
Abstract
Background:
In India, mental health rehabilitation centers run income generation programs (IGP) for therapeutic engagement, skills training, and income generation of clients. The centers have evolved IGP models relevant to their settings. There is a paucity of published literature on practices employed by the centers.
Methods:
This paper compiles data gathered from visits to 13 centers between November 2018 and April 2019. Information was collected through observation and interviews with staff involved in IGP, using a semi-structured pro forma designed for study.
Results:
Most centers were based in south India (n = 11) and urban areas (n = 12). Each center ran two to seven IGP. Each center involved 20–50 clients in IGP. Clients involved in IGP were aged 20–60 years. The centers ran a range of IGP, including the manufacturing of household consumables, paper products, textile products, handicraft products, food products, and jute products; animal husbandry and horticulture initiatives; and running cafeterias and petty shops. IGP were mostly selected based on market demand and sales value of products (n = 11); ease of doing (n = 5); interests, abilities, exposure, and experience of clients (n = 5); and availability of resources (n = 3). Products were priced primarily to cover input and labor costs (n = 8), and many centers sold products below the market rates (n = 5). Running stalls during public events was a common strategy for the sale of products (n = 9). Personal contacts and “word of mouth” publicity were used for advertisement (n = 6). Four centers involved family members in IGP.
Conclusion:
The nature of IGP varied in terms of setting, available resources, and profile of clients availing the services. Marketing and sales were a challenge. A supportive framework of policies and schemes is essential to promote IGP at mental health rehabilitation centers. This report may be helpful for professionals and centers planning to set up an IGP.
Keywords
Indian mental health rehabilitation centers have identified relevant income generation programs as per available resources and client profile. In most centers, the primary goal was client involvement in the rehabilitation process, whereas income generation was secondary. This practice-based evidence can inform “indigenous” and “culture-sensitive” rehabilitation intervention.Key Messages:
Recent legislations have provided an impetus to cater to the unique rehabilitation needs of the clients. The Rights of Persons with Disabilities (RPWD) Act, 2016, recognizes 21 disabilities, including four psychiatric disabilities, namely intellectual disability, mental illness, autism spectrum disorder, and specific learning disability. 6 Mental Healthcare Act (MHCA), 2017, mandates that state governments make provisions for hospital- and community-based rehabilitation services and establishments in each district. 7 A recent order from the Honorable Supreme Court stressed the need for the development of rehabilitation facilities for long-stay patients in government mental hospitals. 8 These developments are expected to pave the way for more centers across the country, especially in the government sector, to serve people who cannot afford “paid” services.
Multiple studies have documented that in India, vocational rehabilitation is an important felt need of clients and their caregivers.9–11 To address this need, centers facilitate skills training, supported employment, self-employment, and home-based work programs. 12 Vocational rehabilitation services commonly consist of income generation programs (IGP). For this study, IGP was operationally defined as “any activities done for productive engagement or skills training, which result in the manufacturing of products suitable for sale.” The centers run IGP in their daycare settings or as a part of vocational training units. The revenue generated from IGP helps centers sustain the vocational unit and offer monetary incentives to the clients involved. 13 Such incentives also help clients support their families or buy medicines. 14
There are several challenges in running an IGP, including identification of a suitable program, the financial viability and sustainability, hiring staff, training clients, marketing, and accounting. 15 Each center has addressed these challenges and evolved IGP practices relevant to their setting. There is a paucity of published literature on models employed by Indian centers. 16 The experience of centers can serve as “indigenous,” “culture-sensitive,” and “practice-based evidence” rehabilitation interventions.17, 18 In this context, the present study was planned to document models of IGP practiced by Indian mental health rehabilitation centers.
Materials and Methods
Fifteen centers were selected based on proximity, convenience, and consent to participate. Details of the research study were shared with the centers, and permission was sought to collect details through a field visit. The centers were explicitly informed that the data collected would be anonymized and not individually identified. Two centers permitted the researcher’s field visit but declined permission to document the data for publication.
This paper compiles the data gathered from visits to 13 centers between November 2018 and April 2019. A field visit to each center lasted 2–3 days. A semi-structured pro forma was designed by the authors’ consensus to collect details of IGP practiced by the centers but was not validated (Appendix S1). Information was collected through observation and interviews with IGP supervisors, trainers, or in-charges. Clients were not interviewed as part of the visit. The respective centers reviewed the reports of the visit, and approval was sought for publication.
