
Abstract
Comparative histomorphological assessment of local response to implanted reference biomaterial, also called biocompatibility testing/evaluation, in an appropriate animal model is a widely practiced safety evaluation procedure performed on biomaterials before clinical use. Standardized protocols and procedures, originally designed for testing synthetic materials, available for the testing/evaluation do not account for the immunogenic potential of a candidate biomaterial. Therefore, it is appropriate to supplement the routine biocompatibility test reports with adjunct data that may provide insight into the immunogenic potential of candidate biomaterials, especially when testing biomaterials that are derived from mammalian sources. This article presents expanded safety evaluation data of a porcine cholecyst–derived scaffold (CDS) intended as a xenogeneic graft. The biocompatibility was tested in rat subcutaneous model in comparison with a reference material and the CDS was found biocompatible. However, when studied by immunohistochemistry and real-time reverse transcription polymerase chain reaction for the number and/or polarization of M1 macrophage, M2 macrophage, cytotoxic T-cell, helper T cell, TH1 cell, and TH2 cell, the CDS appeared to induce a differential local immunopathological tissue reaction despite the similarity in biocompatibility with the reference material. The adjunct data collected were useful for objectively assessing the safety of CDS as a xenograft.
Keywords
Introduction
Xenogeneic scaffold materials derived from mammalian organs/tissues are a class of biomaterials that are used as grafts for a variety of clinical applications including skin-wound healing, hernia repair, dural repair, and cardiac repair (Badylak, Freytes, and Gilbert 2009). These scaffolds are essentially extracellular matrices (ECM) of organs and tissues extracted after variable extent of decellularization. Porcine small intestinal submucosa is the widely used material of this kind. It has been used in more than 1 million human patients worldwide for treating a variety of diseases. Xenogeneic scaffolds prepared from dermis, pericardium, and facia lata are also beginning to be used for clinical applications (Badylak 2007). Cholecyst–derived scaffold (CDS) is a relatively novel biomaterial of mammalian origin (Burugapalli et al. 2007; Anilkumar et al. in press), which has potential clinical use for buttressing staples (Burugapalli et al. 2008), skin graft (Revi et al. 2013), and bladder repair graft (Kajbafzadeh et al. 2014). This article is about safety evaluation of CDS.
The nature of local tissue response around grafted biomaterials in appropriate animal models is a major indicator of safety of any candidate biomaterial. Robust protocols in the form of widely respected standards are available for evaluating the nature of such tissue reactions (Schuh 2008). For the evaluation, also called biocompatibility testing, usually the candidate biomaterial is implanted in animal models in an appropriate site such as bone, skeletal muscle, or subcutis, and the nature of the tissue reaction induced by the implant is compared with those induced by a reference biomaterial. The latter are generally biomaterial-grade products already in market or their raw materials (Anderson 2001). Indeed, respectable standard procedures such as ISO 10993-6 (2007) and USP 34-NF 29 <88> (2011) are used for the biocompatibility evaluation. These procedures were originally developed for testing materials, with known constituents and purity, which are usually synthesized in a laboratory. It is important to note that they are not designed for testing materials of biologic origin. However, these general procedures may pick up residual toxicity caused by chemicals (mostly detergents) used for processing and preparation of scaffold even in products of biological origin (Cebotari et al. 2010; Umashankar, Mohanan, and Kumari 2012).
Biomaterials of animal origin when used for clinical application pose several concerns. One of the critical issues about the use of animal-derived product for medical applications relates to its potential zoonotic disease transmission capability. This is highly relevant for medical graft materials prepared from mammalian organs/tissues. Therefore, defined disease surveillance procedures and appropriate sourcing of animal tissues have been recommended for addressing such concerns (Fishman, Scobie, and Takeuchi 2012; ASTM F2210 2010).
However, as documented in the database of “manufacturer and user facility device experience” (MAUDE, http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfmaude/search.cfm), it appears that most of the reported complications associated with the use of xenogeneic graft materials are related to immune function rather than the already addressed issues concerning zoonotic potential or biocompatibility. Therefore, an assessment of the immunotoxicological potential of candidate biomaterials has been suggested (Haley et al. 2005; ISO/TS 10993-20 2006). On closer examination, one finds that such immunotoxicologic test results provide insight into the nature of toxicity caused by the candidate biomaterial on the organs of immune functioning like spleen, lymph node, thymus, and lymphoid tissue. Although information about remote organ toxicity may be useful in assessing the functional status of the immune system, it may not give any impression about the specific nature of immunopathological reaction occurring around the xenogeneic graft. Moreover, the usefulness of assessing enhanced histopathology of the immune system (Elmore 2012) has not been investigated for testing biomaterials.
