
Abstract
Background:
COVID-19-driven pandemic has caused panic, fear, and stress among all strata of society. The study aimed to assess stress and the factors that influence it in a representative population in the state of Tamil Nadu (TN)—a state in the southern India where the levels of stress have not been measured yet.
Methods:
From April 13 to April 25, 2020, we conducted an online survey among the TN population using the snowball sampling technique, collecting basic demographic data. COVID-19-perceived stress was collected through COVID-19 Peritraumatic Distress Index (CPDI). Binomial regression analysis was used to identify the extent of the relationship between CPDI and sociodemographic factors by estimating the odds of having significant stress. P ≤ 0.05 was considered significant.
Results:
A total of 2,317 valid responses were received. Of the respondents, 830 (35.82%) were males, 1,084 (46.79%) were below 25 years of age, and 2,297 (99.14%) were native residents of TN. The mean(±SD) CPDI was 20.66±12.03. While 1,830 (77.2%) respondents had low or no stress, 478 (20.2%) had mild to moderate stress, and 63 (2.7%) had severe stress. The bivariate model included marital status, age, nativity, and income. The odds of having significant stress (mild–moderate or severe) for a 25–34 year age group as compared to >55 years group was 2.38 (P < 0.001). As compared to widowed, the married had higher odds ratio (3.41, P = 0.05). Compared to those with >10 lakh annual income, those with 2.5–5 lakhs annual income had odds ratio of 1.65 (95% CI = 1.01 to 2.7, P = 0.05).
Conclusions:
During the lockdown due to COVID-19, every 1 in 5 TN population had some form of stress, as measured by CPDI. Our model identified certain factors driving the stress, which would help policy framers to initiate an appropriate response.
Every 1 in 5 Tamil Nadu respondents had some form of COVID-19 related stress, and 2.7% had severe stress. For the 25–34 years age group, those with an annual income of 2.5–5 lakh, and married, were more prone to stress. A total of 6% were irritable and entered into conflict with family members more than usual; 2.4% of respondents could not sleep well and had bad dreams related to COVID-19.Key Message:
Widespread infection, social-media-fueled panic, and disruption creates stress, and thus, has a psychological impact. Meta-analyses revealed that anxiety and depression (16–28%) and self-reported stress (8%) are the common psychological reactions to this pandemic.5, 6 Social isolation, interpersonal distancing, heightened need for infection-control procedures, fear of infection, public perception of COVID-19 stigma, concerns about self/family well-being, the potential of facing emotionally charged clinical environments, issues of financial insecurity, and potential loss of income could precipitate stress.6–8
In the present COVID-19 crisis, a third of the Chinese public (n=52730) manifested psychological stress, with 5% experiencing severe stress. 9 Similarly, 14.1% of the Iranian public (n=1058) suffered severe stress and 47%, moderate stress. 10 Among Indians, a small unstructured general public survey (n = 662) reported that the respondents were preoccupied with the thoughts of COVID-19 (80%) and had sleep difficulties (12.5%), paranoia about acquiring COVID-19 (37.8%), and stress (36.4%). Four of five Indians perceived mental healthcare needs. 11
TN has an effective healthcare delivery system. 12 It also has an established, strong mental health surveillance and treatment program.13, 14 To date, the psychological (dis)stress perception due to COVID-19 has not been assessed among Indian citizens in TN. This study intends to address this lacuna and evaluated the patterns of perceived psychological stress as well as explored the factors associated with it.
Materials and Methods
An online survey for assessing psychological stress among people of TN was conceived in early April 2020 after reports of COVID-19-related suicide and self-harm behavior in India.15, 16 The survey was conducted from April 13 till April 25, both days inclusive. This coincided with the phase 2 of the lockdown. A waiver was obtained for this survey from the first author’s institutional review committee, as this was completely an anonymous survey with no personal identification collected, invasive procedure carried on, or disease exposure details collected. Also, the survey was carried out during a humanitarian emergency and disaster, as per the Indian Council of Medical Research guidelines. 17
The survey was done exclusively using a self-administered bilingual form in English and the local language, Tamil (with back translation verified). The instrument was designed using simple Google Forms and the link was shared among various social media and public platforms, using the snowball sampling technique. Anonymity was ensured and no personal identification, such as IP address, email IDs, or details of COVID-19 exposures, was collected. Participation was on a purely voluntary basis. The demographics of gender, the age group in years (<25, 25–34, 35–44, 45–54 and ≥55), nationality (Indian/other than Indian), state of origin (TN/other Indian states), the state presently living in (TN/other Indian states), marital status (married/unmarried/separated/widowed), nature of employment (student/unemployed/self/government/private), and annual income (in Indian rupees) as per government income tax categorization (below 2.5/2.5–5/5–10/above 10 lakhs) were collected. The state of origin and residence were combined to form people of TN, including TN residents, emigrants (person of TN origin who had left the state), and immigrant population (non-native of TN but settled in there).
