
Abstract
European countries have experienced significant inflows of migrants in the past decade, including many refugees from regions engaged in armed conflicts. Although previous research on migrant health has largely focused on economic migration, empirical evidence on refugee health is sparse. This article uses administrative data from Austria to differentiate between economic migrants and refugees and to analyze both groups’ health-care expenditures in comparison to natives. We contribute to the literature on migrant health in several dimensions. First, we follow economic migrants and refugees over the first five years after arrival and show different health-care expenditure patterns among migration groups. In contrast to patterns for economic migrants, we find substantially higher health-care expenditures for refugees compared to natives, especially in the first year after arrival. This difference is not explained by specific diseases or individual refugee groups, indicating refugees’ generally inferior health status in the first years of settlement. Second, we focus on the health effects of granting asylum and find that the expenditure differences decrease after a positive asylum decision. In the last part, by using refugees’ quasi-random placement as a natural experiment, we show that the local health-care sector's characteristics do not have a significant effect on expenditure levels. The findings highlight the importance of distinguishing between migrant groups in the analysis of health-care utilization and show that the time spent in the host country, as well as legal status, have a substantial impact on migrants’ health-care utilization.
Introduction
Europe has experienced a substantial increase in immigration in recent years (King and Okólski 2019). The number of asylum applications in the European Union (EU) surged from 1.1 million in the years 2006–2010 to over three million in 2011–2015, with many refugees coming from countries engaged in armed conflicts, such as Syria, Afghanistan, and Iraq (Eurostat 2017). Many projections for global trends in international migration expect that large migration flows from developing countries to developed countries will continue in the future, driven by violence, armed conflict, climate change, economic disparities, and diverging demographic trends (OECD 2016). For example, Lutz et al. (2019) estimate an EU population of 521 million by 2060, given current migration patterns, but a population of only 476 million in 2060 without migration. In European countries, these demographic developments increase ethnic, cultural, and linguistic diversity and pose many challenges to society, ranging from labor market integration issues to health-care provision (Rechel et al. 2011; Brell et al. 2020).
An extensive body of research on migrant health has shown that, upon arrival, migrants tend to be healthier than the native population, a phenomenon known as the ‘healthy immigrant’ effect (e.g., Antecol and Bedard 2006). Health advantages have been documented for migrants via various outcomes, including health-care expenditures (Ku 2009; Vargas Bustamante and Chen 2012), subjective well-being (McDonald and Kennedy 2004), body-mass index levels (Antecol and Bedard 2006), and birth outcomes (Farré 2016; Giuntella 2017). Another common finding is that migrants’ outcomes tend to converge to native levels over time (Antecol and Bedard 2006; Vargas Bustamante and Chen 2012). In this article, we provide additional empirical evidence on migrant health. Using large administrative databases from Austria that cover the years 2005–2015, we differentiate between economic migrants and refugees and analyze both groups’ health-care expenditures in comparison to natives. 1
Migration is a selective process, and the decision to leave a country often depends on the costs and benefits for an individual (Abramitzky and Boustan 2017). Economic models of migration typically focus on migrants’ prospective labor-market returns and link the decision to migrate to a person's skills and the value of those skills in the destination country relative to the sending country (Borjas 1987). Most empirical evidence on recent migration flows to the United States and other OECD countries suggests that individuals migrating to developed countries are often positively selected regarding education and other observable skills (Docquier et al. 2007; Abramitzky and Boustan 2017). Positive selection is also a prominent explanation for the healthy immigrant effect, suggesting that healthier individuals are more likely to migrate (e.g., Antecol and Bedard 2006). Consistent with this hypothesis, studies have shown better health outcomes among migrants than among those who stay in their home countries (Kennedy et al. 2015; Farré 2016). This research on migrant health, however, has largely focused on new arrivals in general and has not distinguished between refugees and economic migrants, despite the fact that there are good reasons to believe that economic migrants and refugees have different health statuses, as we outline below. 2
Although both refugees and economic migrants leave their home countries, the push and pull factors that lead to their migrations likely differ (Bernard 1976). International (non-asylum) migration is driven by, among other motives, economic incentives, immigration policy, and network factors (Matsui and Raymer 2020), whereas the factors precipitating forced (asylum) migration include armed conflict, natural disasters (Zetter 2019), and civil-rights violations in connection with political oppression (Matsui and Raymer 2020). These push components may directly influence refugees’ health status, since during such crises, the local political and health-care system might break down and the provision of safe food and water, sanitation, hygiene, and general safety may not be secured. In some regions, medical care can no longer be ensured under these conditions, as medical personnel, such as doctors and nurses, are also trying to escape (Rehn and Johnson-Sirleaf 2002; Levy and Sidel 2016). Reduced access to health care and violent and traumatizing events in origin countries may have long-lasting impacts on refugees’ health (Brell et al. 2020).
In addition, the migration process among economic migrants and refugees differs. Economic migrants prepare for the destination country and typically can move safely (Bernard 1976). Refugees may experience perilous situations during flight, including violence, lack of shelter, and food insecurity, which may directly affect their individual health (Clinton-Davis and Fassil 1992; Brell et al. 2020). Furthermore, refugees may have less preparation time, as they often must flee suddenly (Gilbert and Koser 2006), and their intended destination can change during the flight (Crawley and Hagen-Zanker 2019). These circumstances could result in a lack of language skills and institutional information in the destination country (Bernard 1976; Havinga and Böcker 1999) and create additional barriers to the adequate use of the host country's health-care system. Nevertheless, a person's ability to move away and/or onward from transit countries may depend on various factors, including economic and social circumstances and health (Aksoy and Poutvaara 2019). 3 Even after arriving in the destination country, economic migrants and refugees may encounter different conditions. Refugees often have only limited access to health-care systems in their host countries (IOM 2008). Thus, observed differences between natives’ and refugees’ health-care utilization may be related to a worse health status and/or to different access to health-care services.
Likewise, the social environment plays a crucial role in health-care utilization (Devillanova 2008). If there are already many migrants with the same background (e.g., nationality, language) in a given destination country, economic migrants may become part of an (ethnic) enclave, where they have access to robust information networks (Bernard 1976; Barthel and Neumayer 2015). In contrast, Matsui and Raymer (2020) note that the since mid-2000s, a growing number of asylum-seekers have moved to OECD destination countries without historical relationships (e.g., former colonial ties, common language) or ethnic networks. Furthermore, even if social networks of family, friends, or co-ethnics exist in the destination country, the amount of information passed to those in forced flight is limited (Robinson and Segrott 2002). Although many studies show that asylum policies, (perceived) status of liberalism, economic performance and labor market access regulations in the destination country have a significant effect on migration flows and, therefore, asylum-seekers’ destination choice (e.g., Hatton 2004; Thielemann 2006; Barthel and Neumayer 2015), Gilbert and Koser (2006) and Robinson and Segrott (2002) remark that asylum-seekers often know too little about a destination country's asylum policies and living conditions to make an informed choice. A reason for such limited knowledge is that many asylum-seekers often did not know in which country they would end up (Crawley and Hagen-Zanker 2019), as their preferred destination country changed on the way when they faced obstacles (Crawley and Hagen-Zanker 2019) or when smugglers, not the (trafficked) persons themselves, decided where they should go (Gilbert and Koser 2006; Robinson and Segrott 2002). In addition, asylum-seekers often did not expect to meet any co-ethnics after arrival in the destination country (Gilbert and Koser 2006). Refugees who seek asylum in the destination country are, therefore, more likely to be dependent on voluntary agencies and non-governmental organizations (NGOs), as their access to ethnic networks is reduced (IOM 2008). Limited information about the host country's health-care system has a direct impact on refugees’ usage of health-care services and, thus, the received treatments and individual health status (IOM 2008). Furthermore, Bernard (1976) emphasized that refugees, on average, have a lower socioeconomic status than natives in the host country. In combination with the psychological stress of the asylum and admission process, these factors can lead to further health problems for refugees (IOM 2008).
Because of these differences, it is essential to distinguish between refugees and economic migrants when examining migrant groups’ health-care utilization. As mentioned above, previous work evaluating migrants’ use of health-care services in the host country has failed to differentiate between economic migrants and refugees. Since the number of people forcibly displaced from their homes has increased in recent years (King and Okólski 2019), refugees’ health-care utilization in host countries is a highly relevant research topic.
In this article, we construct a novel dataset to analyze refugees’ health-care utilization in Austria. Using high-quality administrative data on objective health outcomes and migrant legal status (i.e., whether the individual is or was an asylum-seeker), we differentiate between economic migrants and refugees who are currently in the asylum process or have been granted asylum. In doing so, we contribute to a small body of research on refugees’ health outcomes after arrival in host countries (e.g., Chiswick et al. 2008). The data and methods used here have a number of unique characteristics. First, we have information on objective health at the individual level in a panel data structure, which allows us to examine changes over time and the relationship between health-care utilization and legal status. Second, we compare population groups within the same public health insurance institution, and Austria's institutional setting grants the same formal access to services for all persons. Austria is, therefore, particularly useful for such an analysis because any remaining differences in utilization of health-care services can be attributed to other factors, such health-care needs or informal barriers. Third, we explore determinants of refugees’ health-care utilization, using information on the place where refugees live.
We find that, unlike economic migrants, refugees have significantly higher health-care expenditures than natives in Austria. This difference is most pronounced in the first year after arrival and decreases subsequently, indicating a convergence of expenditures over a longer period. We further show that refugee health-care utilization is highly correlated with legal status and that it sharply declines after a positive outcome of the asylum application.