This article records the observations on the ability of a candidate biomaterial of porcine cholecystic origin to induce differential local immunopathological tissue response despite similarity in biocompatibility response with a reference material. The observation may have implication on the safety testing procedures adopted for evaluating animal-derived scaffolds used in regenerative medicine especially as xenografts.
Materials and Methods
Preparation of Scaffolds
Porcine CDS was prepared by a previously published nondetergent/enzymatic procedure for fabricating potential skin graft (Revi et al. 2013). Briefly, porcine organs were collected in a stabilizing agent (10% buffered formalin) and within 24 to 48 hr ECM beneath the mucosa was delaminated. It was washed thoroughly, lyophilized for 16 hr, sterilized by ethylene trioxide gas, and stored (Anilkumar et al. in press).
Wherever indicated, in the absence of any market product of cholecystic origin, a commercial small intestinal submucosa (CSIS) marketed by Cook Medical, Bloomington, IN, as BiodesignsTM Surgisis-1-layer tissue graft (C-SLH-1S-7x10) was used as the reference biomaterial.
Animal Implantation
The CDS and CSIS were implanted subcutaneously into Sprague-Dawley rats and biocompatibility was evaluated, with the approval of Institutional Animal Ethics Committee of the host institution as per national regulation. Briefly, 12 rats were anesthetized with intramuscular injection of Ketamin (70 mg/kg) and Xylazin (5 mg/kg) and the hair of the dorsum was clipped off. Animals were divided in to 2 groups for implanting CDS or CSIS. Under aseptic conditions, subcutaneous pockets were made on the dorsum and the materials (1 cm2 each) were folded and implanted (4 implants per animal) into the pockets. The incisions were closed with sterile sutures (3/0 mersilk, Ethicon Inc., UK). Two animals from each group were euthanized by excess CO2 gas inhalation after 1 week, 4 weeks, and 12 weeks post implantation. The implant with the surrounding tissue was collected from each site. Samples from 2 sites were used for the study and the other 2 were kept as back-up samples. Each sample was cut into 2 halves. The first half was fixed in 10% neutral buffered formalin for histopathology and the other was preserved in RNAlater (Sigma, St. Louis MO) at −20°C freezer for gene expression studies.
Histotechnology
Formalin-fixed tissue samples collected after the animal experiment were processed for routine histopathology using an automated tissue processor Leica TP1020 (Leica Biosystems, Germany) and embedded in paraffin wax. Tissue sections (4-μm thick) were made using Leica RM2255 microtome (Leica Biosystems, Germany) and stained with Harris’s haematoxylin and eosin (H&E; Electron Microscopy Sciences, Hatfield, PA).
Histopathology
Local tissue reaction induced by the CDS was evaluated as per ISO 10993 Part-6, and CSIS was used as the reference biomaterial. In each histology section, the following parameters were studied: number of inflammatory cells (neutrophils, plasma cells, lymphocytes, and macrophages), number of foreign body giant cells (FBGCs), severity of necrosis, extent of neovascularization, extent of fibrosis, and extent of fatty infiltration. Average semiquantitative score was then calculated as [(subtotal-I × 2) + subtotal-II], whereas subtotal-I is the sum of scores for neutrophil, lymphocyte, plasma cell, macrophage, giant cell, and severity of necrosis and subtotal-II is the sum of the scores for neovascularization, fibrosis, and fatty infiltration. The difference of the score for the test material from the reference material was designated as the irritancy score for CDS.
Immunohistochemistry
Immunohistochemistry was performed on histology sections for detecting subpopulations of macrophage and lymphocytes. Briefly, tissue sections were deparaffinized and washed in distilled water and treated with antigen retrieval buffer for 20 min at 92°C and allowed to cool for 30 min at room temperature. The endogenous peroxidase activity in tissues was inhibited by treating the slides with 5% H2O2 (Merck, India) for 15 min. Potential nonspecific reactivity of secondary antibody was blocked by incubating the sections with 10% goat serum for 30 min. Later, the sections were washed in trisodium citrate buffer (Merck, India) and treated with the primary antibody against M1 macrophage, CD80 (Rabbit monoclonal, clone EP1155Y, Abcam, UK; clone no longer available); M2 macrophage, CD163 (Mouse monoclonal, clone ED2, Santa Cruz Biotechnologies, Inc., Santa Cruz, CA); helper T-lymphocytes, CD4 (Mouse monoclonal, clone OX38, Millipore Corporation, Billerica, MA), or cytotoxic T-lymphocyte, CD8 alpha (Mouse monoclonal, clone OX8, Abcam, UK) for 1 hr at room temperature. The antigen–antibody binding was then detected using Supersensitive polymeric-HRPTM detection system (BioGenex Laboratories, Fremont, CA) according to manufacturer’s instructions. Finally, the sections were counterstained with Harris's haematoxylin (Electron Microscopy Sciences, Hatfield, PA).