The survey also used the previously validated questionnaire, COVID-19 Peritraumatic Stress Index (CPDI). 9 This self-reported questionnaire captures the details concerning anxiety, depression, phobias, cognitive change, avoidance and compulsive behavior, physical symptoms, and loss of social functioning in the past week and collectively quantifies the stress on a scale of 0–100. A CPDI score of ≤27 indicates low or no stress, 28–51 indicates mild to moderate stress, and ≥52 indicates severe stress. 9
The data were analyzed using Statistical Package for the Social Sciences (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp). Descriptive statistics, mean ± standard deviation (SD) or median for continuous variables, as well as proportions for categorical variables was calculated. Association of demographic variables with stress levels obtained by CPDI was assessed by the Pearson χ 2 test. For assessing the odds ratio, the stress was classified as no or low stress and as significant stress (mild to moderate and severe together). The magnitude of association of demographic variables with levels of stress was analyzed using binomial logistic regression and presented as odds ratios with 95% confidence interval (CI). Hosmer–Lemeshow goodness-of-fit test was used to assess the model fit. P ≤ 0.05 was considered statistically significant.
Results
We received a total of 2,317 valid, completed responses. Of them, 830 (35.82%) were males, 1,084 (46.79%) were below 25 years of age, 1,179 (50.89%) were unmarried, 1,016 (43.85%) were students, and a vast majority of them were earning less than INR 2.5 lakhs per annum (1,637, 70.65%). Of all respondents, 2,297 (99.14%) were both natives of TN and residing in TN, while the rest were either immigrants or emigrants.
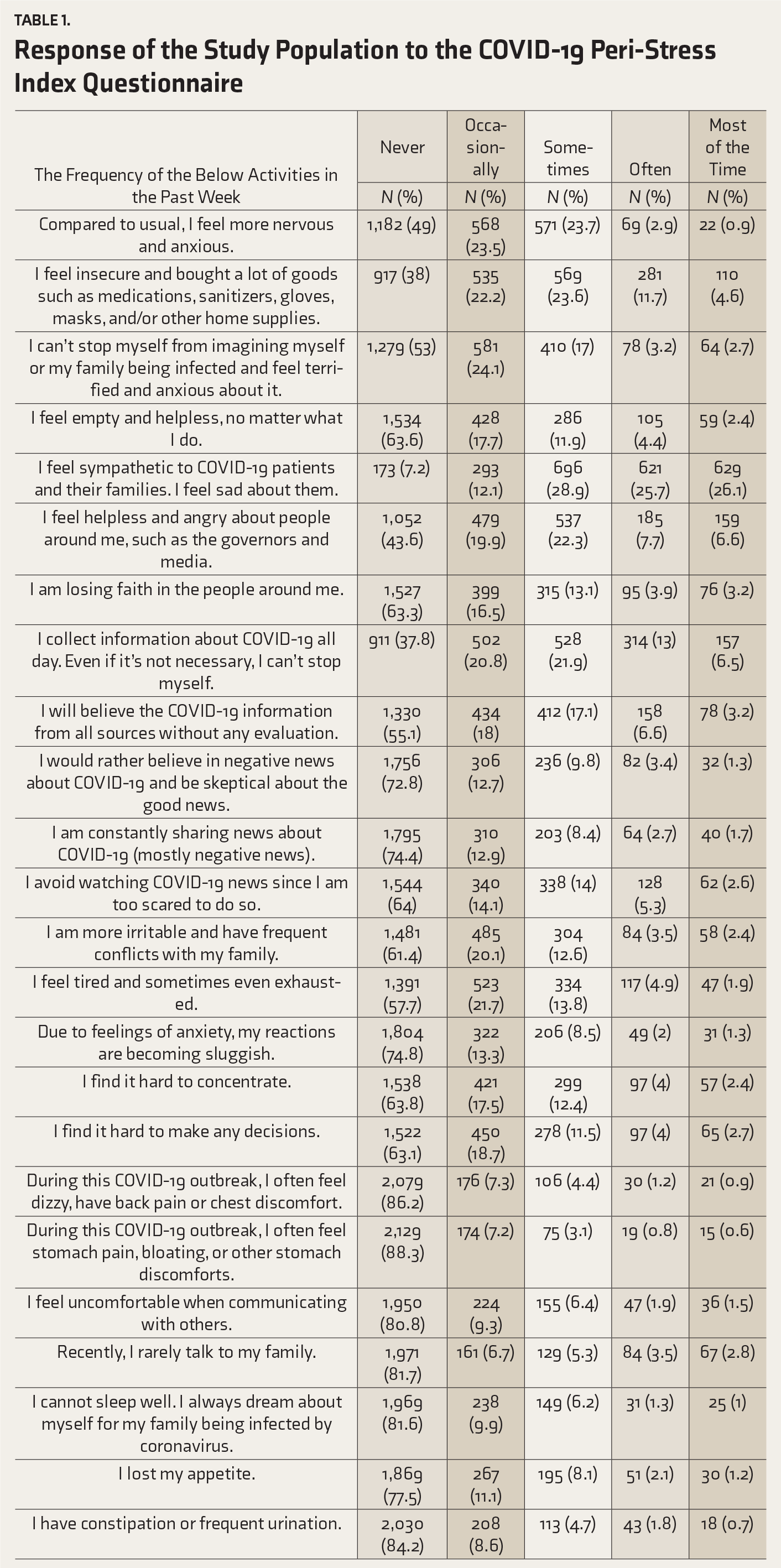
Response of the Study Population to the COVID-19 Peri-Stress Index Questionnaire
Demographics of Study Population (n = 2,371)
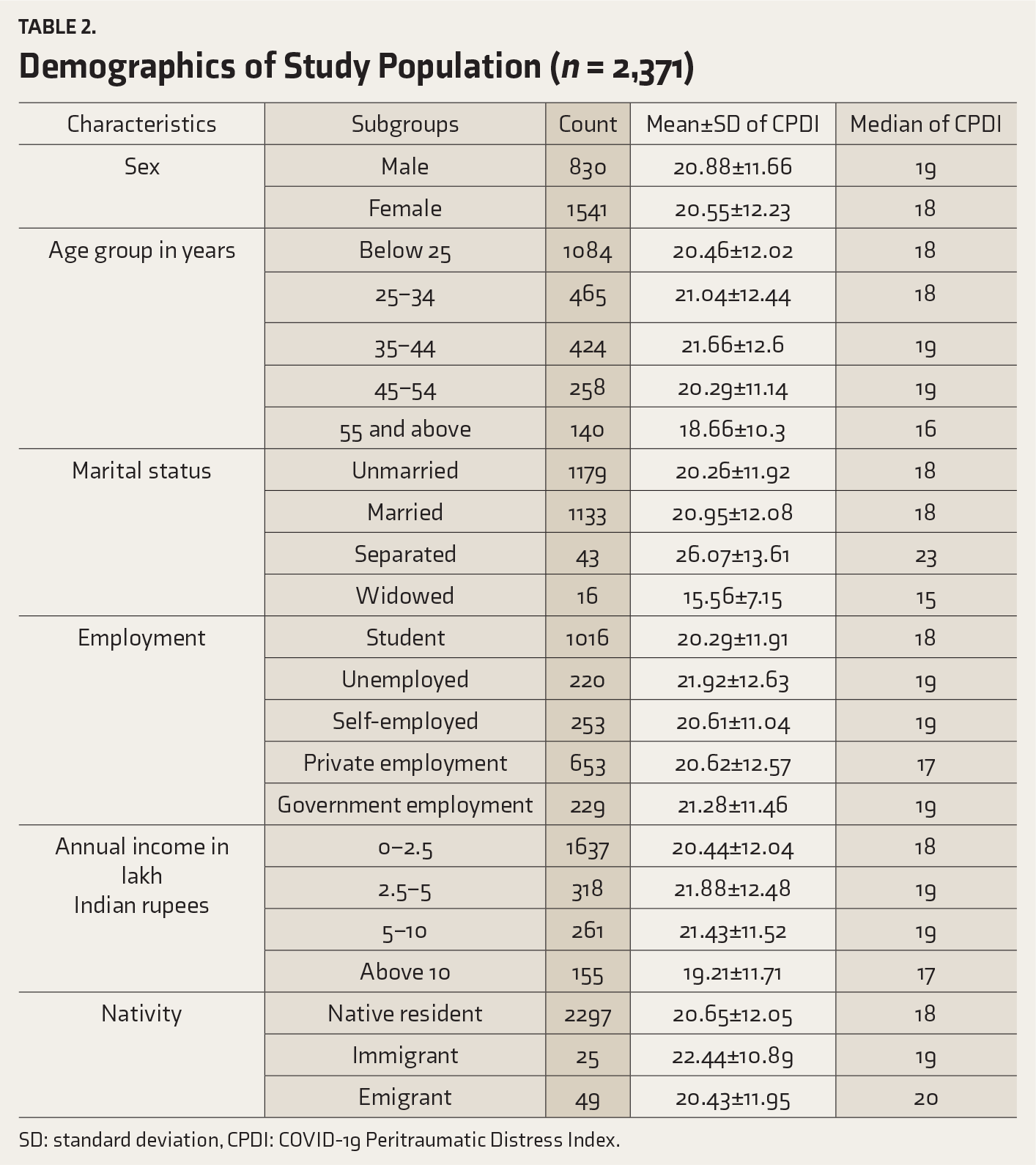
SD: standard deviation, CPDI: COVID-19 Peritraumatic Distress Index.
