
Abstract
Background:
The coronavirus disease 2019 (COVID-19) pandemic has caused great financial and psychological havoc. Healthcare professionals (HCPs) are among the many groups of people who are in the frontline and facing a risk of direct exposure to the virus. This study aimed to assess the prevalence and predictors of stress, depressive, and anxiety symptoms among HCPs of India.
Methods:
It was a cross-sectional, online survey conducted in April 2020 among HCPs who are directly involved in the triage, screening, diagnosing, and treatment of COVID-19 patients and suspects. Stress was estimated using Cohen’s perceived stress scale. Depression and anxiety were assessed using the tools Public Health Questionnaire—9 and Generalized Anxiety Disorder—7. Predictors were analyzed using univariate and multivariate binary logistic regression.
Results:
A total of 433 online responses were obtained, and N = 350 were finally included. The prevalence (95% CI) of HCPs with high-level stress was 3.7% (2.2, 6.2), while the prevalence rates of HCPs with depressive symptoms requiring treatment and anxiety symptoms requiring further evaluation were 11.4% (8.3, 15.2) and 17.7% (13.9, 22.1), respectively. Women had approximately two times the increased odds of developing moderate- or high-level stress, depressive symptoms requiring treatment, and anxiety symptoms requiring further evaluation. Similarly, women staying in a hostel/temporary accommodation had two times the increased odds of developing depression or anxiety symptoms.
Conclusion:
The prevalence of stress, depressive, and anxiety symptoms among HCPs in India during the pandemic is comparable with other countries.
COVID-19 pandemic puts frontline HCPs at great risk of psychological stress. The prevalence values of high-level stress, depressive symptoms requiring treatment, and anxiety symptoms requiring further evaluation were 3.7%, 11.4%, and 17.7%, respectively; these values are comparable to other countries and not high, given the comparatively poor health infrastructure in our country compared to other nations. This could be attributed to the early phase of the pandemic and the resilience of Indian HCPs.Key Messages:
As on April 11, 2020, India faces the most critical phase of the pandemic, with community transmission not yet in full flow. 7 HCPs across the country are facing a fight like never before. Vulnerable to psychological impact, we aim to evaluate the magnitude of stress, anxiety, and depression and to assess possible associated risk factors at this early stage of the pandemic. This would help us plan appropriate interventions at the early stage to prevent a detrimental outcome for the brave HCPs out there.
Materials and Methods
Ethics
The study was approved by the institutional ethics committee. An online written informed consent was obtained from all potential participants.
Study Design and Eligibility Criteria
This was an online-questionnaire-based cross-sectional study conducted in India during the month of April 2020.The online questionnaire was designed on Google Forms and circulated in multiple WhatsApp groups, targeting doctors and nurses involved in triage, screening, diagnosing, and treatment of COVID-19 patients and suspects. Those who were currently doing their internship were excluded.
Study Procedures
The link to the online questionnaire was circulated on April 10, 2020, and the target sample size was achieved on April 25, 2020. A maximum of three reminders were sent in all WhatsApp groups. To limit the number of HCPs who inadvertently answer the questionnaire without being involved in COVD-19 work, a specific yes/no question confirming their work in COVID-19 was asked. Those who marked the answer as “Yes” were allowed to continue answering the questionnaire. The questionnaire had five sections, namely, baseline sociodemographic characteristics, Generalized Anxiety Disorder 7-item (GAD-7), Patient Health Questionnaire-9 (PHQ-9), Perceived Stress Scale-10 (PSS-10), and miscellaneous psychosocial questions. Data were collected anonymously, with only one response was permitted per person.
PHQ-9 is a 9-item self-report questionnaire used in clinical practice for screening, diagnosing, monitoring, and measuring the severity of depression. PHQ scores ≥10 have a sensitivity of 88% and a specificity of 88% for major depression and require treatment. 8 PSS-10 is an instrument designed to measure the degree to which situations in one’s life are appraised as stressful. PSS items have been found to have good correlations with other stress measures, self-reported health and health service measures, health behavior measures, smoking status, and help-seeking behavior. 9 GAD-7 is a 7-item self-report questionnaire used in clinical practice for screening and assessing severity of generalized anxiety disorder. Cut-off points of 5, 10, and 15 may be interpreted as representing mild, moderate, and severe levels of anxiety on the GAD-7. A score of >10 would require further evaluation. 10
Sample Size Estimation
Considering an estimated prevalence of depression (p) among HCPs to be 13.5% based on the study by Zhu et al., 11 the sample size estimated using the formula (Zα) 2 pq/d 2 using an alpha error of 5% and an absolute precision (d) of 5% was 179. If estimated considering the prevalence of stress (p = 29.8%), although a different tool being used, and anxiety (p = 24.1%), the sample size, with the other assumptions remaining constant, would be 322 and 281, respectively. Considering the largest value among the three and assuming an approximate 10% of questionnaires to have incomplete responses, we decided to increase the sample size to 350.