This paper is an outcome of a PhD research study—approved by the Institute Ethics Committee—whose objectives included identifying and integrating models of IGP for clients and describing operational and financial feasibility as well as stakeholder experiences in an IGP implemented in a tertiary care center. This paper focuses on the first objective and presents results about the centers, IGP, staffing, and challenges.
Results
The profiles of the 13 centers and the types and details of IGP are described in
Profile of Mental Health Rehabilitation Centers
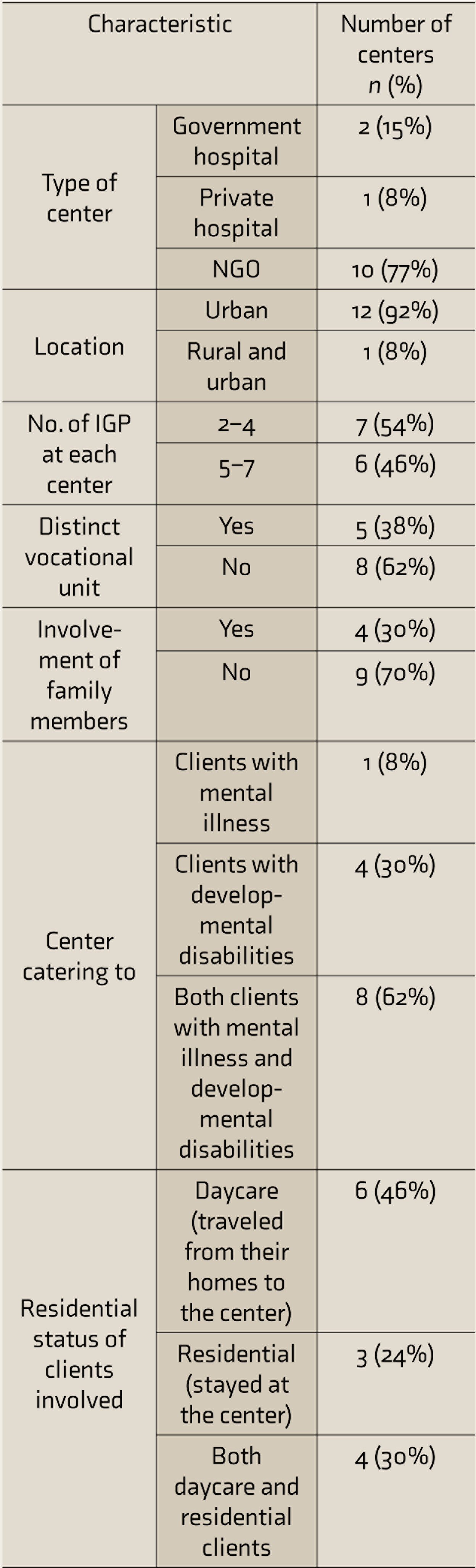
IGP: income generation program, NGO: non-governmental organization.
Compilation of IGP Practiced at Various Centers
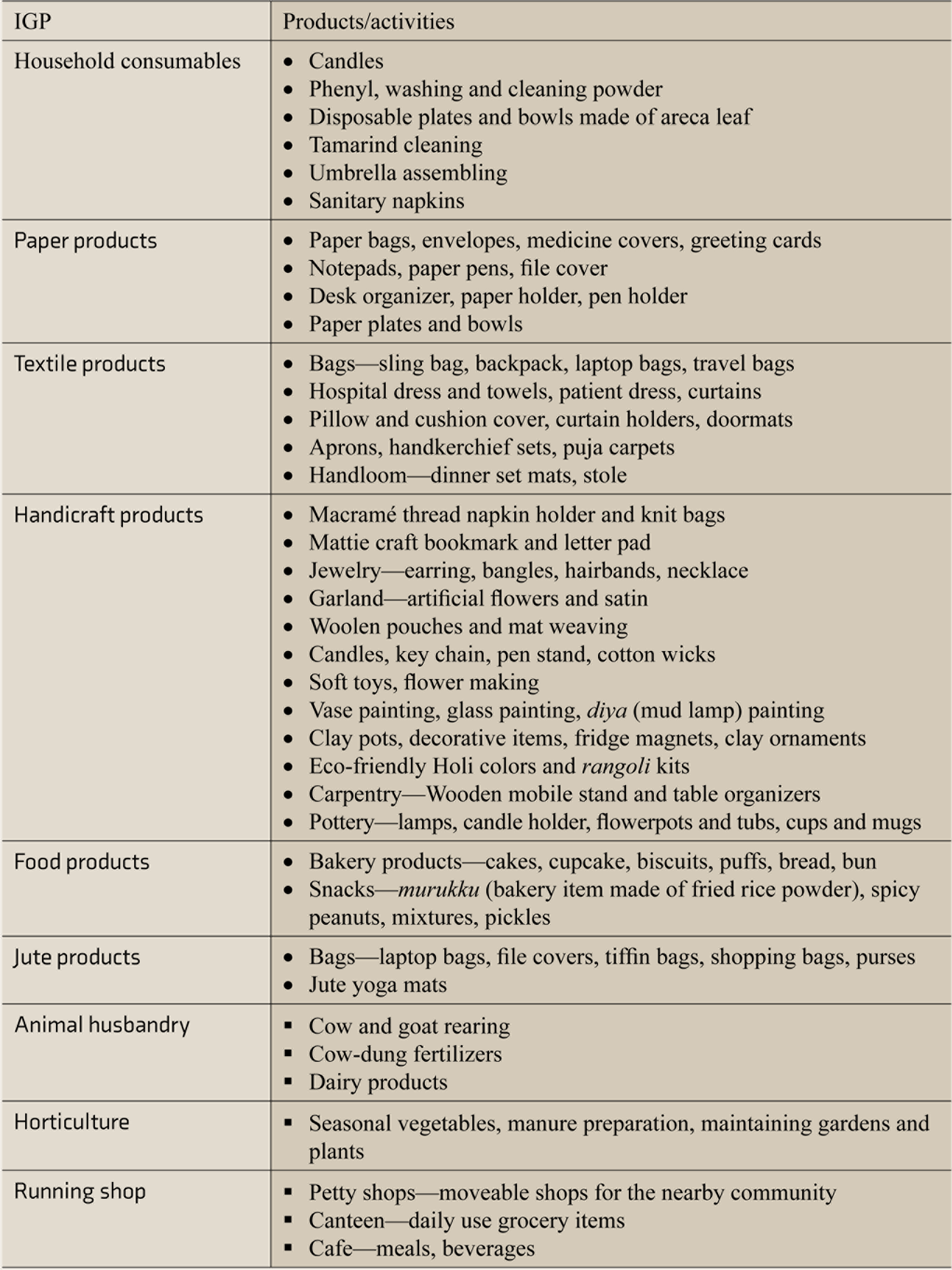
IGP: income generation program.
Multiple Response Table of Findings Related to IGP
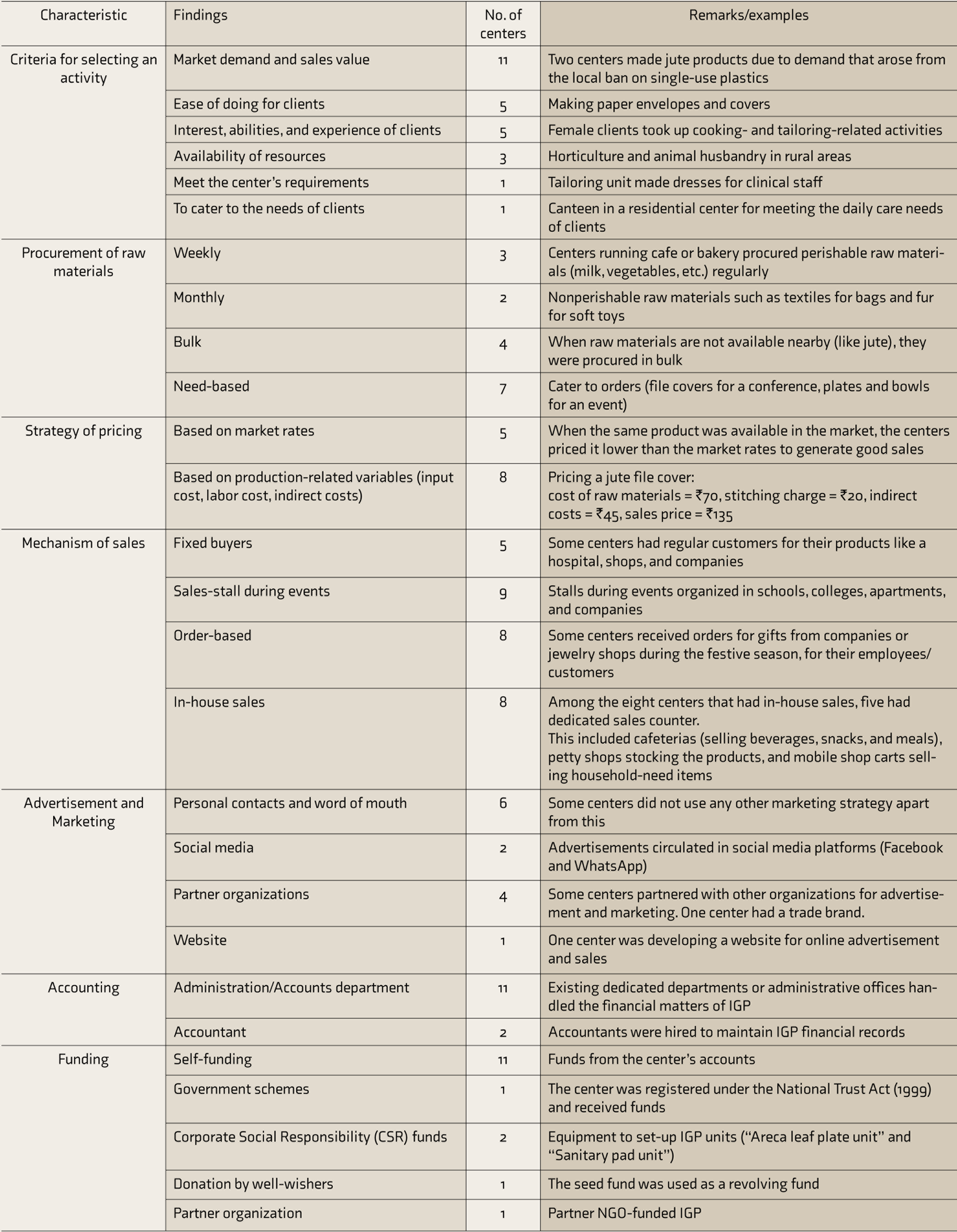