Histomorphometry
Histomorphometry was performed on histology images (original magnification, 40×) captured with a DP71 camera loaded on to a BX51 microscope (Olympus Corporation, Japan) using ImagePro version 3DS6.1 software (Media Cybernetics, Silver Spring, MD). The microscope had an automated stage movement system. The implant tissue was imaged, frame by frame, through automation to obtain a series of images that covered the entire implant tissue. The number of images varied with the area occupied by the tissue reaction. The number of immunostained cells with phenotypic features of macrophages/lymphocytes in the reaction zone was counted manually. The area of the implant tissue was also estimated. The number of cells per mm2 was determined and the respective ratio was calculated.
RNA Isolation and Real-time Reverse Transcription Polymerase Chain Reaction
Following the animal experiment, tissue samples that were stored in RNAlater were ground in a tissue homogenizer (IKA, Germany) and total RNA was isolated using Trizol reagent (Invitrogen, Carlsbad, CA) as per manufacturer’s protocol. The purity and concentration of RNA were tested using NanoDrop ND-1000 spectrophotometer (NanoDrop, Wilmington, DE). One microgram of RNA was used for cDNA synthesis (superscript III reverse transcriptase enzyme, Invitrogen Corporation, Carlsbad, CA). The primer sets for Glyceraldehyde phosphate dehydrogenase (GAPDH) housekeeping gene, interferon gamma (INF-γ), interleukin-4 (IL-4), arginase-I, and inducible nitric oxide synthase (iNOS) were custom designed and obtained from Eurogentec (Belgium). PCR primer sequences are as follows: GAPDH forward: 5′-CAAGTTCAACGGCACAGTCAAG-3′; GAPDH reverse: 5′-ACATACTCAGCACCAGCATCAC-3′; iNOS forward: 5′-AAGAGACGCACAGGCAGAGG-3′; iNOS reverse: 5′-AGCAGGCACACGCAATGATG-3′; Arginase-I forward: 5′-GGCAGTGGCGTTGACCTTG-3′; Arginase-I reverse: 5′-GTTCTGTTCGGTTTGCTGTGATG-3′; INF-γ forward: 5′-AACCCACAGATCCAGCACAAAG-3′; INF-γ reverse: 5′-TT TCCGCTTCCTTAGGCTAGATTC-3′; IL4 forward: 5′-ACAAGGAACACCACGGAGAAC-3′; IL4 reverse: 5′-TTCAAGCACGGAGGTACATCAC-3′. Real-time PCR was carried out using qPCR MasterMix Plus SYBR® reagents (Eurogentec, Belgium). M1/M2 macrophage phenotypic polarization was studied by the ratio of gene expression of iNOS to that of arginase-I using the equation,
Statistical Analysis
One-way analysis of variance and Tukey-Kramer multiple comparison tests were performed using GraphPad InStat software for calculating the differences between groups. p value less than .05 was considered as significant difference.
Results
Routine Histopathology
The scaffolds appeared as pink stained thin strips of the material of variable thickness (<50 μm) embedded in the subcutaneous tissue (Figure 1), in histology sections. Both CDS and CSIS induced acute inflammatory reaction around the implants (Figure 1A and D; Table 1). There was also ingrowth of granulation tissue composed of proliferating fibroblast, mononuclear cell infiltrate, and neovascularization into the space between folds of the scaffold materials and at the tissue materials interface. Although few in number FBGCs were present in the implant tissue even in 1-week samples.