Data Management
Data were exported from the Google Forms to Microsoft Excel (Microsoft Corporation, Redmond, Washington, USA, 2016) spreadsheet and coded. Statistical analyses were performed using Statistical Package for Social Sciences (SPSS) Statistics for Windows, Version 20.0 (IBM Corp., USA, 2011).
Statistical Analysis Plan
Demographic characteristics were summarized using descriptive statistics such as frequency and percentages in case of discrete data, or mean and standard deviation (SD) in the case of continuous data. Prevalence rates of high-level stress, anxiety symptoms requiring further evaluation, and depressive symptoms requiring treatment were expressed as proportions with 95% confidence intervals (CI). The hypothesized factors/predictors to each of these conditions, namely stress, anxiety, and depression, such as age, gender, being a doctor, years of experience, hostel/ temporary accommodation, history of mental illness, presence of comorbidities, perceived inability to distress, and employment in the government sector, were subjected to univariate binary logistic regression. Those with a significance of P < 0.2 in the univariate analysis were included in the multivariate binary logistic regression model.
Results
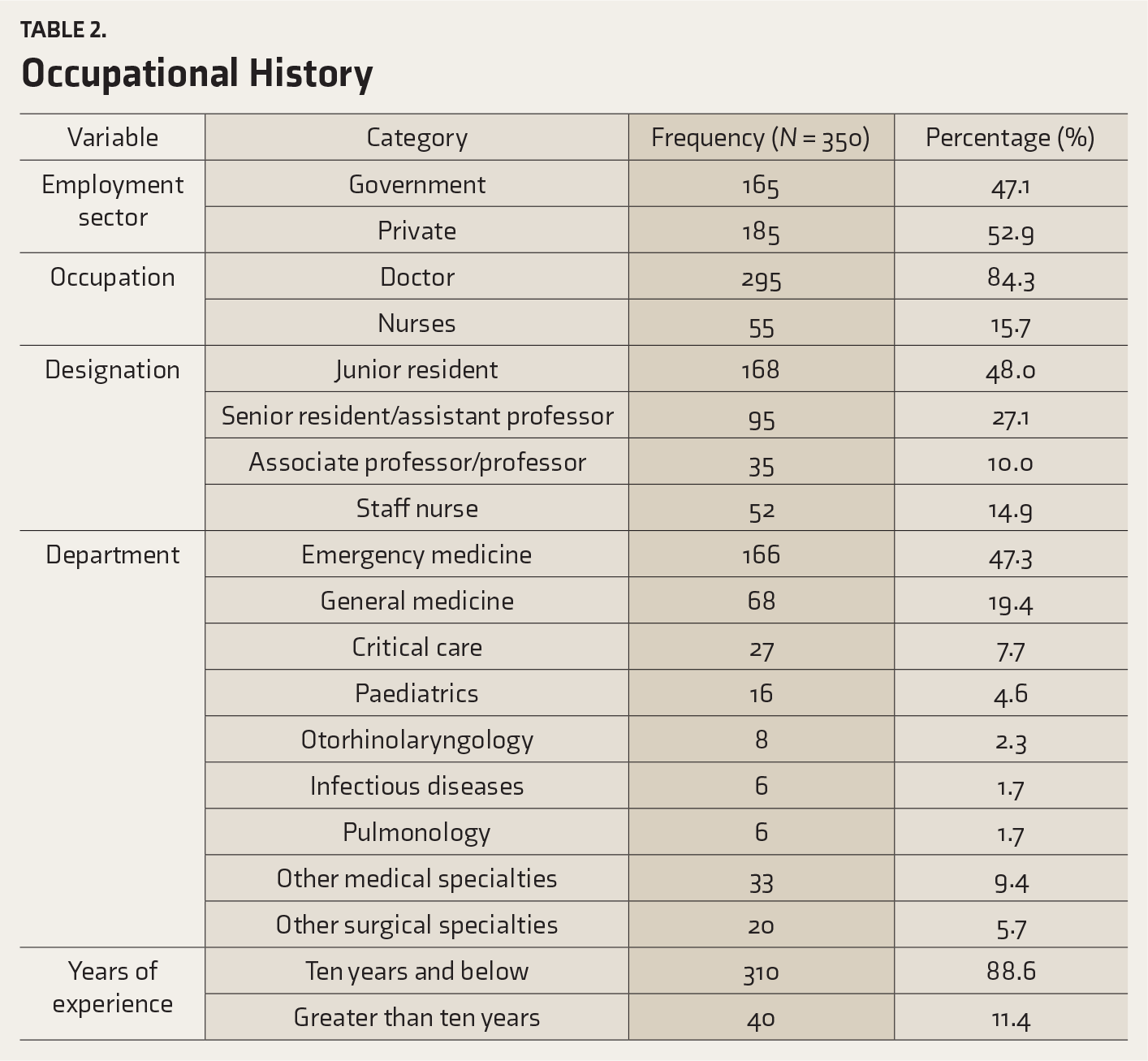