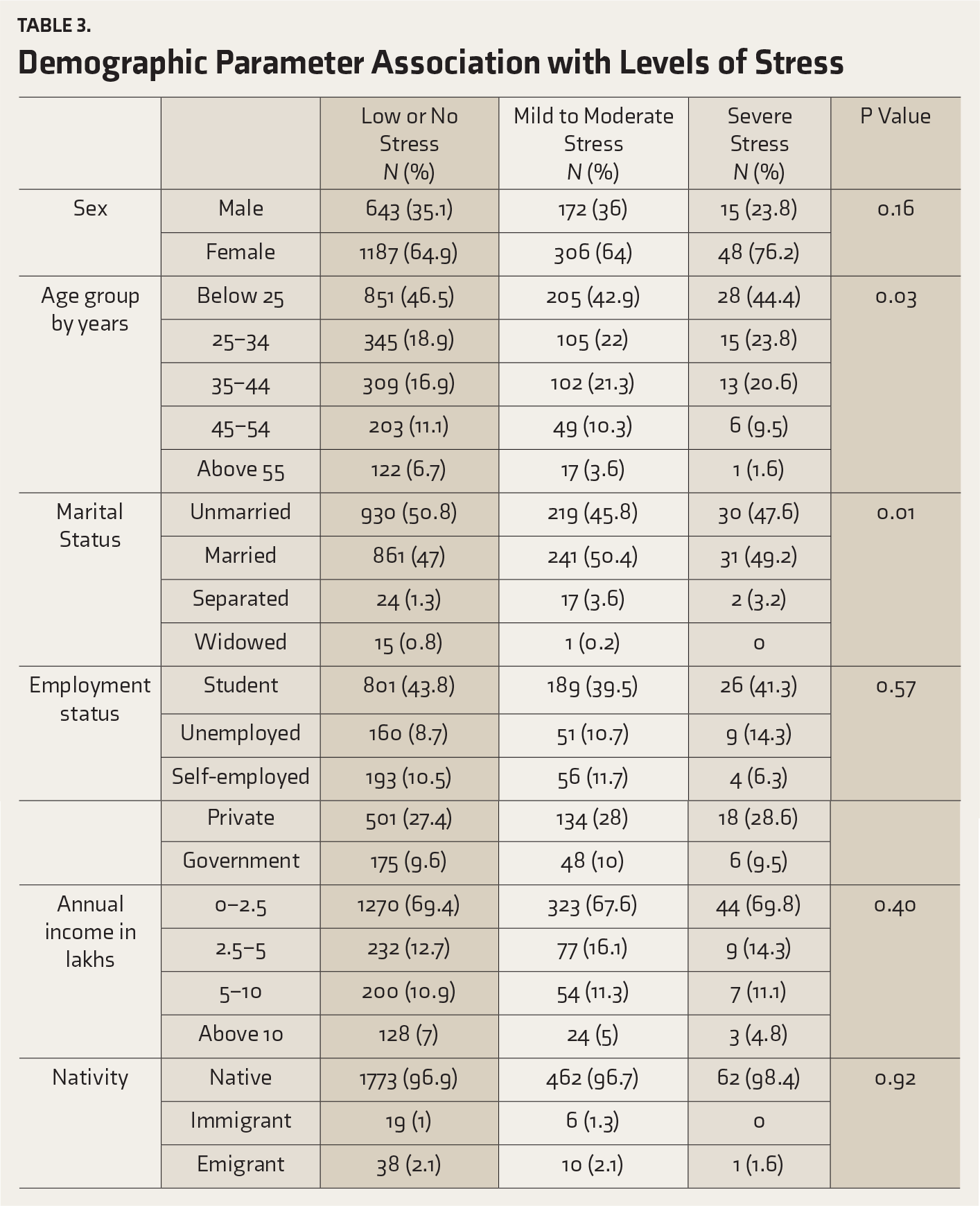
Demographic Parameter Association with Levels of Stress
Binomial Logistic Regression Analysis to Assess the Stressor with No or Less