
Abstract
Background:
Bariatric surgery (BS) is an effective therapy for those who are excessively obese. However, the consequences of surgery on mental health are still debatable. We aimed to investigate the patients’ depression, stress, and anxiety levels before and after BS at two different times: just before surgery and 12 months later.
Methods:
This is a repeated cross-sectional study. The Depression Anxiety Stress Scale (DASS-21) was used to assess depression, anxiety, and stress levels.
Results:
There were 288 participants in the BS groups. Changes in anxiety, stress, and depressive symptoms over time were examined using generalised estimating equations models with repeated measurements per individual. Anxiety (incidence rate ratio [IRR] = 1.2, p < .001) and stress (IRR = 0.86, p < .001) worsened, whereas depression (IRR = –1.8, p < .001) improved significantly in 288 patients one year after BS.
Conclusions:
BS had significant impacts on obesity-associated mental health issues.
Research has indicated that bariatric surgery (BS) may have a positive effect on depressive symptoms. Nevertheless, there is also evidence to suggest that the procedure could potentially increase levels of stress and anxiety. In the postoperative phase, diligent monitoring of patients’ psychological well-being and the provision of appropriate support and treatments by healthcare personnel is of paramount importance.Key Messages
The escalating incidence of obesity has emerged as a global public health concern. 1 Based on data from the National Health and Nutrition Examination Survey, the age-standardized prevalence of obesity among adults in the United States experienced a notable rise from 33.7% in 2007–2008 to 39.6% in 2015–2016. 2
Patients who are overweight or have obesity are distinguished by an excessive buildup of adipose tissue, a condition that presents a significant health hazard. Obesity is defined as a body mass index (BMI) exceeding 30. Overweight is defined as a BMI exceeding 25. 3 When the risk of adverse health effects increases due to the accumulation of too much fat, this can contribute to detrimental health consequences. 4 Potential health implications encompass a range of conditions such as cancer, cardiovascular disease, type 2 diabetes, and stroke.5,6 In addition to physical problems, individuals with obesity face significant psychological difficulties. 7 Depression is the most prevalent psychological problem that obese people experience,8,9 as well as exacerbate obesity and its associated decline in quality of life. 10 In addition, those who are obese usually report having higher rates of anxiety and low levels of self-esteem.11,12
Lifestyle, pharmacological, surgical, and endoscopic bariatric therapies for obesity have been used. 13 Several longitudinal studies show that obesity is still generally resistant to standard treatment techniques.14,15 Only BS provides long-term medical benefits and weight loss. 16 BS limits food intake or absorption. 17 The most frequent current bariatric procedures include gastric bypass (GBY) and sleeve gastrectomy. 18
It has been discovered that BS considerably affects the mental health of patients undergoing this form of surgery. 3 Mental health research before and after BS is essential for ensuring complete treatment and support throughout the weight loss process. 19 Understanding the psychological effects of BS can assist medical professionals in detecting and treating mental health conditions, thereby improving patient outcomes and well-being. 20 Studies showed that almost 45% of BS candidates exhibit a depressive disorder, 21 and 15%–25% anxiety disorders.22–24 Even though most patients experience a reduction in psychological symptoms after BS, 3 a large proportion continue to experience psychological issues, and in some instances, their mental health deteriorates. Moreover, research has demonstrated that individuals who are intending to have BS are more likely to suffer from anxiety than depression. 24 As a result, incorporating mental health practitioners within bariatric teams would aid in monitoring patients for unfavourable psychosocial outcomes and identifying patients who are at risk of depression, anxiety, or other kinds of mental health problems following surgery. 25
Although the prevalence of psychological issues is an essential clinical concern for obesity, there are still significant gaps in the evidence regarding mental health before and following BS. Therefore, the study’s primary objective was to investigate patients’ depression, stress, and anxiety levels before and after BS at two time points: immediately before the surgery and 12 months later. We hypothesised that BS would impact patients’ depression, stress, and anxiety.
Materials and Methods
Study Design
A repeated, descriptive cross-sectional research design was used for this investigation.