A total of 433 responses were received. Of these, 83 respondents were not involved in any of the COVID-19 related activities and hence were excluded. The remaining 350 from across ten states and one union territory were included in the analysis. A total of 344 participants had disclosed their institutions of affiliation, and the number of participating institutions totaled to 98. Of the 350 participants, 84.3% (n = 295/350) were doctors and the remaining 15.7% (n = 55/350) were nurses. The mean (SD) age of the participants was 30.21 (5.22) years. The demographic characteristics are summarized in Table 1.
Demographic Characteristics
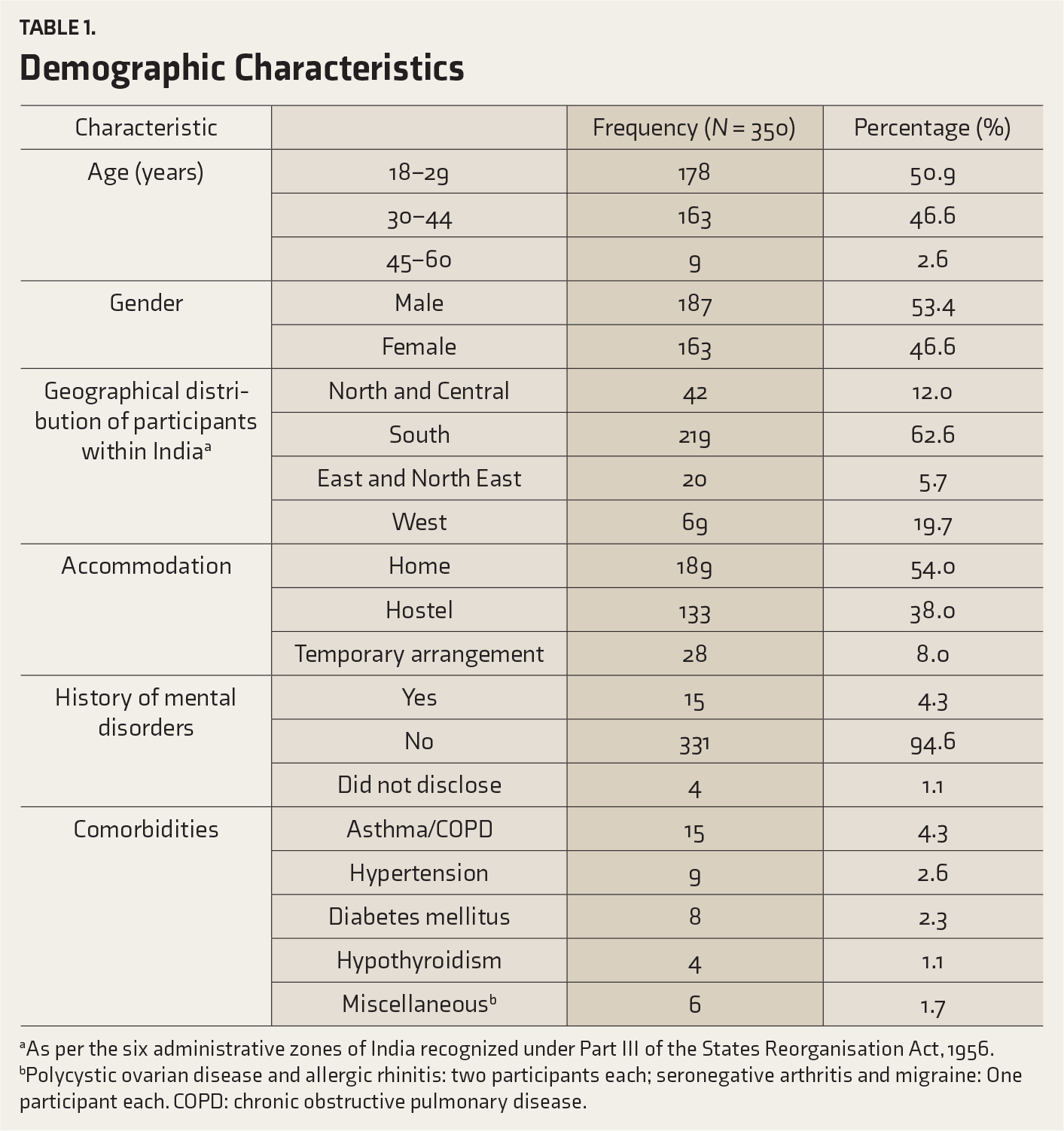
aAs per the six administrative zones of India recognized under Part III of the States Reorganisation Act, 1956.
bPolycystic ovarian disease and allergic rhinitis: two participants each; seronegative arthritis and migraine: One participant each. COPD: chronic obstructive pulmonary disease.
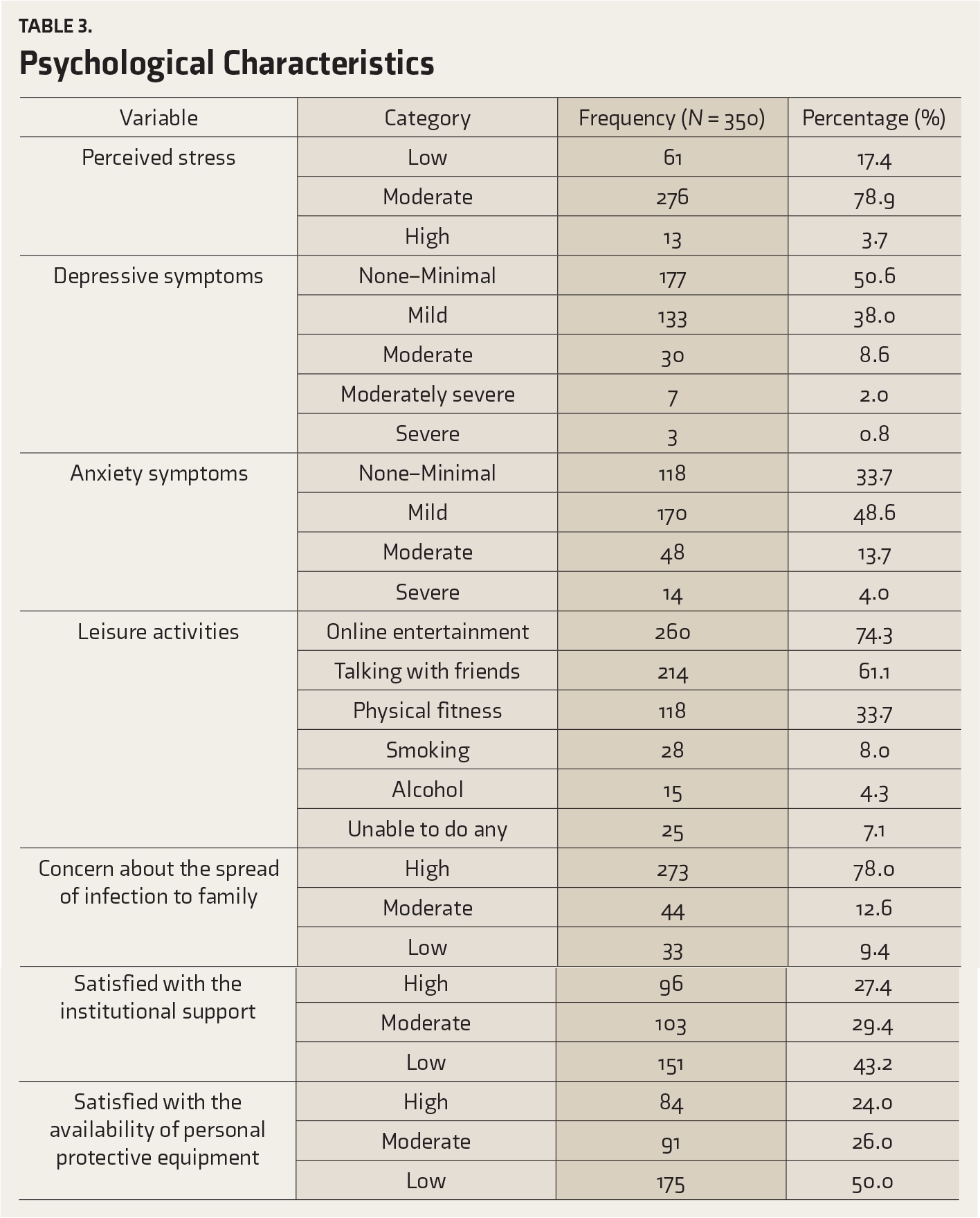
The prevalence (95% CI) of HCPs with high-level stress was 3.7% (2.2, 6.2). The prevalence rates (95% CI) of HCPs with depressive symptoms requiring treatment and anxiety symptoms requiring further evaluation were 11.4% (8.3, 15.2) and 17.7% (13.9, 22.1), respectively. The details