To develop these arguments, the rest of the article is organized as follows. Background reviews existing evidence on refugee health and summarizes past migration patterns in Austria. Further, it describes the asylum process and health-care system in Austria and the data we use. Differences in Health Care Expenditures analyzes refugees’ and economic migrants’ health-care expenditures in the first years after arrival, while Legal Status and Health Care Utilization focuses on refugees’ legal status and analyzes health-care expenditures before and after they are granted asylum. Determinants of Health Care Utilization explores potential determinants of individual health-care utilization, and Conclusion discusses the implications of our findings for the wider study of international migration.
Background
Existing Evidence on Refugees’ Health
Meta-analyses of epidemiological studies suggest that refugees in high-income countries frequently experience violence-related health issues (Kalt et al. 2013) and that there is a high prevalence of infectious diseases (Clark and Mytton 2007) and physical (Hadgkiss and Renzaho 2014) and mental (Fazel et al. 2005) health problems among refugees. The results documented in these studies, however, often rely on small, non-representative samples. For example, refugees are invited to participate in studies when they have contact with refugee-supporting organizations or seek care at health clinics (Kalt et al. 2013).
An important exception is Chiswick et al. (2008), who contrast migrants’ self-reported health status by the type of visa used to gain entry to Australia. As they show, shortly after arrival, refugees using humanitarian visas less often rate their health as good or very good than do migrants with employment-related visas. Furthermore, for each immigrant category, they report a decline in health over the first 3.5 years after arrival, with the greatest decline recorded for refugees. In similar fashion, Kohlenberger et al. (2019) provide recent evidence on refugee health in Austria and show that refugees rate their subjective well-being worse than the resident population. These studies rely on survey data to compare respondents’ health status, raising questions about the validity of self-reported health state for cross-cultural comparisons. People from different countries may have different reference levels against which they judge their health, and, depending on the language, available response categories may have different associated connotations (Jürges 2007). Therefore, a comparison of health states of people from different countries may lead to misleading results if differences in reporting styles are not considered (Jürges 2007).
Bauhoff and Göpffarth (2018), to our knowledge, are the only scholars to analyze a large sample of refugees, using administrative data. Their work compares the health-care utilization of asylum-seekers, who, in Germany, have restricted access to health services, with regularly insured persons. Their mixed results suggest that asylum-seekers’ hospital expenditures are twice as high as that for regularly insured individuals, while expenditures for drugs and outpatient care among asylum-seekers are lower. Bauhoff and Göpffarth argue that this pattern could be explained by asylum-seekers’ inadequate access to primary care; however, this issue is not further investigated as the data cover only a small number of municipalities. Since the results relate to refugees who had only recently applied for asylum, a second question is how refugees’ health-care utilization develops over time, as experience with the health-care system increases. In summary, there is very little evidence regarding refugees’ objective health status, how it evolves over time, and on what determinants this status depends. This article intends to close this gap.
Migration in Austria
Austria and the EU as a whole have become important destinations for migrants in recent decades, with positive net migration in each year since the 1990s (see Figure A5 in the Online Appendix for details). In the 1960s and 1970s, northwestern European countries actively recruited workers from southern Europe to fill labor-market shortages (King and Okólski 2019). In Austria, former Yugoslavia and Turkey were the most important suppliers of so-called guest workers (Kraler 2011). Originally intended as a temporary presence, many workers and their families settled permanently in the country and influenced long-term migrations patterns through social and cultural ties (Halla et al. 2017).
The Iron Curtain's fall in 1989 removed an effective migration barrier at the edge of Austria and unleashed a new era of intra-European migration from the East to the West (King and Okólski 2019). Subsequent wars in former Yugoslavia brought additional migration flows to Austria (Kraler 2011). Since Austria's entry into the EU in 1995, labor mobility from other EU member-states has increased, as people seek employment opportunities in the country (Halla et al. 2017). The largest share of migrants in this group come from Germany, Austria's largest neighbor (OECD 2021). EU enlargements in 2004, 2007, and 2013 integrated eight Central and Eastern European countries, as well as two Mediterranean countries, into the EU, creating an area of free movement for half a billion people (King and Okólski 2019). In Austria, these developments resulted in the new EU member-states, Romania and Hungary, entering the top three source countries between 2006 and 2015 (OECD 2021; Table A17).
International conflicts, most notably in Syria, Afghanistan, and Somalia, brought further waves of refugees to Europe, sharply increasing refugee numbers between 2011 and 2015 (OECD 2016). In 2015 alone, more than one-million refugees arrived in Europe (Eurostat 2017). Most refugees only passed through Austria, although Austria was also among the top host countries in the EU (Eurostat 2017). From 2005 to 2013, while there were, on average, 15,000 asylum applications per year in Austria, 2015 saw more than 88,000 applications (BMI 2018; see Figure A6 in the Online Appendix). Refugees in the last decades have come to Austria from various countries, indicating the large diversity of global conflicts (OECD 2021; see Table A18 in the Online Appendix). Between 2001 and 2010, Afghanistan, Russia, and Serbia were the three most frequent nationalities among asylum-seekers in Austria (Table A18 in the Online Appendix). However, a significant number of refugees also came from India, Turkey, Georgia, and Nigeria (ibid.). Between 2011 and 2015, Syria and Iraq were among the top three source countries, behind Afghanistan (ibid.).
Asylum Process
After receiving an asylum application, Austria's federal office for immigration and asylum assesses the country's responsibility to conduct the asylum procedure (Limberger 2010). During this process, the asylum-seeker is placed in one of three national reception centers (Limberger 2010). If, according to the EU's Dublin regulation, Austria is responsible for the asylum application, the asylum-seeker is transferred to one of several asylum shelters spread across the country, where he/she receives basic welfare support, including accommodation, counseling services, some pocket money (40€ per month), and health insurance (Limberger 2010). Although Austria's nine regional states have the task of distributing asylum-seekers between municipalities, asylum shelters are often managed by non-governmental organizations (König and Rosenberger 2010).
The basic welfare support covers asylum-seekers, recognized refugees in the first four months after receiving asylum, failed asylum-seekers who cannot be deported, people who are entitled to subsidiary protection, 4 foreigners who have a right of residency for humanitarian reasons, and war-displaced persons and foreigners who are supposed to be sent to a different country responsible for the asylum process (Limberger 2010). Refugees are allowed to enter Austria's labor market three months after their asylum procedure begins, but access is restricted to selected occupations in the area of seasonal work, effectively excluding asylum-seekers from the labor market (Limberger 2010). Refugees are free to enter the labor market after receiving asylum status or apply for social security benefits if they do not find employment (Limberger 2010).
The distribution of refugees from reception centers to regional asylum shelters across Austria is handled by the federal government, in agreement with the respective state where a shelter is located, and follows a quota system wherein the state's population size determines the number of refugees (Koppenberg 2014). In practice, states receive lists of applicants who must be allocated on a daily basis and then provide feedback on how many and which applicants they can accommodate (ibid.). In the process, public authorities may take existing refugees’ family relations and special needs (e.g., disabilities) into account (ibid.). There are particular regulations for unaccompanied minors, who are entitled to be accommodated in specific facilities with increased supervision (ibid.). Operators of asylum shelters are not involved in the decision-making process (ibid.).
The legal basis for assigning refugees in Austria follows EU directives that lay down standards for the reception of applicants for international protection (Council directives 2003/9/EC and 2013/33/EUb22). Accordingly, countries have the right to assign refugees a place of residence (Council directive 2013/33/EU, Article 7). If a refugee rejects the offered accommodation, member states have the power to withdraw the reception conditions, including the refugee's entitlement to housing and basic welfare support (Rosenberger and König 2012). Therefore, Rosenberger and König (2012) note, from the asylum-seeker's perspective, the distribution policy has been described as a ‘no choice’ principle.
In our empirical analysis, we focus on Upper Austria, one of Austria's nine states. Figure A7 in the Online Appendix shows the regional distribution of migrants and refugees in Upper Austria in 2010, the middle of our analysis period. 5 Refugees are accommodated in 47.7% of Upper Austrian municipalities. The share of refugees in the municipalities varies between 0% and 8.9% of the population, with a mean of 0.25%. Figure A7 clearly shows that refugees are distributed across the whole state. They are also placed in smaller municipalities, which, in the past, had only small shares of the foreign population, 6 indicating the successful avoidance of strong clustering of refugees in certain areas. We also examined the influence of observable refugee characteristics in the distribution process, revealing no substantial association between individual characteristics and assigned municipalities’ features. 7
Health Care System
Austria's social security system includes mandatory public health insurance that covers almost the entire population (Hofmarcher 2013). The system is characterized by free choice and easy access to health-care providers and is devoid of strict gate-keeping mechanisms (OECD 2017). Compared to other European countries, Austria's health-care system has a high density of physicians and hospital beds (OECD 2017). Primary health care is mainly provided by general practitioners (GPs), who are typically self-employed and operate in single practices (Bachner et al. 2018). Additional health care is provided by medical specialists in the outpatient sector and hospitals (Bachner et al. 2018). Health insurance covers health-related costs in the inpatient and outpatient sector, including prescription drugs, dental care, and other services provided by GPs and specialists, with only minor co-payments (Hofmarcher 2013). Mental health care, however, is often only partially covered by public health insurance (Bachner et al. 2018). Private health insurance plays only a minor role in Austria and accounts for 5% of total health expenditure (OECD 2013). Private health insurance is used to complement public health insurance, for example, to cover the additional costs for private hospital rooms. However, hospitals are also reimbursed by public insurance for treatment costs of privately insured patients (Bachner et al. 2018). These expenditures can, therefore, be observed in the data analyzed here.