Stress as a Comparison Group to Those with Significant Stress (Mild to Moderate and Severe)
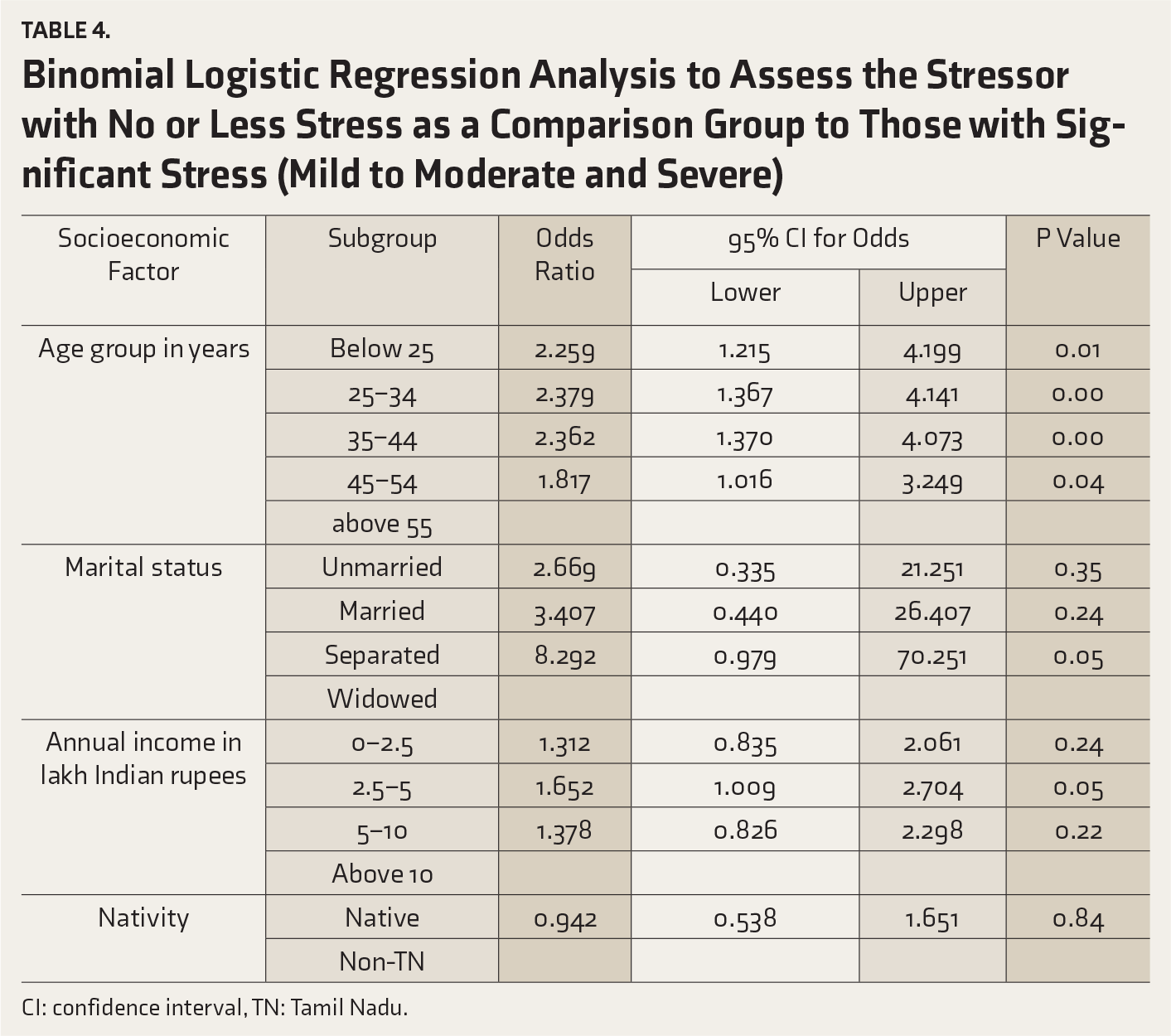
CI: confidence interval, TN: Tamil Nadu.
