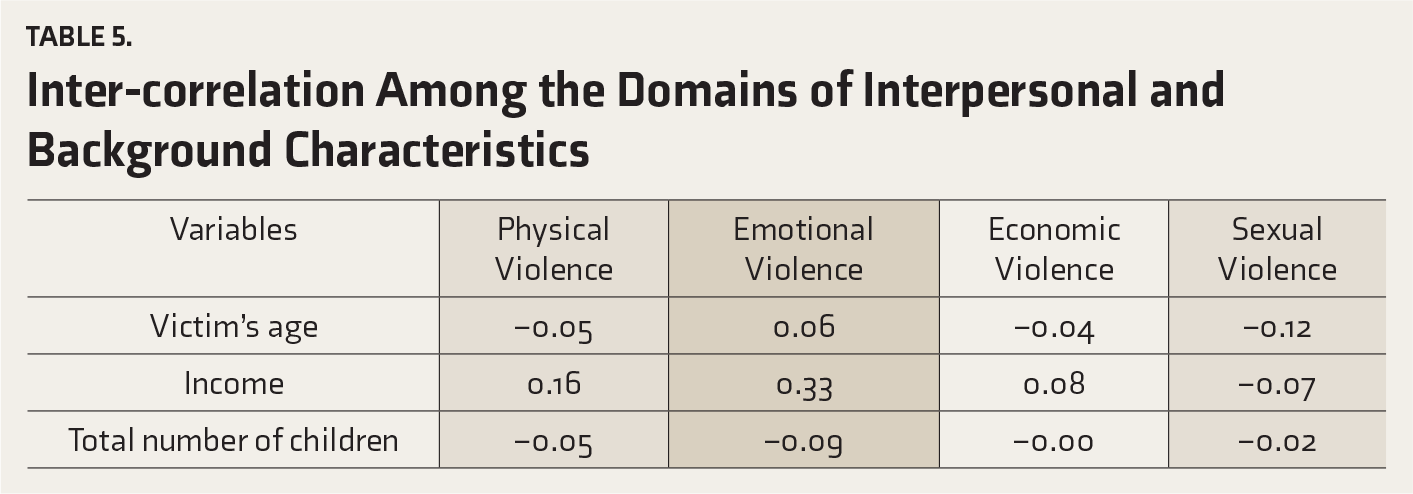
Inter-correlation Among the Domains of Interpersonal and Background Characteristics
About 90% of women with IPV wanted counseling services to overcome psychological distress secondary to violence, 40% each wanted stress management intervention, police aid, and treatment to abusive partner for alcohol problems. A total of 22% of women wanted shelter care facilities; a small percentage (10% each) expected family counseling services to prevent ongoing violence and teaching anger management skills to abusive partners from the Mental Health Professionals (MHPs).
The range of services expected from the MHPs varied from counselling services, police help, stress management, deaddiction treatment, and anger management skills for the abusive partner.
Discussion
This study aimed to assess the extent and severity of IPV, lifetime victimization, and services expected from MHPs at a tertiary care psychiatric hospital in India. Majority of the women experienced moderate IPV by their partners and known family members. Three-fourth of the women (83%) developed psychiatric illness after marriage, and IPV could have been one of the stress factors for developing mental illness secondary to ongoing violence. This finding is in concordance with recent findings that9,10 reported that women who have experienced domestic abuse have three times the risk of developing a mental illness, including severe conditions. A recent systematic review and meta-analysis of cohort studies on IPV against women and health outcomes revealed a positive association between IPV and subsequent depressive symptoms and increased symptoms of post-postpartum depression. There was also a bidirectional relationship between recent IPV and hard drug and marijuana use. 11
A few studies have reported that childhood exposure to family violence is associated with increased risk of IPV12,13 and a significant risk factor for further victimization and poor health outcomes in adulthood.14,15 In the current research, more than three-fourth of WMI had witnessed abuse of their mothers by their fathers and more than half had undergone physical abuse by their fathers in childhood. Bensley et al., 16 in a study conducted on 3,527 women, revealed that women reporting childhood physical abuse or witnessing interparental violence had a fourfold to sixfold increased risk of physical IPV, and threefold to fourfold increase in the risk of emotional abuse from partner.
Those WMI whose husbands use alcohol experienced significantly higher IPV than the WMI whose husbands did not use alcohol. Similarly, past research had found that the husband’s use of alcohol was one of the major factors for violence toward women.17–22
McFarlane et al., 23 in their community-based research, revealed that irrespective of service used, women who returned to the abuser reported higher danger and associated lethality risk compared to women who did not return. Additionally, the severity of physical abuse was significantly higher for women returning to the abuser who had been in a shelter but not for women who received a protection order. Further, leaving an intimate partner and estrangement from an intimate partner are risk factors for femicide among women victims. WHO 24 reported that women with a past history of attempts to leave the abusive relationships experienced higher sexual violence than those who made no such attempts. 25 According to our findings, women who returned to live with the abusive partners, after temporary separation, reported significantly higher danger of lethality compared to WMI who did not return to their abusive partners. Women who separated from their abusive partners after cohabitation experienced increased risk of femicide, particularly when the abuser was highly controlling. Other studies have revealed the same risks were posed by estrangement26,27 but ours further explicates the findings by identifying highly controlling male partners as presenting utmost danger in this situation.
Implications
In light of our findings, it is important to mandatorily screen all WMI in tertiary psychiatric care for IPV. Asking simplistic questions may not be a sufficient intervention on the part of a clinician, as evidence exists that victims of IPV minimize the extent of the abuse when it is disclosed to clinicians.28,29 Also, the key to safe and appropriate intervention is that women most likely to minimize the disclosure of violence may also be those who have experienced the most severe violence and those who have the most accepting attitudes toward violence. 30 The findings of a part of our larger research 31 revealed that at the patient level, many WMI undergoing IPV chose to conceal their abuse from MHPs, fearing retaliation from their partners if they get to know about the disclosure. At the professional level, lack of privacy was another important barrier for disclosure, where women reported that MHPs discussed the abuse in the presence of their violent partner. Hence, MHPs need to maintain privacy and confidentiality while doing an assessment. Safety planning with survivors should incorporate risk information that the clinician has gleaned from screening, and intake procedure suggests that incorporating risk assessments and safely planning of the predictions made by women regarding their safety can be extremely useful. In addition to planning for a woman’s physical safety, effective safety planning should always include an assessment of her mental state or psychological stability. In India, Vranda et al. 32 developed and standardized a comprehensive culturally appropriate guide, first of a kind, Psychosocial First Aid Intervention and Support for Women Survivors of Intimate Partner Violence/Domestic Violence—A Guide for Health Care Professionals based on research. It is a unique effort to equip health care providers with skills and guidance as to how to respond to IPV/domestic violence against women in clinical settings. From the clinical standpoint, large-scale, longitudinal, prospective studies are required to know about the mental health outcomes of the victims.
Limitations
The study was confined to one tertiary psychiatric hospital; hence, the generalizability of the result is limited.
Conclusion
Despite progress in legislation, policies, and programs, WMI are continuing to experience violence. The promotion of women’s mental health requires appropriate public and private recognition of the problem and preventive, proactive measures.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The study was financially supported by intramural NIMHANS funding (NIMH/Proj-VMN/00559/2016-17).