A person's affiliation with one of the health insurance-providing institutions is determined by occupation and place of residence and cannot be chosen freely (Hofmarcher 2013). The majority of Austria's population is covered by nine regional health insurance funds, which include all active and retired private-sector employees, individuals receiving unemployment or social security benefits, and these individuals’ co-insured dependents (Hofmarcher 2013). These funds also cover refugees who are entitled to basic welfare support during the asylum process and refugees who receive social security benefits or private-sector employment after receiving asylum status (Bachner et al. 2018). All insured persons are entitled to use the same health care (Bachner et al. 2018). Other social insurance funds offer health insurance for specific occupational groups, such as farmers, civil servants, and self-employed persons (Hofmarcher 2013). The institutional setting in Austria, thus, implies formally equal access to health services for all population groups. Any differences in health-care utilization should, therefore, be attributed to other causes, such as differences in health-care needs or informal barriers.
Data
For our empirical analysis, we use administrative data from the Austrian Social Security Database (ASSD), which contains labor market histories at the individual level, such as periods of employment and unemployment (Zweimüller et al. 2009). The ASSD also includes individuals’ socio-demographic characteristics, such as citizenship and information about refugee status, and can be linked to data from the Upper Austrian Regional Health Insurance Fund, which provides detailed information about covered health-care expenditures. The fund has more than one-million members and represents roughly three-quarters of the Upper Austrian population.
Expenditures related to physician visits in the outpatient sector are largely based on a fee-for-service scheme (Hofmarcher 2013). Conversely, expenditures for hospital inpatient treatment follow the Austrian diagnosis-related group (DRG) system (Bachner et al. 2018). Similar to other DRG systems, hospital cases are classified into a limited number of groups according to diagnoses and treatment, and hospitals receive the same reimbursement for cases within each group, with supplementary (reduced) payments for longer (shorter) hospital stays (Bachner et al. 2018). Additionally, the data include expenditures for prescription drugs, as well as most health-care expenditures covered by public health insurance. An important exception is visits to a hospital's outpatient departments, which, although primarily designed for medical emergencies, can also serve as substitutes for physician visits (Bachner et al. 2018). We have data on the number of visits to outpatient departments for selected years, which we use in supplementary analyses.
Concerning hospital stays, the data include the diagnosis, following the 10th revision of the International Classification of Diseases (ICD-10), which we use to characterize patients’ health conditions. We differentiate between causes for hospital visits, following the World Health Organization's study of the global burden of disease (WHO 2008), which classifies diagnoses into the following three broad groups: injuries, non-communicable disease, and a residual category. We divide the residual category into maternal and perinatal conditions, as well as communicable conditions and nutritional deficiencies, because differences in fertility between groups may affect differences in conditions related to pregnancy and childbirth. Non-communicable diseases account for most of the observed health-care expenditures (see below); hence, we further analyze the most common conditions within this group.
We construct a dataset of annual health-care expenditures for the years 2005–2015 for individuals aged 18–64 years. The analysis is restricted to persons who were insured throughout the corresponding calendar year - that is, we exclude individuals with insurance breaks. We determine migration status on the first day of each calendar year to differentiate between three groups. Refugees are persons who were in the asylum process or had been seeking asylum in the past. Economic migrants are the residual group of all individuals with non-Austrian citizenship living in Austria who had never sought asylum, and the native population includes all individuals with Austrian citizenship and without any migration background. Although most people in the second category were employed, this group also included persons who had been in Austria for different reasons, such as education. 8 Since the ASSD starts at 1972, we observe the date marking immigrants’ first entry into the Austrian labor market and check if they held foreign citizenship before 2005. 9
We analyze recent migrants and refugees in their first five years in Austria and label the first full calendar year after arrival as year one. We focus on the first five years to provide information on refugees that arrived in recent years. Observations of migrants after five years are excluded from the data. In total, the dataset includes nearly six-million observations for more than 850,000 people. The majority of observations belong to the native population, but the data also contain 74,758 economic migrants and 9,771 refugees. Table A1 in the Online Appendix shows the large diversity in the origin regions of the two migrant groups. Among economic migrants, German citizens comprise the largest group in the sample (25.6%), followed by individuals from Hungary (10.2%) and Romania (8.9%). For refugees, the most frequent source countries were Russia 10 (18.0%), Afghanistan (14.2%), Syria (9.9%), and former Yugoslavia (7.2%). As mentioned above, the data also include information on refugees after the completion of the asylum procedure. Naturally, the share of asylum-seekers within the refugee group decreases with the time that refugees spend in the country, from (by definition) 100% in the first year to 85.5% in the second year and to 38.2% five years after arrival.
We use the same data in a supplementary analysis focusing on the time when asylum is granted. Because the data do not include information on the exact legal outcome of the asylum process, we infer legal status from the ASSD and assume that refugees residing in Austria who were employed or received social security benefits, after they permanently left the asylum process, were granted asylum. The group of refugees, therefore, also includes persons who only received subsidiary protection, which is granted for a limited term, after which refugees can apply for extension. Among asylum decisions in 2015, 41% included the granting of asylum, 7% were subsidiary protections, 30% were rejections, and in 23% of the cases, the process was stopped for various reasons (Statistik Austria 2016). For the analysis of legal status, we use observations up to five years before and after asylum was granted and exclude all refugees with an unclear status in 2016.
Differences in Health Care Expenditures
Descriptive Comparison
Table 1 shows descriptive statistics of the sample separated into natives, economic migrants, and refugees. Migrants were significantly younger than the native population, with the average age (across all observations) being 33.3 years for economic migrants, 31.9 years for refugees, and 39.5 years for natives. Additionally, males are overrepresented among refugees and economic migrants. Concerning average annual health-care utilization, economic migrants’ expenditures were substantially lower than those of natives. The observed difference holds for total expenditures, as well as for different expenditure components. The descriptive comparison between native and refugees reveals ambiguous results. Although both groups show similar values for physician fees and prescription drugs, refugees had substantially higher expenditures for hospital visits. If health conditions are considered separately, refugees’ higher expenditure is found in almost all diagnoses, with the largest differences in hospital stays in connection with maternal and perinatal conditions and mental disorders. Certainly, raw differences in expenditures can be influenced by differences in characteristics and regional variations in health-care use, which we allow in the regression analysis.
Descriptive Statistics of the Analysis Sample.
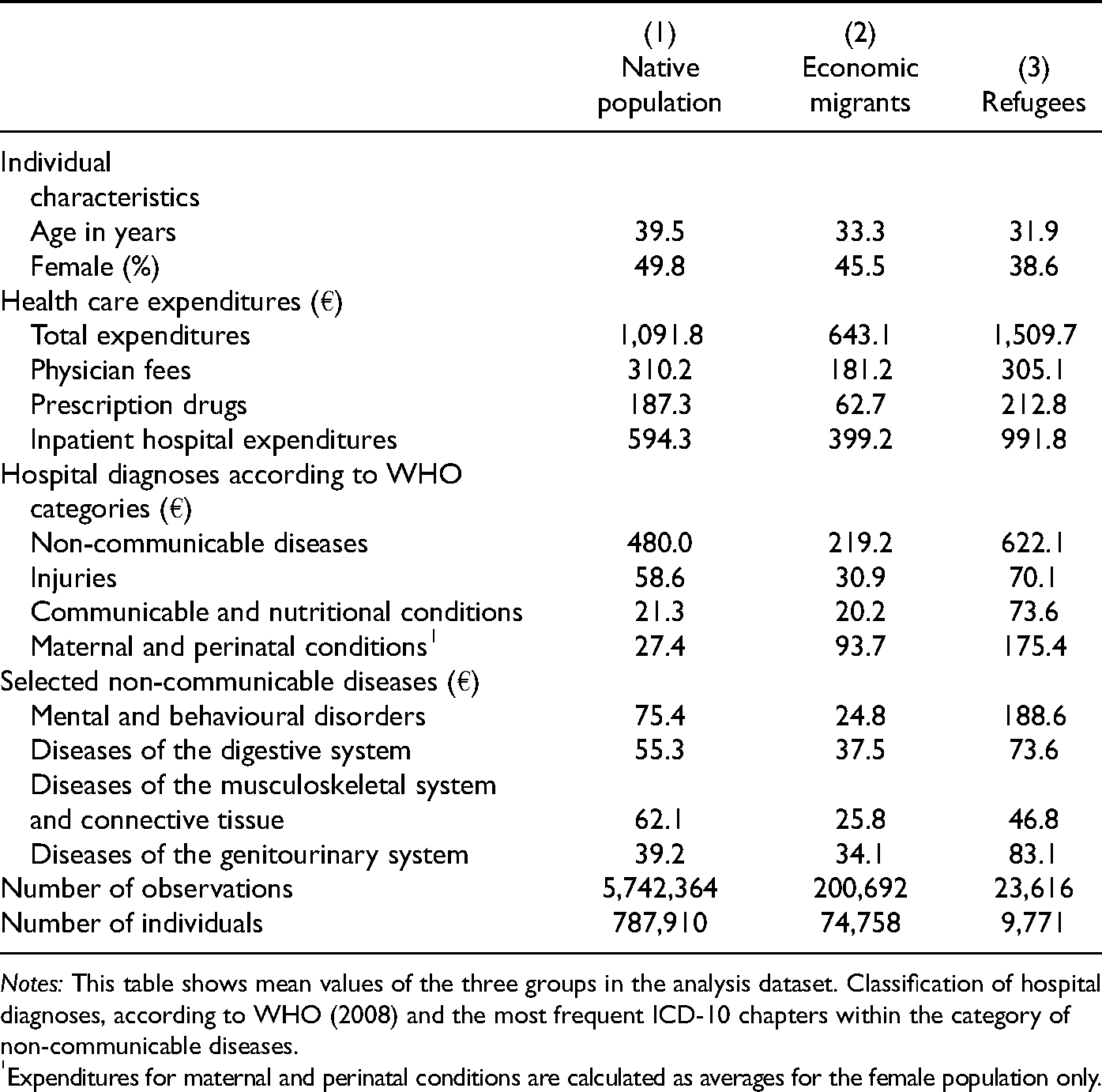
Notes: This table shows mean values of the three groups in the analysis dataset. Classification of hospital diagnoses, according to WHO (2008) and the most frequent ICD-10 chapters within the category of non-communicable diseases.