Setting
At Safwat ElGolf Hospital in Egypt, the research was carried out at two distinct time intervals: time 1, spanning from January 2022 to June 2022, and time 2, extending from January 2023 to June 2023.
Participants
The study included individuals who were residing in Egypt and were pursuing weight loss treatment at the nutrition & weight loss clinic. They were required to satisfy the specified inclusion criteria. The criteria for inclusion were as follows: weighing over 30 kg/m2 and falling within the age range of 18–65 years. Exclusion criteria include any pre-existing medical conditions that could influence the results of the study, such as schizophrenia, epilepsy, or severe cardiovascular disease. In addition, participants who are currently taking medications that may interfere with the objectives of the study will be excluded.
Variables
The primary outcome measurements were the patients’ depression, anxiety, and stress scores. Every primary outcome was assessed at baseline, immediately prior to the surgery, and 12 months after the procedure.
Instruments
We utilized standardized questionnaires. The data for the study were gathered using:
Personal Information: Sociodemographic, personal, family-related, social, economic, educational, and academic inquiries are included. Patients were asked about the type of BS they would undergo, their physical activities, their level of satisfaction with their physical appearance and their need for psychological support.
Depression Anxiety Stress Scale (DASS): 26 The DASS was used to assess the mental health of the subjects. The DASS is a self-report, well-validated tool that has been proven by various studies across a wide range of demographics. 27 The DASS evaluates three mental health domains: depression, anxiety, and stress. Individuals respond to a succession of questions based on their experiences over the previous week. The DASS-21 was validated as a valid and reliable instrument for assessing depression, anxiety, and stress due to its strong psychometric properties. 28 The Cronbach’s alpha coefficients for stress (0.91), anxiety (0.79), and depression (0.93) were all acceptable. It was determined that the test-retest reliability of the DASS-21 and its three dimensions was satisfactory (0.74–0.88, P < .01). 29 The present study exhibited a high level of one-week test-retest stability (0.89).
Study Size
Statistical analysis using SPSS Sample Power confirmed that the sample size was large enough to detect substantial primary outcome differences. According to previous research, we chose a two-tailed significance test with 0.80 power, an unstructured covariance matrix with two-time points, a correlation of 0.50 between repeated assessments, a margin of error of 5%, and a 30% attrition rate between time 1 and 2. 30 With 250 individuals, group differences in outcomes are 80% detectable.
Procedure
We asked that individuals who agreed to participate be interviewed and have their evaluations completed at the nutrition clinic at time 1. At time 1 of evaluation, the patients’ BS had already been scheduled. At time 2, participants are emailed to complete the DASS assessment 12 months after BS. Each participant required roughly 15–20 minutes to complete the questionnaire.
Ethics and Human Subjects Issues
The study was approved by the British University in Egypt Institutional Review Board (IRB Protocol CL-2310). The information sheet and consent form were signed by participants. They were told about the research’s nature, process, goals, data confidentiality, the option to participate in the study, and the ability to withdraw at any time. The participants were informed that the trial will include psychological assessments.
Statistical Analysis
The IBM SPSS Statistics, version 23 software was used to analyse the data. The sociodemographic and baseline features of this sample were described using descriptive statistics (means, standard deviations, frequencies, and percentages). For repeated assessments of DASS scores, generalized estimating equations (GEE) were used. 31 A temporal within-subjects autoregressive [AR(1)] correlation matrix was used. Due to outcome measure distributions, models were created. DASS scores were modelled using identity link functions for normal distributions. We chose GEE because it extends the generalized linear model, processes repeat measurement data, requires no parametric distribution assumption, provides robust inference for an incorrect description of subject internal correlation, and provides good within-subject correlations. 32 To reduce the possibility of Type-II errors, interactions at least trend-level (i.e., α < 0.10) were investigated for simple effects at the follow-up time point, as was done in other research using equivalent analytic approaches. 33 At the (α = 0.05) threshold, all simple and main effects were found to be statistically significant (two-tailed). To adjust for Type I errors, Bonferroni corrections were used for all DASS outcome models. Missing data in important models was investigated further with sensitivity analysis and multiple imputations.