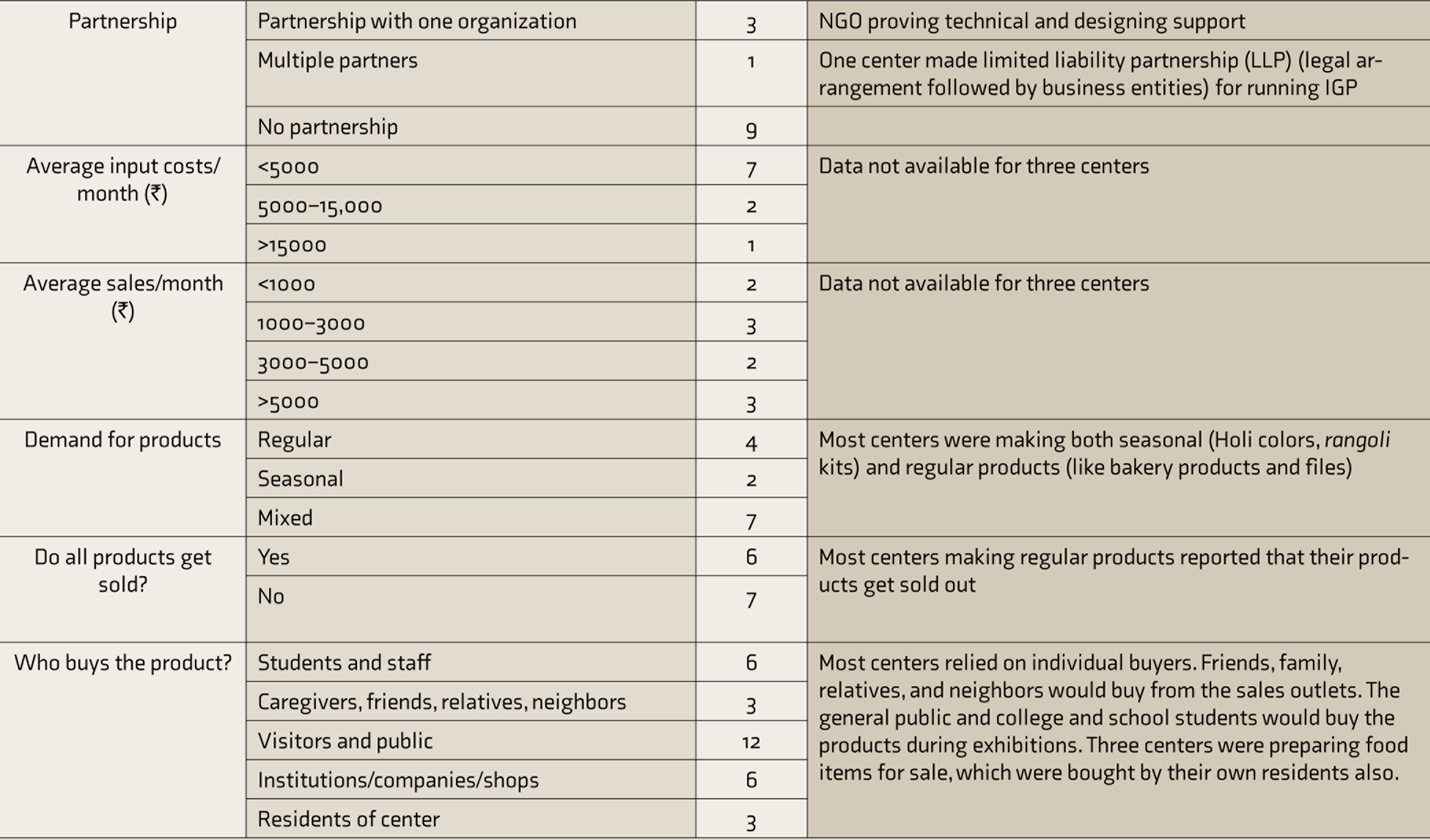
IGP: income generation program; NGO: non-governmental organization.
Eleven centers were from the south Indian states of Karnataka, Tamil Nadu, and Kerala. Most centers were urban-based (n = 12) and in the NGO sector (n = 10). Most centers catered to both persons with mental illness and persons with developmental disabilities (n = 8). Each center ran two to seven IGP. Each center involved 20–50 clients in IGP. The age range of clients involved was 20–60 years. Five centers ran distinct units aimed at providing vocation-based skills training or transitional employment opportunities or facilitating income generation for clients. Four centers involved family members (primarily mothers). Some of them were employed as trainers or supervisors. Many of them took part in the activities done by their wards, whereas the others assisted the trainers in training or monitoring a group of clients (
Content analysis was used for compiling the IGP practiced at the various centers. Categories were created through an interpretive process by using constant comparison and sorting. All centers were involved in a diverse range of activities, which are grouped under the following categories—the manufacture of household consumables, paper products, textile products, handicraft products, food products, or jute products; animal husbandry and horticulture; and running shops (Table 2).
For analyzing the practices related to IGP, distinctive meaning units were delineated, and data were organized using the interview questions as domains. IGP were mostly selected based on market demand and sales value of products (n = 11); ease of doing (n = 5); interests, abilities, exposure, and experience of clients (n = 5); and availability of resources (n = 3). For example, a rural center had adopted animal husbandry, dairy, and horticulture. One center made files that were supplied to a nearby hospital. Another center made saplings that were gifted to dignitaries in their organization. Nonsustainable IGP was discontinued. For example, one center had stopped candle-making unit due to poor sales. Some IGP such as paper-cover making were time-consuming and did not generate revenues commensurate to efforts but were continued as they were inexpensive to sustain, were easy to do, and engaged clients with limited functioning. Centers involved clients in different IGP or various steps of the same IGP, based on their functioning. For example, the higher functioning clients were involved in stitching clothes, whereas the other clients were involved in folding the clothes.