Expenditures for maternal and perinatal conditions are calculated as averages for the female population only.
Estimation Strategy
We compare health-care expenditures between migrants and natives by estimating the following model:
A further distinction is made between a simple repeated cross-sectional analysis of all migrants and a sample of migrants who stayed in Austria. In repeated cross sections, selective return migration or emigration to different countries may bias the development of outcomes over time (Riosmena et al. 2013; Abramitzky et al. 2014). For example, if migrants with a low health status are more likely to return to their home countries, an analysis of cross sections of migrants would mechanically indicate that their average health improves over time. We address this issue by estimating health-expenditure profiles for immigrants who stayed in the country for at least five years after arrival (“stayers”) and compare the results with the full sample of migrants in a repeated cross-section analysis.
Aggregate Expenditures
Table 2 summarizes the estimates of equation 1 for total annual health-care expenditures. Columns 1 and 2 show the results for the cross section and stayer sample of economic migrants. In the cross section, health-care expenditures in the first year after arrival were 204€ below those of natives of the same age and sex, which is 19% of the mean annual expenditures in the sample (1077€). In years two to five after arrival, the estimates also suggest economic migrants’ lower health-care expenditures, as the difference between natives and migrants varied between 146€ and 128€. Similar results are obtained using the sample of migrants who stayed in Austria for at least five years. Migrants’ expenditures in the first five years are between 58€ and 141€ lower than those of natives. Although the difference from the first to second year decreases in both samples, the point estimates do not reveal a clear pattern of convergence of health-care expenditures among economic migrants.
Health Care Expenditures of Migrants and Natives.
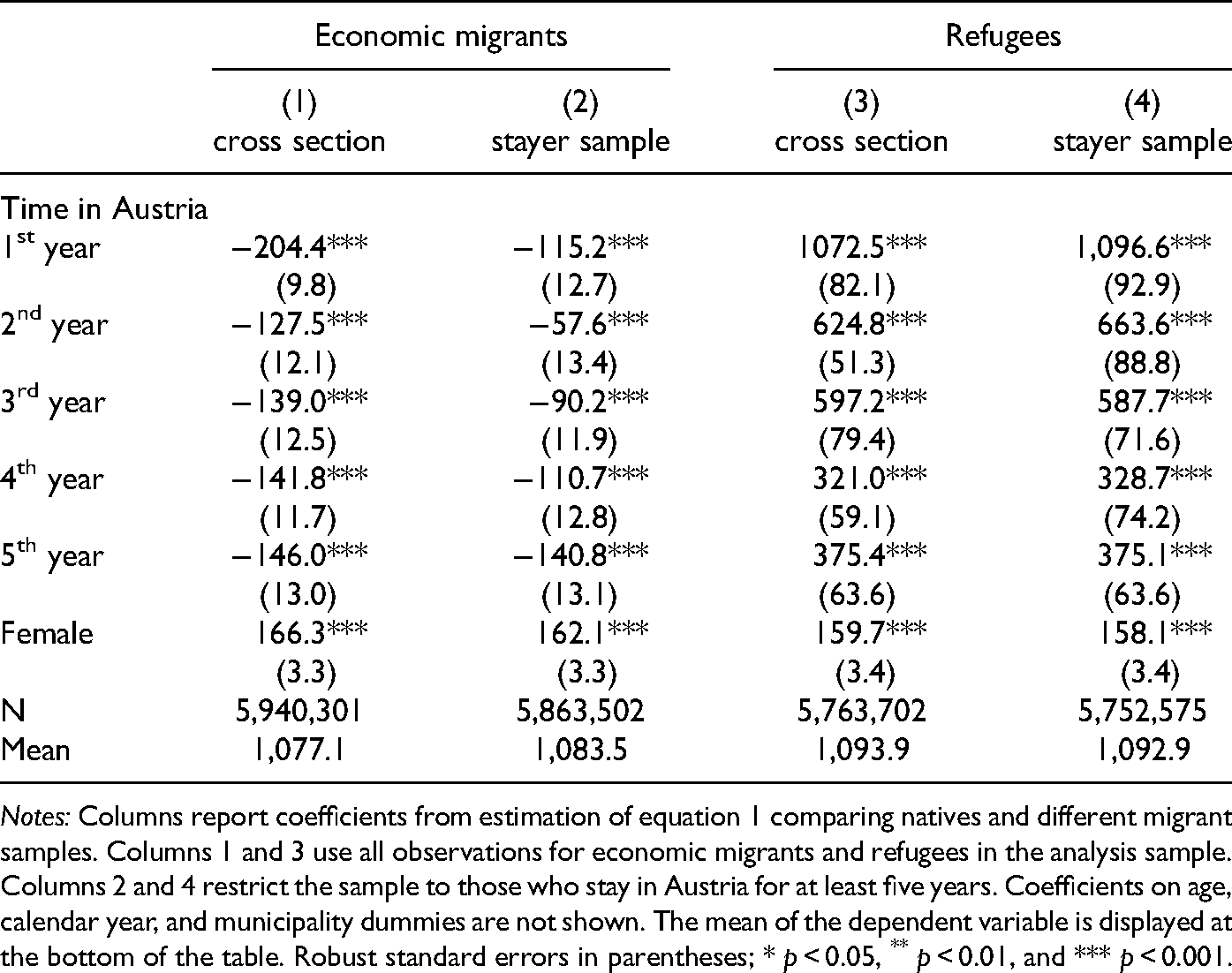
Notes: Columns report coefficients from estimation of equation 1 comparing natives and different migrant samples. Columns 1 and 3 use all observations for economic migrants and refugees in the analysis sample. Columns 2 and 4 restrict the sample to those who stay in Austria for at least five years. Coefficients on age, calendar year, and municipality dummies are not shown. The mean of the dependent variable is displayed at the bottom of the table. Robust standard errors in parentheses; * p < 0.05, ** p < 0.01, and *** p < 0.001.
The results are consistent with findings from other countries, which show migrants’ better health outcomes and lower health-care expenditures when compared to natives (e.g., McDonald and Kennedy 2004; Vargas Bustamante and Chen 2012). The limited evidence for convergence of expenditures may be attributed to analyzing only the first years after arrival. Compared to the stayer sample of economic migrants, we find even lower expenditures for the full sample of economic migrants. A plausible explanation for this finding is a correlation between mobility and health among economic migrants. In other words, migrants with lower health-care expenditures were more likely to emigrate again in the first five years after moving to Austria.
Columns 3 and 4 present the results for refugees. In contrast to the pattern for economic migrants, the estimates show refugees’ significantly higher health-care expenditures when compared to natives. In the cross section, the difference in expenditures in the first year is estimated to be 1073€. In the following years, the difference decreases substantially but remains statistically significant at 375€ in the fifth year in Austria. Similar results are obtained using the sample of refugees who stayed over five years, with slightly smaller differences in the first year after arrival and slightly higher differences in the following years. 11
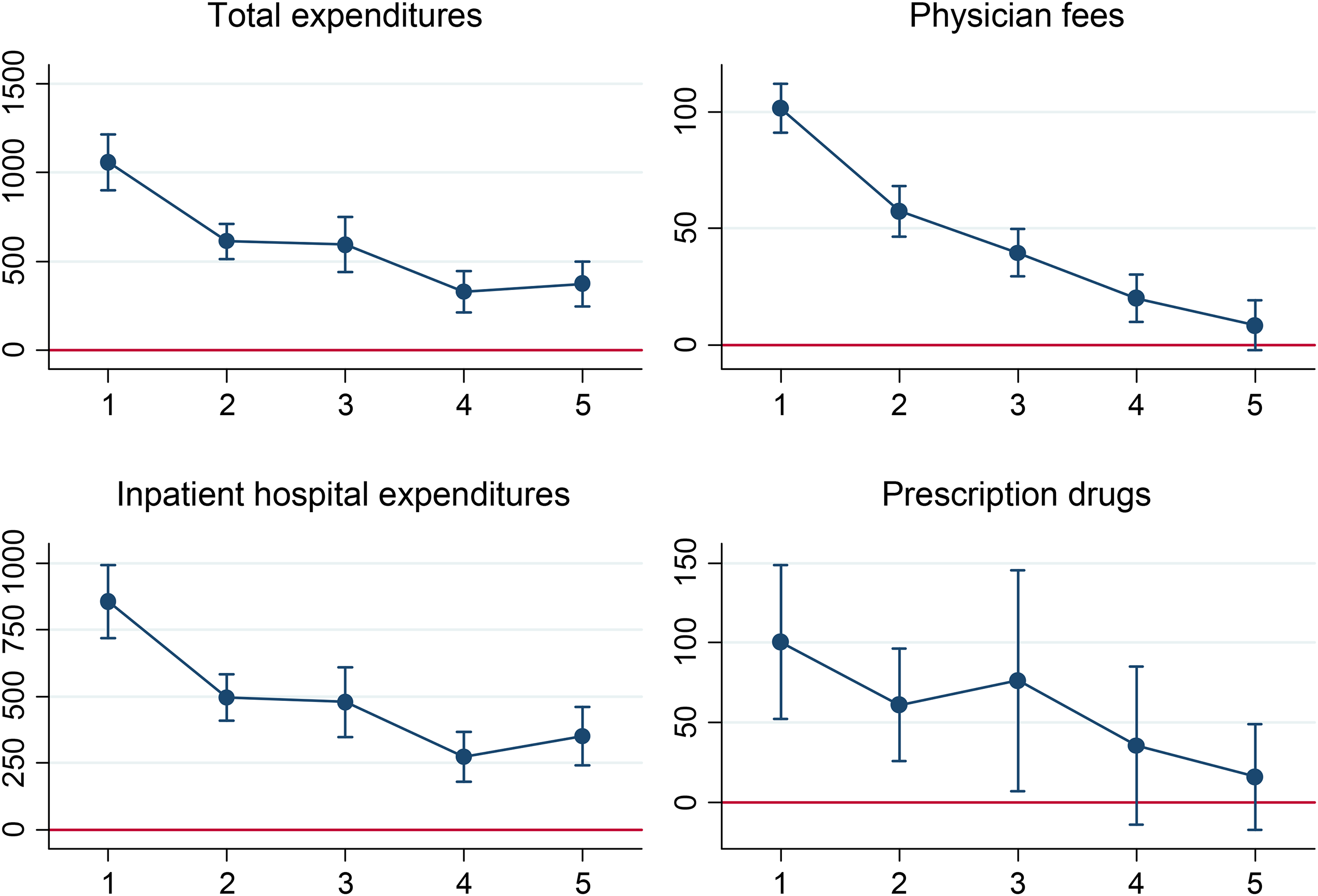
Refugees’ Relative Expenditures for Different Health Care Services. The Graph Plots Point Estimates and 95% Confidence Intervals of equation 1, Comparing the Health Care Expenditures of Refugees and Natives. See Table A5 for Estimation Output.