Discussion
Besides physical health, mental health also takes a strong hit during a pandemic. Past pandemics have underlined the need for an efficient mental health screening program and integration into the pandemic response. The stress, fear, and panic could fuel emotional and behavioral turmoil, precipitating mental health burden during or after the pandemic. Psychological factors play a vital role in determining the behavior of the public and their contribution to lockdown and isolation. 18 As there was a paucity of data on the stress reaction to the developing COVID-19 situation in TN, this study was designed to capture the stress among the general public using a non-contact, anonymous, brief, indirect, self-reporting, and self-volunteering format.
Unlike the Chinese CPDI score of 23.65±15.45 and Iranian score of 34.54±14.92, TN had 20.66±12.03.9, 10 About 61% of Iranian and 35% of the Chinese public had relatively higher stress, as compared to 23% in the TN sample.9, 10 This difference could emanate from the fact that both the countries had heightened spread and were epicenters of the outbreak during the data collection, as well as the fact that TN (and India) were never hot spots by the time of the collection and writing of this data. The present data collection was done after the lockdown extension.
This study, to the best of our knowledge, for the first time, has provided robust measures of psychological stress profile of the general public in TN in COVID-19 situation. The sociodemographic factors that precipitated psychological stress differed widely between Chinese and Iranian studies.9, 10 This study also identifies association of different factors. In the present study, young adults were predisposed to stress as compared to no or low stress, with an OR < 2 with high statistical significance. This could be due to several reasons: Young TN public is much exposed to smartphones, news, and social media. Rapid increase of COVID-19 virus and social media-fueled COVID-19-related voluminous information, including unverified claims, may precipitate stress and other psychological reaction.19–21 In this regard, this study resonates with Chinese studies.8, 22 Those with an average annual income of INR 2.5 to 5 lakhs had a significant odds ratio (OR=1.65, P = 0.05) as compared to those earning above ten lakhs per year. Age is a major contributor for stress with odds ratio ranging from 1.8 to 2.38 in different age groups as compared to those above 55 years. Younger people are at more risk to stress as compared to those above 55 years. Marital status plays a very significant influence on stress. This aspect has not been described in earlier studies. As there is no precedence, the findings could not be compared with existing literature. As there was only a small number of immigrants and emigrants, the influence of this factor could not be compared, though narrative reviews are available. 23 Also, our results broadly resonate with those of a recent index survey from West Bengal, India. 24
Present findings provide robust insights into the features of psychological stress in the TN public. The pre-COVID-19 prevalence of various psychological disorders were estimated: mood disorders at 4.62%, depressive disorders was 3.61%, anxiety related disorders 3.5%, and neurotic/stress related disorder 1.9%.25–27 In this study, 22.8% had significant stress, with 2.7% of respondents having severe stress. This underlines the need for providing mental health assistance to vulnerable groups such as young people, those with lower income levels, and those lacking a support system. The system also needs to dynamically provide access to mental health support systems. There is a need for strategic planning and development of COVID-19-related psychological first aid team that should indulge in non-contact monitoring, screening, referral, and targeted intervention procedures. As one in five of the population could suffer from stress, the focus should be on preventing stress among those with mild-to-moderate stress while providing mental health care for those with severe stress. This is a mass, self-administered tool. Only initial screening is feasible and this tool can identify those with significant stress. Further clinical interview and psychological aid have to follow.
The results of this study should be interpreted with caution as this is an observational cross-sectional survey, and done in a relatively small, smartphone-handling sample. This sample could not be representative of the entirety of TN. Also, there are limitations in online surveys, particularly those in which the response rate is not known.28, 29 Also, the low (pseudo) R 2 but statistical significance indicate that there could be outliers and other confounding factors. This underlines the need for further studies with larger sample size and accounting more sociodemographic factors. Future studies have to take these limitations into account.
Conclusion
COVID-19 pandemic has created stress across all spheres of human life. The stress among the TN population has been captured in the initial phases of the pandemic containment effort. This would help the mental health professionals and the policymakers to institute appropriate mental health efforts and solutions during the lockdown as well as when the normalcy is restored.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.