Results
Sociodemographic Characteristics
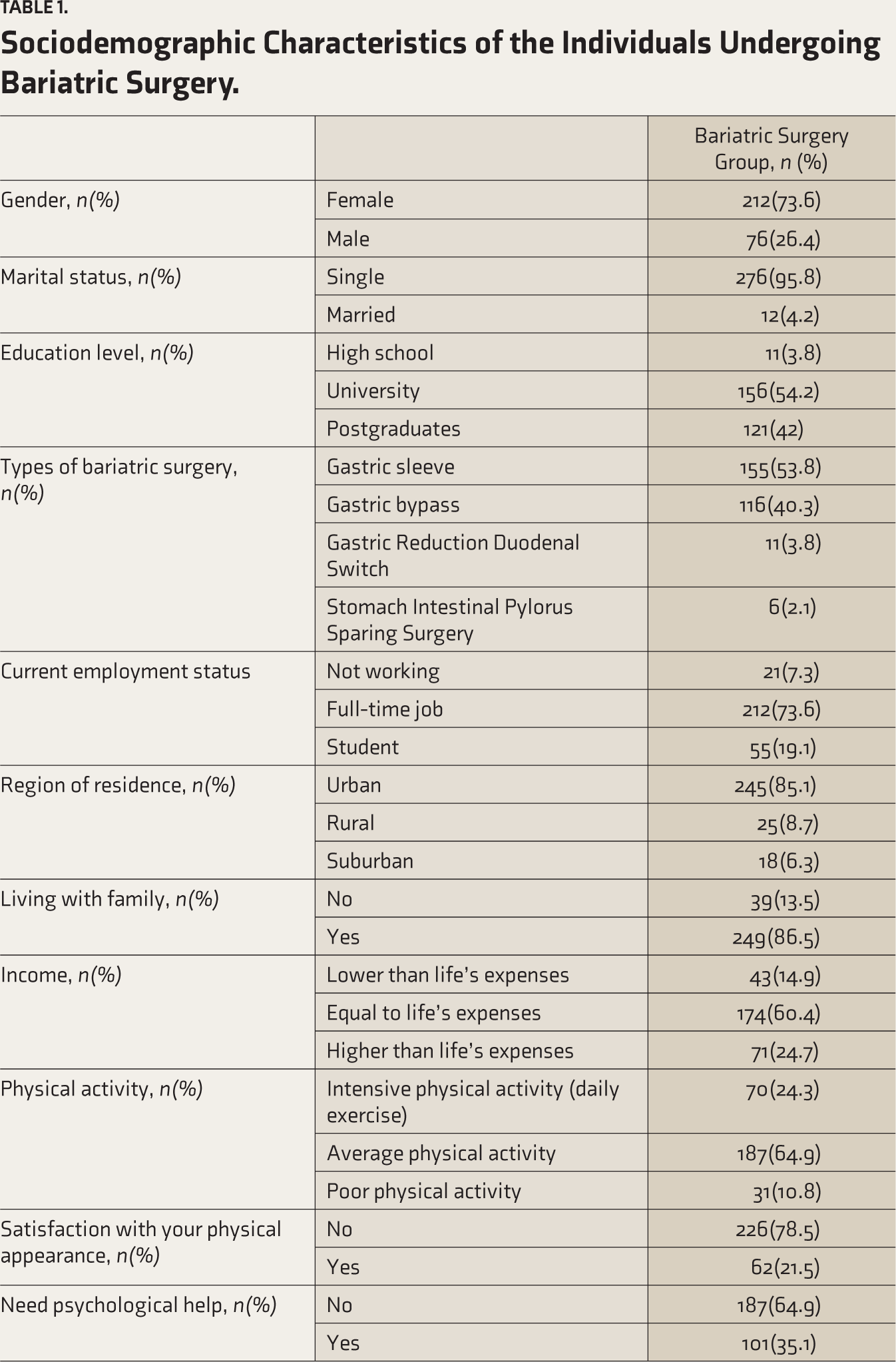
At time 1, 288 patients had been interviewed and had completed the DASS. At time 2, only 217 patients had been interviewed and completed the DASS. Table 1 displays the sociodemographic characteristics of the subjects. There were (N = 288), 73.6% females and 26.4% males. The mean age of the 288 participants was (M = 20.24 ±3.8) years (min. = 17, max. = 36).