Figure 1 graphically illustrates the estimation results for refugees and displays estimates when we decompose total health-care expenditures into their components and analyze physician fees, prescription drugs, and hospital stays separately. 12 In the first year after arrival, the results reveal higher expenditures for all three health-care resources. The point estimates (see Table A5 in the Online Appendix for the estimation output) suggest the largest difference concerning expenditures in case of hospitalization, with higher expenditures of 866€ for refugees. Over the period of five years, the results point toward a convergence of observed expenditures. The estimated difference decreases substantially for all health-care resources and becomes statistically insignificant for physician fees and prescription drugs until the fifth year.
Results are very similar when we restrict the analysis to refugees who stayed in Austria for over five years (see Table A7 in the Online Appendix for estimation output). In general, comparing the results of the cross section and stayer sample does not indicate any correlation between refugees’ health state and migration to different countries (including voluntary departures and deportations). Therefore, we continue with the full sample of refugees in the remaining analysis because of the larger sample size and increased precision of the estimates.
Health Condition and Refugee Characteristics
Expenditures for hospital treatment account for a large part of total expenditures, and we observe the largest difference between refugees and natives for this type of health care. Therefore, we examine causes for hospitalizations by separately estimating equation 1 for groups of hospital diagnoses. Figure 2 summarizes the results. Refugees had significantly higher expenditures for communicable conditions and nutritional deficiencies, including infectious diseases such as pneumonia, tonsillitis, and tuberculosis, with point estimates ranging between 84€ and 36€. For women, we analyze expenditures related to maternal and perinatal conditions, wherein we again find substantially higher expenditures for refugees than for natives. This difference may be partly explained by higher levels of fertility among the refugee population. Conversely, the results do not indicate a statistically significant difference for expenditures related to injuries. The quantitatively relatively small differences in communicable diseases are evidence that refugees do not pose a serious health risk to the general population. Refugees receive a first medical examination at the initial reception center, where they also receive tuberculosis screenings (AIDA 2019), which may contribute to the small difference regarding communicable diseases.
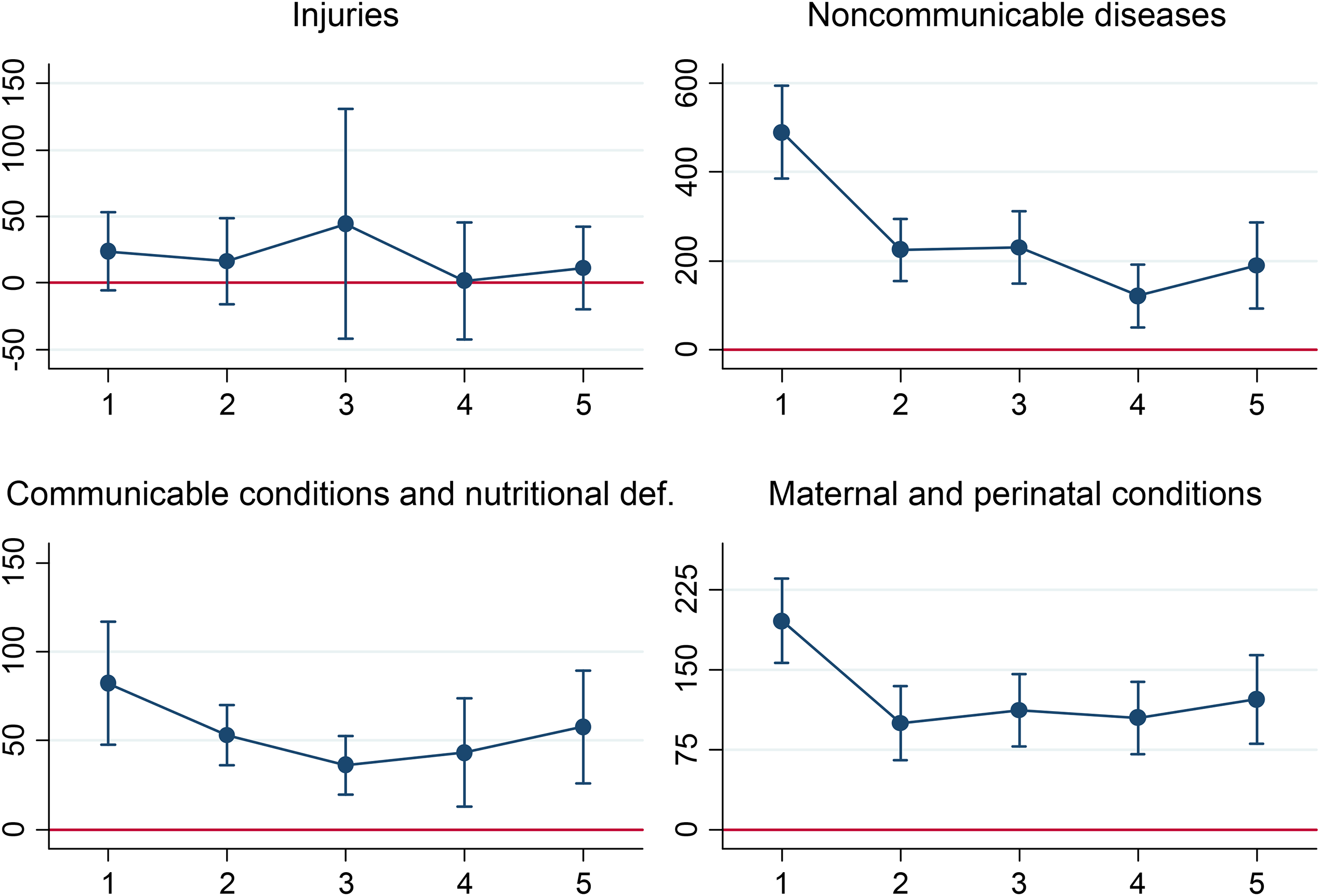
Refugees’ Relative Expenditures for Different Hospital Diagnoses. The Graph Plots Point Estimates and 95% Confidence Intervals of equation 1, Comparing the Health Care Expenditures of Refugees and Natives. See Table A9 for Estimation Output.
We further analyze the most frequent ICD-10 chapters within the group of non-communicable conditions because this group is responsible for most of the observed hospital stays (see Table A8 in the Online Appendix for the detailed incidence rates). Figure 3 shows that during the first year, refugees had substantially higher expenditures for all analyzed health conditions, with the largest difference seen for hospital visits related to mental and behavioral disorders wherein the estimates suggest higher expenditures of 155€. This result is consistent with existing evidence, which suggests high prevalence rates of mental-health issues among refugees (Lindert et al. 2009). Over time, the point estimates indicate a decrease in expenditures for mental disorders. After five years, refugees’ expenditures for mental disorders are 67€ higher than those of the native population. For diseases of the digestive system, musculoskeletal system, and connective tissue, however, results show that after five years, refugees’ expenditures were not statistically different from those of natives. Conversely, we do not find a pattern of convergence of expenditures for diseases of the genitourinary system, that is, diseases that affect organs of the reproductive and urinary systems. For all health conditions, we observe the largest difference in the first year after arrival. Although the gap in expenditures decreased over time and indicates a convergence in the long run, refugees’ health-care expenditures did not reach native levels within five years.