Most centers funded IGP from their funds (n = 11). Running stalls during public events was a common strategy for facilitating sales of products (n = 9). Personal contacts and “word of mouth” publicity were the commonly used advertisement strategies (n = 6). Most centers (n = 7) made both seasonal and regular sales products. Most centers reported that all products did not get sold out (n =7). As per the data available for ten centers, seven centers spent <₹5000 per month for input costs and generated sales of <₹5000 per month. Products were priced primarily to cover input and labor costs (n = 8), and many centers sold products below the market rates (n = 5), to boost sales. The centers reported that the public, visitors, family members, neighbors, and students bought the products as a gesture of goodwill. Sales income was used to sustain IGP (buy raw materials) and offer some incentives to clients. Practices related to IGP are summarized in a multiple response table (
In government-run academic centers, the faculty members oversaw the vocational/skills training unit. In the NGO sector, IGP was governed by the management (board members or administrative departments). Progress of clients was monitored by social workers, psychologists, nurses, and psychiatrists (depending on availability). Two centers hired placement officers for facilitating supported employment/self-employment opportunities. Vocational trainers and supervisors were involved in training the clients in vocational skills. Qualifications of the vocational trainers varied across centers and even in the same center. In the majority of centers (n = 10), the minimum qualification of vocational trainers was secondary or senior secondary schooling, whereas at other centers, it was a certificate course in specific vocational skills, graduation, or diploma. Each vocational trainer, on average, supervised 5–25 clients (
Details Related to Staff Involved in IGP
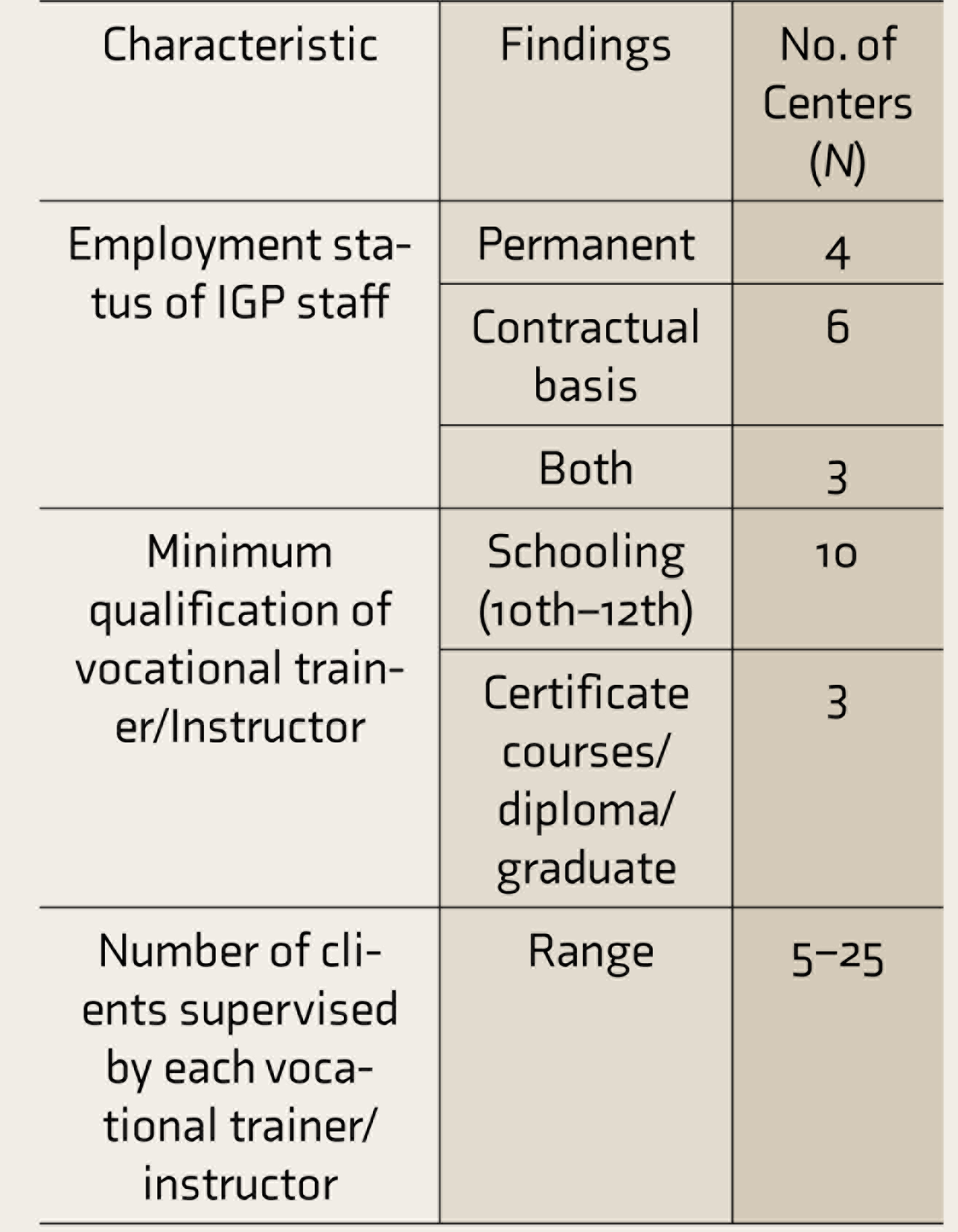
IGP: income generation program.