Sociodemographic Characteristics of the Individuals Undergoing Bariatric Surgery.
Time 1 to Time 2 Differences in DASS Scores
As shown in Table 2, anxiety (incidence rate ratio [IRR] = 1.2, p < .001) and stress (IRR = 0.86, p < .001) worsen, whereas depression (IRR = –1.8, p < .001) improves significantly in 288 patients one year after BS.
Differences in Stress, Anxiety, and Depression Scores between Before and One Year After Bariatric Surgery.
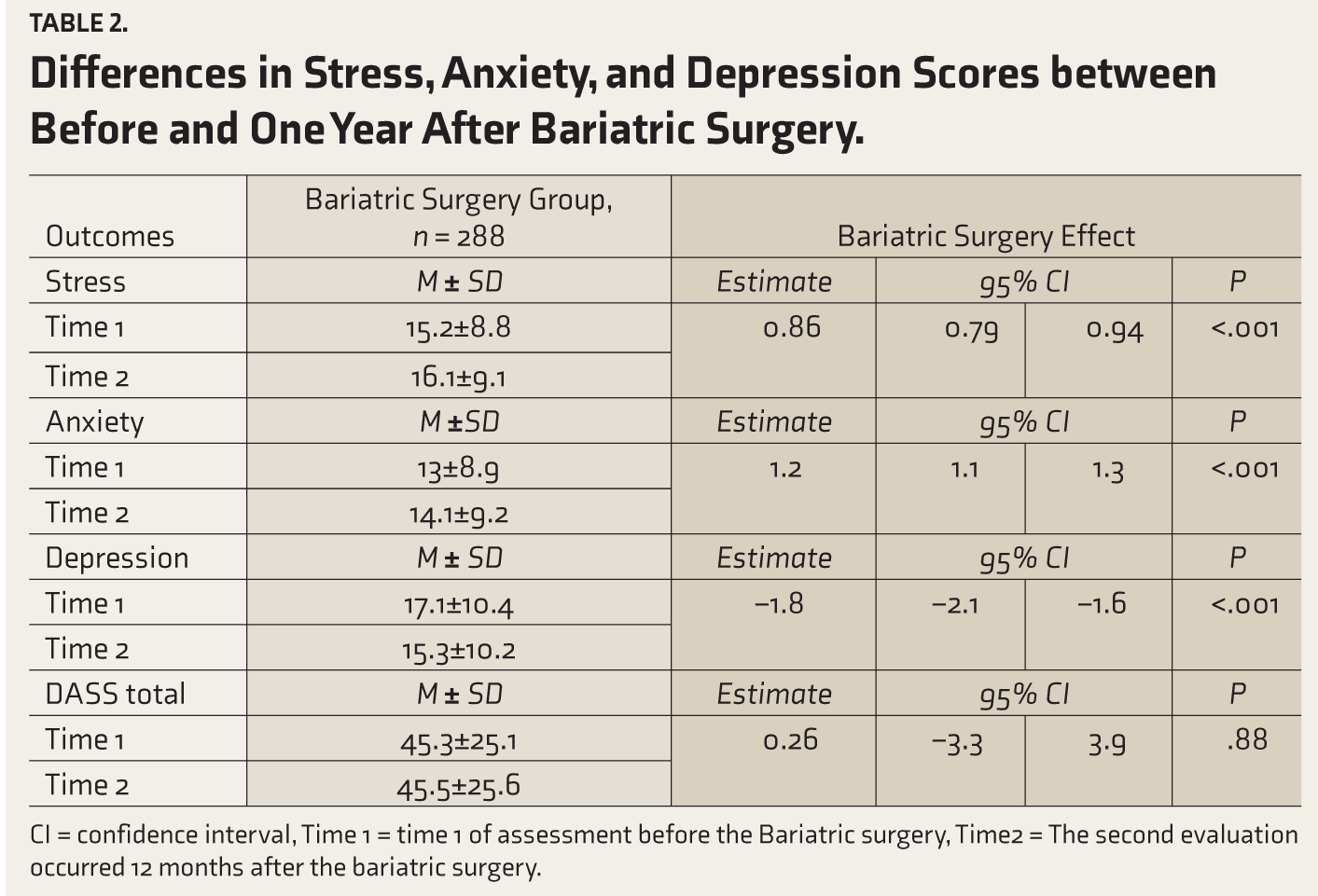
CI = confidence interval, Time 1 = time 1 of assessment before the Bariatric surgery, Time2 = The second evaluation occurred 12 months after the bariatric surgery.