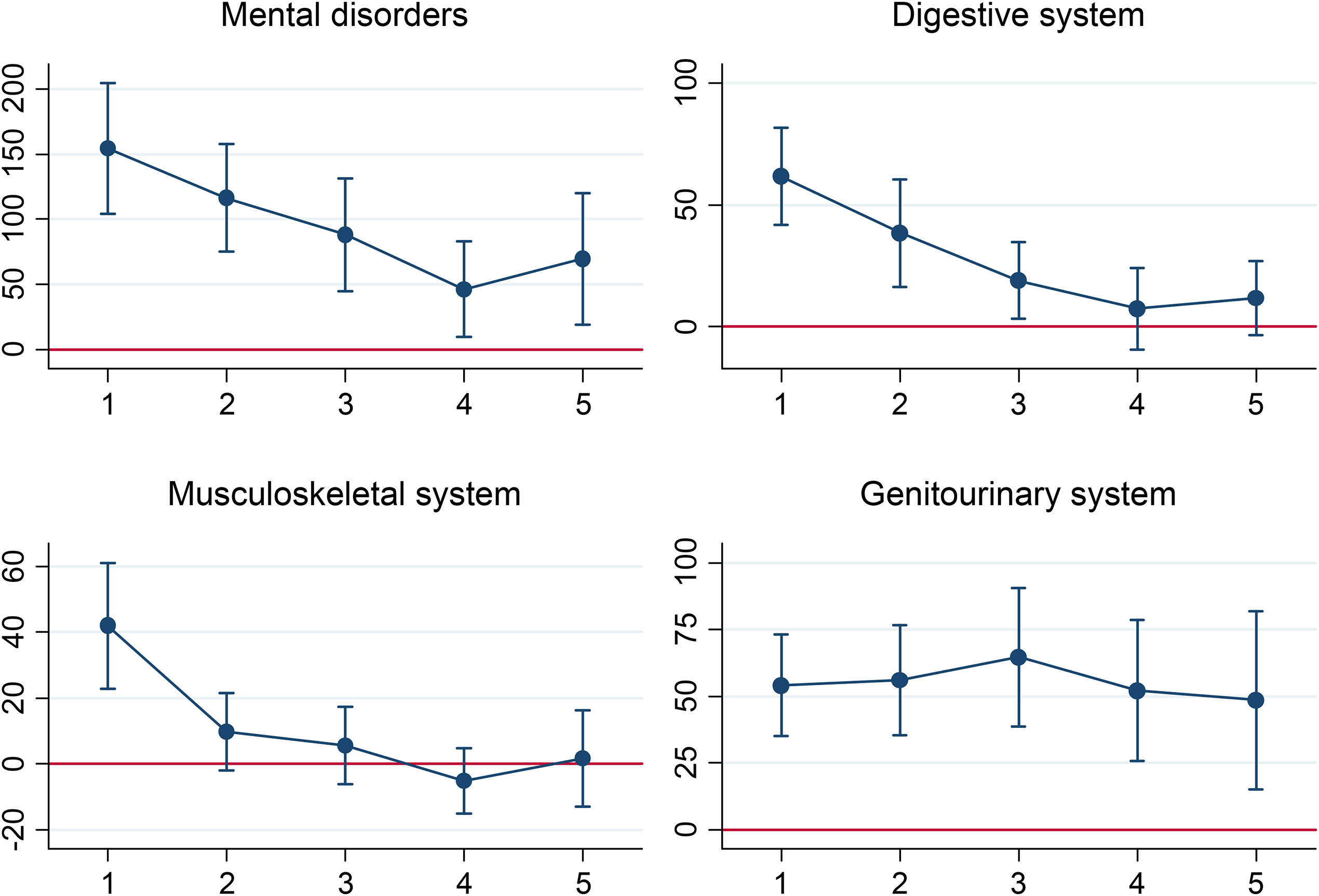
Refugees’ Relative Expenditures for Selected Non-Communicable Diseases. The Graph Plots Point Estimates and 95% Confidence Intervals of equation 1, Comparing the Health Care Expenditures of Refugees and Natives. See Table A10 for Estimation Output.
Additionally, we disaggregate refugees by the outcome of the asylum process, that is, refugees who at some point in time received asylum and those who did not. Estimation results are presented in Figure 4. We find a continuous decline in the differences of expenditures for refugees who received asylum, whereas among refugees who were not accepted by the end of 2016, large differences remained. In both samples, we find similar expenditure patterns in the first years, with large differences in comparison to natives in the beginning (959€ and 961€, see Table A12) and decreases in the subsequent two years. Among refugees who have not been granted asylum, the point estimates suggest an increase in expenditures after three years. Due to the small size, however, the estimates are relatively imprecise. The results indicate that legal status has an important influence on health-care expenditures, as we analyze in greater detail in the next section. 13
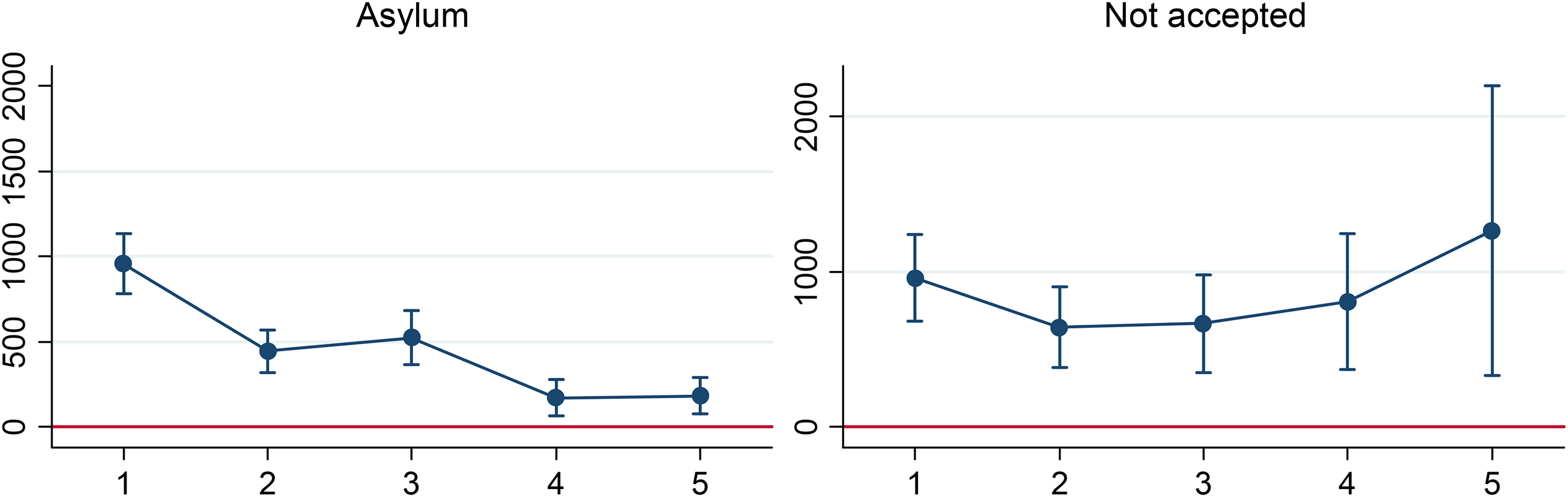
Refugees’ Relative Expenditures With Respect to Legal Status. The Graph Plots Point Estimates and 95% Confidence Intervals of equation 1, Comparing the Health Care Expenditures of Refugees and Natives. See Table A12 for Estimation Output.
Legal Status and Health Care Utilization
In many countries, migrants’ legal status affects access to social services and health care (Rechel et al. 2011). In the United States, for example, many immigrants with non-permanent statuses are not eligible for health-care benefits through the Affordable Care Act (Waters and Pineau 2015). Refugees in Canada often only have access to temporary health insurance that covers only urgent and essential needs (McKeary and Newbold 2010). Such barriers could have long-term effects on immigrants’ health and successful integration into society.
As outlined in Section 2.4, refugees are integrated into the Austrian social security system and have the same access to health-care services as the general population. Legal status, however, could still affect health-care utilization in different ways. During the asylum process, refugees are typically housed in special asylum shelters. Staff at these shelters provide refugees with support and counseling, which can include advice concerning when and where to seek health care (Koppenberg 2014). Refugees lose this support if they are granted asylum and leave shelters. At this point in time, many refugees also change their place of residence and are inclined to move to urban centers in Austria (Galera et al. 2018). When they are still in the asylum process, refugees are also exposed to uncertainty as to whether their application will be granted. This unsettled situation may affect health and health-care utilization levels, for example, if refugees address health-care needs more quickly for fear of deportation.
Estimating Equation
To investigate the role of legal status in health-care utilization, we run additional regressions focusing on the effect of granting asylum. We center the observations of all refugees on the year of asylum recognition and examine the expenditure relative to that time by estimating the following model:
Of course, granting asylum is not an exogenous event, and not all refugees reach this status. Consequently, we focus on refugees who received asylum to mitigate this potential source of bias. However, there could also be time-varying confounding factors - that is, unobserved variables may affect health-care utilization and the asylum decision. Many refugees change their place of residence after being granted asylum, when they must leave the asylum shelters (Dellinger and Huber 2021). We, therefore, restrict the sample to refugees whom we observed before and after the asylum decision to avoid a potential bias introduced by selective migration within Austria. A further limitation is that we do not observe the same set of refugees over all years, and changes in the composition of refugees may affect the estimated effects. Despite these caveats, this method allows an alternative descriptive view of the development of expenditures over time.