The vocational trainers were involved across the IGP phases such as doing market surveys for finding cost-effective sources of raw-materials, preparing work orders and estimating finances, procuring raw materials, training clients, monitoring product quality, maintaining stocks, taking and coordinating orders, shifting products for sales events, tallying sales, keeping records of clients’ involvement, and at some centers, even marketing and liaison. The staff members reported the following challenges about IGP: lack of funding, space constraints, changing market demands, limited sales and profits, unsold products, difficulty in the transportation of products for sales, lack of marketing expertise, handling finances, and laborious accounting and record keeping.
Discussion
The centers offered a menu of IGP from which the clients could choose. Clients were involved in tasks according to their functioning level. With experience, the centers had identified IGP that could be continued with available resources. The centers sold the products through their own sales outlet, stalls at exhibition sales, and patrons in the locality who bought out of goodwill. The products showcased the ability of clients among visitors and the public.
The revenue generated is meager. Most centers had a monthly sale of <₹5000. Most centers reported that they faced the challenge of unsold stocks. This can be attributed to multiple reasons: doubts about the quality of products made by the clients, perception of “pity purchase,” lack of unique products, competition with companies who make cheaper and better products, difficulty in catering to bulk orders at short notice, doubts if trainer or clients make the product, and limited marketing opportunities. 15 Five centers priced the products lower than the market rates to liquidate the old stocks and keep the vocational units active. Marketing of the products is a challenge for many centers who cannot afford to employ staff exclusively for this purpose. So, many centers rely on personal contacts. Active collaboration is required between stakeholders at various levels. 12 The centers need to focus on product innovation, quality, and pricing. Joint ventures with businesses can offer a professional understanding of the supply chain and available market to run sustainable IGP. 19 Sales partnerships with local retail chains and e-commerce platforms are the future directions to be explored.
A fundamental dilemma before the centers is to choose between “profitable” IGP (focused on generating higher profits) versus “therapeutic” IGP (focused at contributing to the clients’ recovery). A “profitable” IGP can be run as workshops with the efficiency of a business enterprise. Five centers ran distinct vocational units. The set-up needs to be well-equipped and adequately staffed. The enterprise needs to utilize highly efficient clients to make products in demand, do liaison with customers, and fulfill orders as per promised time. In contrast, a “therapeutic” IGP is run in daycare centers. The aim is to gainfully engage clients in activity scheduling and offer skills training. Involvement in IGP can also facilitate social interaction, expand the repertoire of activities, and offer a sense of purpose, which helps in the rehabilitation process. Some clients may start with “therapeutic” IGP and graduate to “profitable” IGP over time, but this transition may not be possible for all clients, especially those with severe challenges. In the present study, we observed that the philosophy of the centers was to offer a “therapeutic” IGP that also generated some revenue. In other words, the goal of IGP was to facilitate the rehabilitation process, and income generation was a by-product.
Families need to play a proactive role in deciding services/facilities to be developed for the empowerment of clients. 20 Family caregivers (predominantly mothers) were actively involved in IGP at four centers. Many of them were also employed as vocational trainers. Family caregivers gained the required skills on the job. 17 It was a mutually beneficial arrangement for the centers and the families. The centers benefited from a pool of people who were sensitive to the needs of the clients. Such family-caregivers-cum-staff were in a better position to liaise with other families. The employment helped the families financially. It could also pave the way for some families to consider self-employment ventures or home-based IGP in the future.