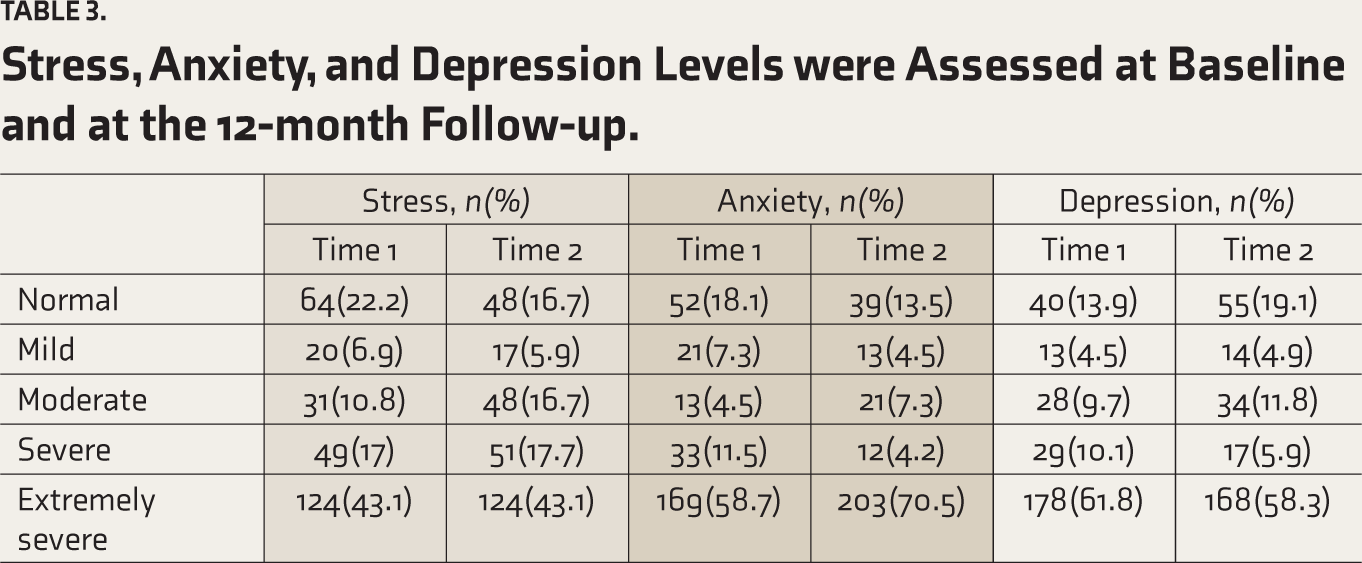
As shown in Table 3, there were differences between baseline and 12-month follow-ups in the observed levels of stress, anxiety, and depression among the patients. According to our study, there was a significant increase in anxiety and stress scores one year following BS. Also, there was a significant decrease in depression scores one year following BS.
Stress, Anxiety, and Depression Levels were Assessed at Baseline and at the 12-month Follow-up.
Discussion
Patients’ mental health is affected by BS. The major goal of this study was to look at mental health before and after BS at two periods in time (immediately before and 12 months after surgery). According to our findings, the anxiety and stress levels of 288 patients one year following BS increased significantly. In contrast, considerable improvement in the same group of patients’ depression symptoms was seen.