Results
Figure 5 presents the results for the main health-care expenditure outcomes. During the asylum process (equation 2, from r = −4 to r = 0), total expenditure, inpatient hospital expenditure, physician fees, and expenditures for prescribed drugs were significantly higher for refugees than for the native population. The point estimates indicate differences in total expenditure up to 928€ (see Table A14 in the Online Appendix). For total and hospital expenditures, results reveal decreasing expenditures already before the asylum process (from −2 to 0). With the receipt of asylum, however, expenditures decreased markedly for all outcomes, and the differences compared to the native population became insignificant for all types of expenditure, beginning with the third year after the positive decision. 14
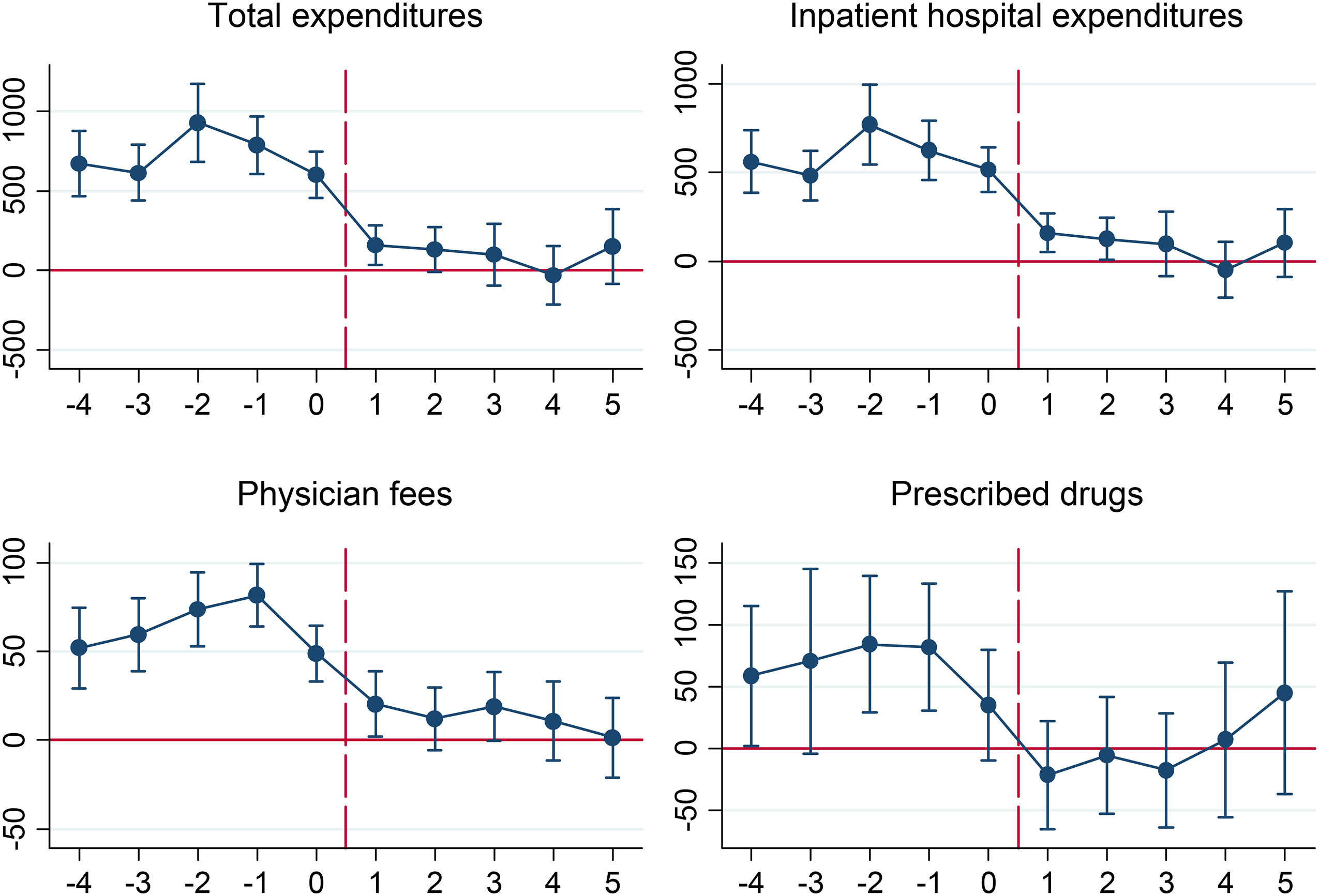
The Graph Plots Point Estimates and 95% Confidence Intervals of equation 2, Comparing the Health Care Expenditures of Refugees and Natives Relative to the Year of Receiving Asylum. See Table A14 for Estimation Output.
The estimates suggest a strong effect of legal status on the level of health-care utilization. On average, refugees in this sample received a positive decision on their asylum application during their third year in Austria. The previously observed trend of decreasing differences between refugees and natives with each additional year of residence can, therefore, be attributed, at least partially, to the positive change in legal status. Granting asylum has a number of consequences that can affect health-care utilization. Official recognition of the need for protection and permission to remain in the country is likely to have positive effects on refugees’ (psychological) well-being. At the same time, refugees typically must leave the asylum shelters and find new accommodation, while also being allowed to enter the labor market or apply for social security benefits if they do not find employment. Since these changes occur at the same time, it is difficult to distinguish to what extent they contribute to the reduction in health-care expenditures.
Determinants of Health Care Utilization
A large body of literature studies the determinants of health-care utilization in the general population and has documented widespread variations in health-care utilization both across and within regions (e.g., Chandra et al. 2011; Skinner 2011). Explanations for observed differences in health-care utilization have been linked to demand-side factors, such as prices, income, preferences, and health-care needs, or supply-side factors, such as supplier-induced demand and practice styles (Chandra et al. 2011; Skinner 2011; Ahammer and Schober 2020). Recent evidence also suggests that social interactions can have a significant impact on various dimensions of health, including risky health behaviors, obesity, and preventive health-care utilization (Fletcher 2014; Pruckner et al. 2019). Peer effects indicate that information, norms, or attitudes are transmitted among friends, family members, or other social networks and that such a social influence may be more relevant for migrants who are new to a country and not familiar with the existing health-care system (Devillanova 2008). Accordingly, Åslund and Fredriksson (2009) and Markussen et al. (2013) find sizable peer effects in welfare use and social insurance claims among refugees and migrants in Sweden and Norway.
In the Austrian health-care system, the influence of income and prices on health-care utilization is limited because of public insurance and price regulations (Bachner et al. 2018). We, therefore, focus the analysis of the determinants of health-care utilization on physician supply and the role of social networks. Results in the previous sections suggest that refugees’ substantially higher health-care expenditures in the first years after arrival, compared to natives, are predominantly driven by hospitalizations. Among the general population, existing evidence indicates that limited access to primary care may increase hospitalizations (Rosano et al. 2012). This relationship could be even more relevant for refugees, who are unfamiliar with the health-care system and, hence, potentially strongly affected by a lack of primary health care. Accordingly, we test how variables indicating the local accessibility of (primary) care affect refugees’ health-care expenditures. As argued in Section 2.3, refugees are quasi-randomly assigned to Austrian municipalities, where they receive basic welfare support. Therefore, this placement is largely exogenous with respect to their health-care needs and preferences, avoiding usual concerns related to residential sorting.
Estimating Equation
We explore determinants of refugees’ health-care utilization by estimating
Nit is a vector of social network variables for which we include the average level of health-care expenditures of refugees, 15 economic migrants, and natives within the municipality. When we analyze the different expenditure components, we use the average values of the corresponding health-care services as covariates. Additionally, we use a set of control variables Xit, including an individual's age, sex, origin region, and time spent in Austria. In this analysis, we only use data from refugees during the asylum procedure because, after asylum is granted, refugees may move to another place to get access to better employment opportunities or for other reasons.
Descriptive statistics of explanatory variables, at a municipality level, are presented in Table A16 in the Online Appendix and show significant variation in characteristics of the local health-care sector. There are hospitals in 8% of the refugee municipalities. The average number of general practitioners (specialists) per 1,000 insured individuals was 1.62 (0.49), with a standard deviation of 1.13 (1.12). In general, individual levels of health-care utilization can be expected to vary significantly, due to differences in health status and health-care needs, but there is also large variation among municipalities. For example, natives’ average total health-care expenditures ranged from 475€ in the municipality with the lowest average spending to a maximum value of 2,386€. For all categories of health-care expenditures, we observe the greatest variance among refugees, followed by economic migrants and natives. A plausible explanation for this pattern is that the number of observations of refugees and migrants per municipality was significantly smaller than for natives.
Results
Table 3 summarizes the estimation results of equation 3. The results do not indicate an important influence of the local health-care sector on overall resource use. Neither the density of GPs, who are predominantly responsible for primary care, nor the density of specialists had a statistically significant effect on total health-care expenditures. Likewise, we do not find significant effects for the different components of expenditures. Most notably, for hospitalization expenditures, the point estimates for physician density are positive but not statistically significant, indicating that variation in access to primary care does not explain hospital expenditures among our sample of refugees.
Determinants of Health Care Expenditures.