The centers deliver services through multidisciplinary teams that vary in composition, organization, setting, ideology, and procedures. 21 To run an IGP, the vocational trainers worked as a team with clients, family caregivers, other staff, and mental health professionals. The vocational trainers multitasked and shared responsibilities as per the situation. Many vocational trainers were employed in contractual jobs at lower pay scales than permanent jobs. At many centers, especially in residential centers, the researcher observed that staff members and clients worked in close coordination. They enjoyed their meals together and took care of each other. A similar finding has been observed in a western study, which reported that many rehabilitation staff worked for intrinsic rewards (interesting/challenging work and opportunity to help clients) rather than extrinsic rewards (pay and benefits). 22
Ten centers had recruited vocational trainers who have completed schooling, and only a few were graduates. The situation is similar even in developed countries. A study from the USA reported that one-third of psychosocial rehabilitation workers (who were not in supervisory or administrative positions) did not have college degrees. 23 During data collection, the researcher observed that across the centers, the vocational trainers had several essential core competencies of psychosocial rehabilitation. This was reflected in the way the trainers treated the clients with dignity, involved the family caregivers in service planning and delivery, utilized community resources, displayed cultural competence, and worked collaboratively within and across the system. Experts have remarked that while many competencies can be evolved on-job, certain core competencies like “interpersonal skills” and “problem-solving abilities” are innate and difficult to develop.24, 25 In this context, it appears that the centers had recruited staff with good interpersonal skills and an aptitude to work with clients, while educational qualification was secondary.
In comparison to the government-funded centers, NGO-run centers are constrained for funds. The centers registered under National Trust can avail funds for running daycare centers (Vikas scheme) and for marketing (Prerna scheme). 26 As per the mandate of the National Trust, such a center can cater only to persons with a primary diagnosis of mental retardation, autism, cerebral palsy, or multiple disabilities. Apart from the recently introduced “Deendayal Disabled Rehabilitation Scheme (DDRS)” to set up half-way homes for the rehabilitation of long-stay patients of state mental hospitals, 27 there are no government schemes to fund rehabilitation programs for persons with mental illness. It is a financial tight rope walk for the centers to offer the services. Many NGO-run centers generate funds from the fees collected from the clients for availing the services, individual donations, and other funding agencies. The funds generated are used to pay the staff, bear the infrastructure costs, and sustain the services. The funding scenario influences the pay scale for the staff, the number of permanent staff (who get higher pay than contractual staff), and fresh investments in IGP. The fact that the centers have survived and are thriving despite odds is a testament to the strong leadership of the organizations.
To expand the centers across the country, more government funding is required. In the present study, no centers were availing funding under “Skill India” and other flagship programs of the Government of India. Supportive government policies are needed. For example, the government can offer incentives to corporates/government agencies for placing bulk orders from organizations working for the empowerment for persons with disabilities. Such affirmative action by the government will help the centers expand IGP.
Limitations
As the centers were selected based on proximity, most were in South India. Information was gathered by visiting the centers and was not cross-verified. The report does not include the perspectives of clients and family caregivers.
Conclusion
The present study documents IGP models followed by 13 Indian centers. The nature of IGP varied as per setting, available resources, and profile of clients availing the services. Marketing and sales were a challenge. A supportive framework of policies and schemes is essential to promote IGP at rehabilitation centers. This report may be helpful for professionals and centers planning to set-up an IGP.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for Income Generation Programs for Persons with Mental Health Challenges: Practices from 13 Indian Mental Health Rehabilitation Centers by Amrita Roy, Deepak Jayarajan, Thanapal Sivakumar, in Indian Journal of Psychological Medicine
Footnotes
Acknowledgements
The authors would like to thank following centers for permitting to visit and publish findings: Amogh (Bengaluru); Government Medical College & Hospital (Chandigarh); Hombelaku (Manipal); Institute of Mental Health and Neuro Sciences (Calicut); Manas Rehabilitation Centre (The Society for Mental Health, Kerala) (Calicut); MS Chellamuthu Trust & Research Foundation (Madurai); Richmond Fellowship Society (I), (Bangalore branch); Richmond Fellowship Society (I), (Lucknow branch); Schizophrenia Research Foundation (Chennai); Seva In Action (Bengaluru); Spastic Society of Karnataka (Bengaluru); The Association for the Mentally Challenged (Bengaluru); The Banyan (Centre for Emergency care & Recovery) (Chennai).
The authors would also like to thank Dr Jagadisha Thirthalli (Professor of Psychiatry & Head (I/C), Psychiatric Rehabilitation Services, NIMHANS), Dr Thomas Kishore (Additional Professor, Department of Clinical Psychology, NIMHANS), and Dr Kalyanasundaram (Honorary advisor, Richmond Fellowship Society [India], Bangalore branch) for reviewing the initial draft and offering valuable suggestions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AR was funded by the Indian Council of Medical Research (ICMR) fellowship and Psychiatric Rehabilitation Services (NIMHANS) corpus funds.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.