of various categories of stress, depressive symptoms, and anxiety symptoms, and the details of leisure activities are depicted in Table 3. A large majority (n = 273/350; 78.0% had serious concerns about the spread of infection from them to their friends or family members. Also, most participants (n = 151/350; 43.2% and n = 175/350; 50.0%, respectively) were not satisfied with the administrative support from the institution and the availability of personal protective equipment.
An analysis to identify the predictors of moderate- and high-level stress revealed that female gender (odds ratio [OR] = 2.008, 95% CI = 1.122, 3.594, and P value = 0.019) was the only significant predictor among all the hypothesized factors, thereby negating the need for multivariate analysis. With regards to depressive symptoms requiring treatment, the significant predictors (adjusted OR; 95% CI; P value) were female gender (2.023; 1.021, 4.010; 0.044) and hostel/temporary accommodation (2.355; 1.180, 4.702; 0.015). Similarly, the significant predictors (adjusted OR; 95% CI; P value) of anxiety symptoms requiring further evaluation were female gender (2.180; 1.230, 3.862; 0.008) and hostel/temporary accommodation (1.926; 1.046, 3.548; 0.035). The details of the univariate analysis and multivariate analysis to identify the predictors of stress, depression, and anxiety are summarized in Table 4.
Discussion
Occupational History
Psychological Characteristics
Univariate Analysis for Predictors of Stress, Depression, and Anxiety
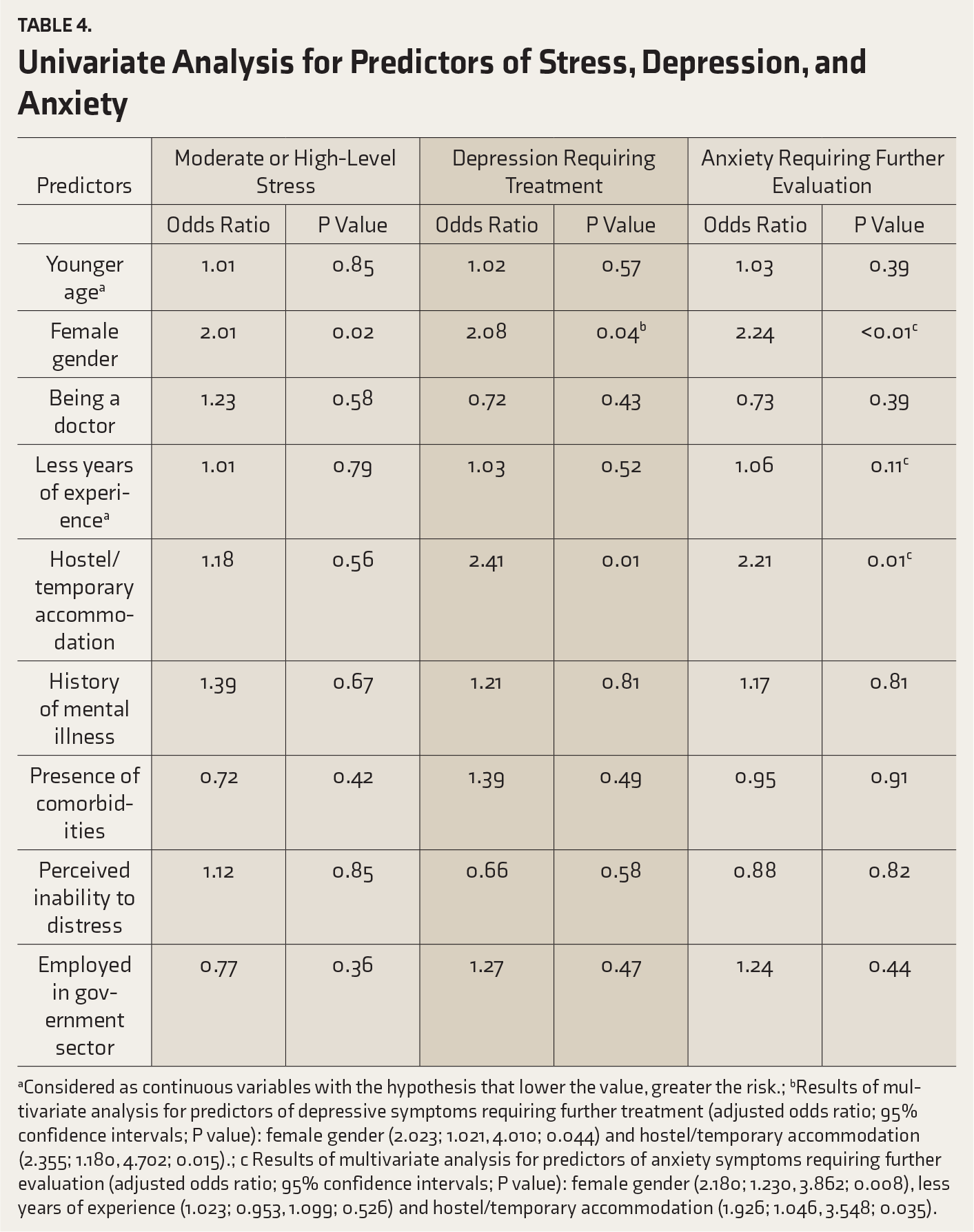
aConsidered as continuous variables with the hypothesis that lower the value, greater the risk.; bResults of multivariate analysis for predictors of depressive symptoms requiring further treatment (adjusted odds ratio; 95% confidence intervals; P value): female gender (2.023; 1.021, 4.010; 0.044) and hostel/temporary accommodation (2.355; 1.180, 4.702; 0.015).; c Results of multivariate analysis for predictors of anxiety symptoms requiring further evaluation (adjusted odds ratio; 95% confidence intervals; P value): female gender (2.180; 1.230, 3.862; 0.008), less years of experience (1.023; 0.953, 1.099; 0.526) and hostel/temporary accommodation (1.926; 1.046, 3.548; 0.035).
Our study has a few limitations. By virtue of its design that it is an online questionnaire without face-to-face interviews, it is difficult to pin a clinical diagnosis on participants who exhibited symptoms. The actual prevalence rates of clinically diagnosed psychological issues studied may vary, although validated screening tools have been used in this study. Also, self-selection bias is a possibility. Further, not all cadres of HCPs other than nurses and doctors have participated in the study. Yet another limitation is that India being a large country in area, the burden of patients diagnosed with COVID-19 is varied, with metros facing the brunt of the pandemic rather than the interiors. Thus, the findings may not be truly reflective of the entire nation during the time of this study. Having said that, the main strength of this study is that the psychological impact has been assessed while the trigger event is actually still ongoing and the threat is still looming.
Conclusion
The prevalence rates of high-level stress, depressive symptoms requiring treatment, and anxiety symptoms requiring further evaluation were 3.7%, 11.4%, and 17.7%, respectively. These were comparable to the reports from other countries. Female gender and staying away from family were significant predictors. The government of India has already been taking a lot of initiatives to cater to the psychological needs of the general population and its HCPs, and we recommend that these measures continue to be in place at least till the pandemic completely phases out itself.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.