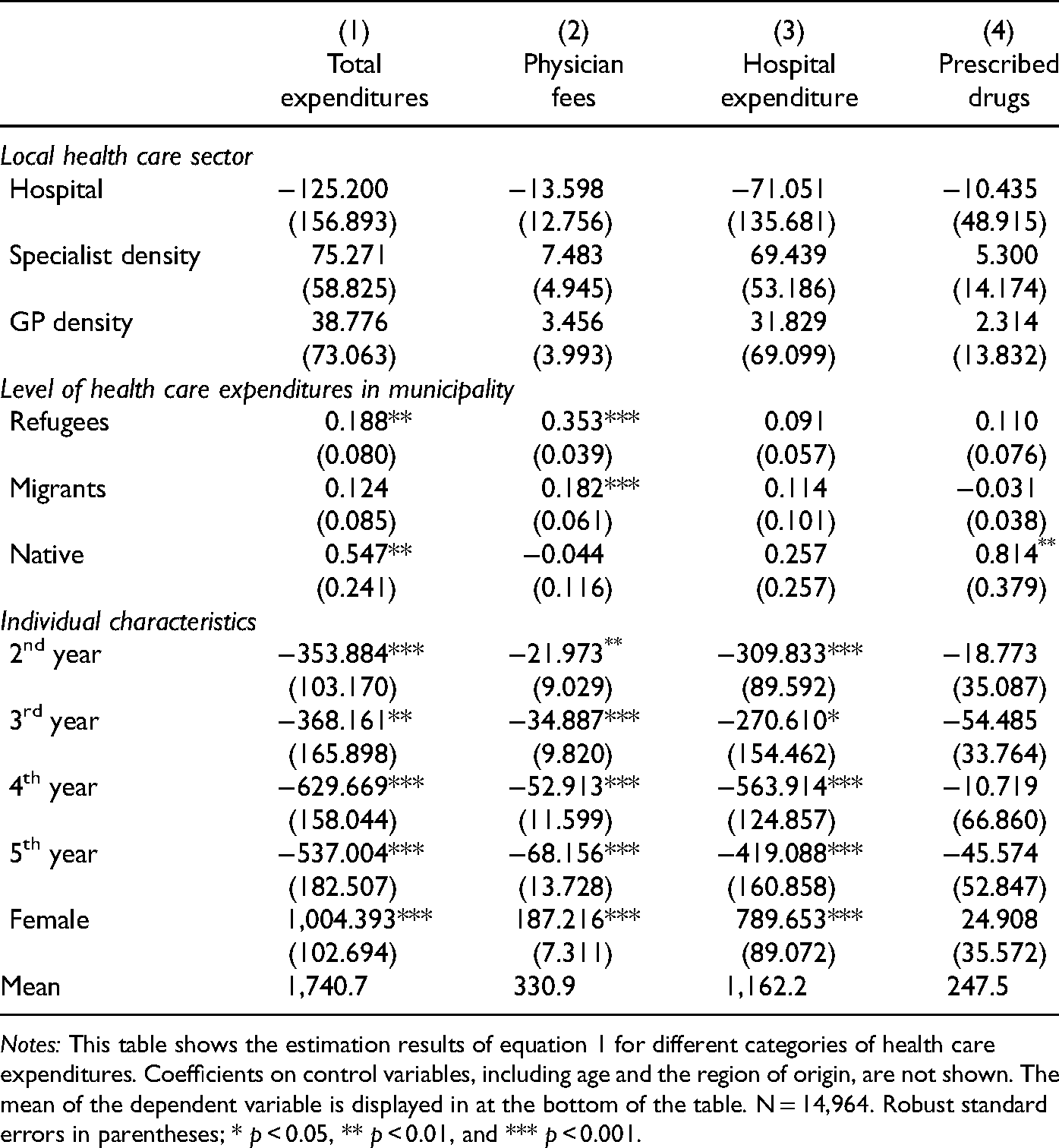
Notes: This table shows the estimation results of equation 1 for different categories of health care expenditures. Coefficients on control variables, including age and the region of origin, are not shown. The mean of the dependent variable is displayed in at the bottom of the table. N = 14,964. Robust standard errors in parentheses; * p < 0.05, ** p < 0.01, and *** p < 0.001.
Considering the expenditure levels, we find that an individual refugee's total health-care expenditures were positively correlated to the level of expenditure of other refugees in the municipality. The point estimate suggests that an increase of 1€ in average expenditure is associated with a 0.19€ increase in individual expenditure. An analysis of health-care services suggests that this effect is largely explained by the correlation of expenditures for physician visits among refugees. We also find that refugees’ physician visits were positively related to economic migrants’ expenditures in the municipality but that this effect was smaller and that there was no significant effect on total expenditures. Conversely, refugees’ total expenditures were also positively associated with natives’ expenditures in the municipality, and the results suggest that this effect is driven by prescribed drugs. Overall, we find smaller effects on expenditures for hospitalizations than for physician fees and drug prescriptions, which can be attributed to the fact that physician visits and prescriptions are more dependent on individual health-care preferences, while hospital stays are strongly related to (objective) health-care needs; hence, the influence of other factors is limited.
Similar results regarding the positive correlation of health-care service utilization have been documented for migrants in Canada (Deri 2005). Additionally, existing evidence from Italy suggests that social networks affect undocumented migrants’ health care (Devillanova 2008). Our empirical findings are consistent with the assumption that individual behavior is influenced by one's social network. However, even in (quasi-)random settings, the identification of causal peer effects is challenging (Manski 1993; Angrist 2014). Shared influences, such as NGO employees or volunteers who support refugees during the asylum procedure, may influence health-care expenditures of all refugees in a municipality. These persons can advise refugees on when and where to seek health care or even accompany them to physician visits. Unfortunately, the data do not hold information on the exact care and support that refugees receive outside the health system in Austria. Similarly, the positive correlation of expenditures for prescription drugs between refugees and natives could be related to variation in practice styles between municipalities - that is, differences in physicians regarding the appropriateness of medical care.
Conclusion
This article presents a comprehensive analysis of refugees’ health-care expenditures in Austria in three dimensions. In the first part, we investigated disparities in health-care utilization among migrants and natives, using administrative data and use information on asylum status to differentiate between economic migrants and refugees. The results indicate distinctly different patterns between the two groups. In accordance with the existing literature on the healthy immigrant effect (e.g., Antecol and Bedard 2006), economic migrants had lower health-care expenditures than the native population. Conversely, we find substantially higher expenditures for refugees, particularly in the first year after arrival. These finding are consistent with epidemiological studies documenting high prevalence rates of disorders among refugee groups (e.g., Clark and Mytton 2007). In addition, our results indicate a convergence of expenditures over time; however, a statistically significant difference between refugees and natives remains for most analyzed health outcomes and refugee groups over a period of five years. A limitation of the data is that we only observe health-care utilization, not the true health status or well-being of insured persons. Individuals may have unmet health care needs that do not appear in the data.
In the second part, the observed long-run convergence of expenditures between refugees and natives is supported with additional results focusing on refugees’ legal status, which show that expenditures for inpatient and outpatient treatments, as well as for prescribed drugs, decreased markedly after a positive asylum decision. Three years after the decision, there were no statistically significant differences in expenditures compared to natives. In contrast, for refugees who did not have a positive asylum decision even in the fifth year after arrival in Austria, health-care expenditures remained at an unchanged high level. These results are particularly noteworthy because, in contrast to other studies, 16 formal access to the Austrian health-care system did not change with the observed legal-status change. From this perspective, the results on the reduced health-care expenditures may be attributed to refugees’ potentially lowered psychological stress of being granted asylum and to the numerous new rights which accompany a positive asylum decision. Once granted asylum, refugees can move freely in Austria and gain formal full access to the labor market. However, they may also lose counseling related to health care when they must leave the asylum shelters, due to the positive asylum decision. From a health policy perspective, policy-makers should place a particular focus on the transition period after the granting of asylum. Our novel finding of a marked decrease in health-care expenditures implies, on the one hand, a lower financial burden on the public health-care system and, on the other hand, negative long-term effects on refugee health if this decrease comes at the cost of inadequate health care.
In the third part of our article, we show that the local health-care sector's characteristics did not have a significant effect on refugees’ health-care expenditures, indicating that the large health-care expenditures among refugees are not a result of insufficient supply of (primary) health care. Instead, a plausible explanation is that health-care needs are higher for refugees than for natives and economic migrants, especially in the first years after arrival. Additionally, refugees may face other barriers to health care that could impede adequate access and affect health status and utilization levels, including lack of information on the health-care system, language issues, cultural differences, or (hidden) costs such as co-payments for specific services (Mangrio and Forss 2017; Kohlenberger et al. 2019). We compare expenditures in a publicly funded health-care system with near-universal coverage, as it exists in many European countries (OECD 2013). Although the results cannot be generalized to countries with different health systems, additional barriers to health care may exacerbate initial inequalities in health, if refugees’ health status deteriorates because of unmet health care needs.
Our findings highlight the importance of distinguishing between migrant groups in the analysis of health-care utilization. In Central Europe, the discussion about migrants’ health-care utilization has been mostly limited to migrant access to the health-care system and the impact of this access on individual health status (e.g., Jaschke and Kosyakova 2021). We find that even with equal formal access, there are differences in health-care expenditures between the native population and different migrant groups. Future research should, therefore, investigate which factors affect the observed health expenditures differences between natives and asylum-seekers. In particular, such work should explore whether migrants’ reasons leaving the home country (e.g., armed conflicts) and type of movement to the host country (e.g., taken route, involvement of smugglers, and physical challenges on the flight), as well as receiving countries’ migration policies (e.g., labor market access), are relevant for migrants’ health status and, thus, health expenditures on migrants in the host country. In addition, attention should be paid to the period around the asylum decision itself. Although we see a large reduction in health-care utilization in the case of a positive asylum decision, it is unclear whether this pattern can be explained by change in health status and whether these health-care expenditure changes are also observable in other countries.
Acknowledgments
For helpful comments and discussions, we would like to thank Gerald J. Pruckner, participants of the 2017 Conference of the International Health Economics Association (Boston), the 2018 Annual Meeting of the German Society for Health Economics (Hamburg), the 2018 Conference of the European Health Economics Association (Maastricht) and the 2018 Annual Meeting of the Austrian Economic Association (Vienna). The financial support by the Austrian Economic Association, the Austrian Federal Ministry for Digital and Economic Affairs and the National Foundation for Research, Technology and Development is gratefully acknowledged.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Austrian Economic Association, the Austrian Federal Ministry for Digital and Economic Affairs, and the National Foundation for Research, Technology and Development.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.