Recent research examined the development of anxiety and depressive symptoms after BS. According to the findings, six weeks and three to six months after BS, depression symptoms improved significantly. 34 People who underwent BS and then completed the Beck Depression Inventory (BDI) both before and after the procedure exhibited substantial improvements in their level of depression six and twelve months after the procedure. 21
Consistent with previous findings, our findings demonstrated the improvement of depressive symptoms following BS. 35 In one study, researchers looked at the association between weight loss and psychological characteristics such as depression, anxiety, health-related quality of life, and self-esteem up to four years following BS. They observed substantial improvements in depressive symptoms, the physical component of quality of life, and self-esteem one year following BS. These improvements remained after four years after surgery. 36 However, another study found that, while BS patients initially had benefits in depression, anxiety, and self-esteem, these improvements deteriorated by the nine-year evaluation and were comparable to or worse than preoperative levels. 37 The outcomes of prior research imply that the initial beneficial effects of BS on mental health may not be sustained over time. Following surgery, healthcare practitioners must evaluate patients and give continuous assistance to address any possible recurrence or aggravation of mental health issues.
In contrast to our findings, Ribeiro et al. 38 found that anxiety symptoms decreased during the first 23 months following BS, indicating significant healing during this time period. However, all anxiety indicators rose beyond the first 23 months following surgery. emphasizing the transitory influence of weight loss or BS on these symptoms. 38 Also, contradictory to our results, the authors of a systematic study that examined the outcomes of BS at 24 months and beyond concluded that anxiety levels decreased overall more than 24 months after the procedure. 39 After BS, the development of stress and anxiety symptoms is a complicated and multidimensional issue. Some individuals may experience improvements in mental health because of the procedure,34,39 while others may develop or worsen anxious symptoms. The anxiety and stress levels of patients one year after BS were substantially higher than their pre-surgery levels, according to our findings. This increase in stress and anxiety may be attributable to several factors, including the adoption of new eating behaviours, and the need to maintain weight loss. 40 Our findings revealed that patients’ anxiety and stress levels one year after BS were significantly higher than their pre-surgery levels, owing to the fact that they were still adapting to the physical and mental changes caused by the operation. Furthermore, the patients may have been concerned about long-term weight management and potential consequences following surgery. Patients were concerned that their stomachs would expand again and they would gain weight after reducing it.
This is the first study that investigates levels of stress, anxiety, and depression before and after BS at two time points in Egypt.
The implication of the current research can be described as increasing awareness of the effects of BS on mental health.
Recommendations: Given the risks of BS and the potential that patients would experience psychological discomfort, recommendations for patient assistance are required. Routine psychological examinations before and after surgery should be required under these recommendations to detect any prior mental health disorders or possible risk factors. Furthermore, healthcare practitioners should offer extensive counselling and therapy services to help patients overcome emotional challenges that may develop during their weight reduction journey.
Limitations and Future Directions
First, this study is based on self-report; a significant constraint is the participant’s capacity and willingness to offer personal information about depression, anxiety, and stress. A bigger sample of BS patients may be used in future studies to examine the relationship between BS and depression, anxiety, and stress. Furthermore, it would be beneficial to explore the long-term effects of post-operative problems on patients’ overall health and quality of life. Understanding the possible influence of characteristics including gender, obesity level, and need for psychological support might give useful insights for improving patient care and surgical results in the future.
Conclusion
Patients who underwent BS experience psychological consequences. According to the present study, while BS may have a good influence on depression symptoms, it may also raise anxiety and stress levels. Our results have therapeutic implications for post-surgical recovery and mental health. These data suggest that BS may alleviate depression and improve patients’ quality of life. It is critical that healthcare providers regularly evaluate patients’ mental health after surgery and give the appropriate support and treatments. More study is needed to understand the underlying mechanisms that contribute to these various outcomes and to develop strategies to improve patients’ psychological well-being following surgery.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.