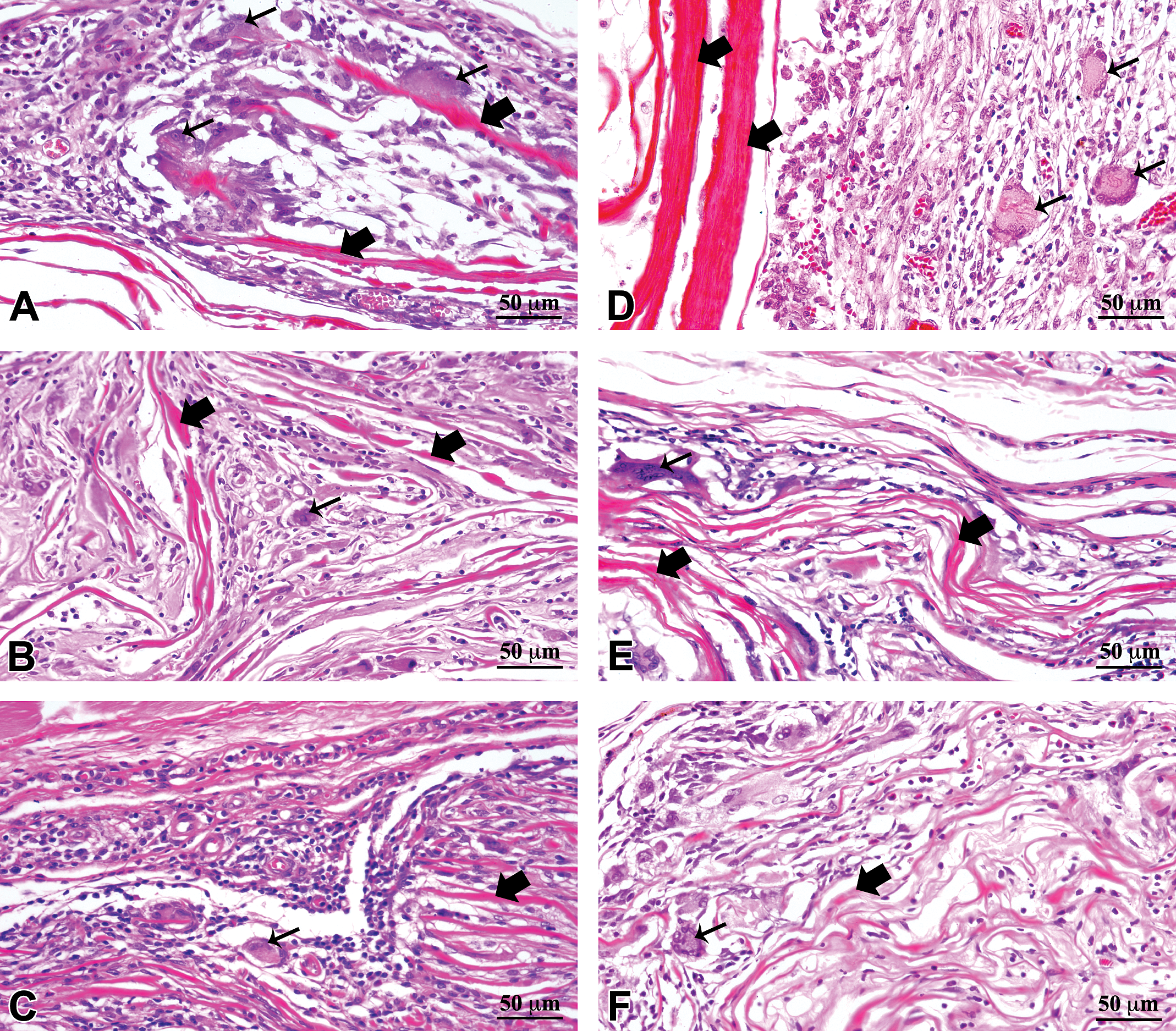
Histomorphology of the local response induced by commercial small intestinal submucosa (CSIS; A, B, and C) and cholecyst-derived scaffold (CDS; D, E, and F) implanted in subcutaneous tissue of rat at 1 week (A and D), 4 weeks (B and E), and 12 weeks (C and F). The scaffold and foreign body giant cells are shown by thick and thin arrows, respectively.
Quantitative and semiquantitative parameters studied for evaluating histopathology (parameters as per ISO 10993 part-6 2007).
Note. All values represent mean (n = 4) of the semiquantitative score of local tissue response as per ISO 10993 Part-6 (2007), local effects of implantation. CDS = cholecyst-derived scaffold; CSIS = commercial small intestinal submucosa.
aInflammatory cells: N, polymorphonuclear cells; L, lymphocytes; P, plasma cells; and M, macrophage. Gradings were based on the number and distribution of cells (0 = 0 no cell, 1 = 1–5 cells, 2 = 6–15 cells, 3 = heavy infiltration, and 4 = packed cells represented as average of 5 fields at magnification, 400×).
bGC (Giant cells): (0 = 0 cells, 1 = 1–2 cells, 2 = 3–5 cells, 3 = heavy infiltration, and 4 = packed cells represented as average of 5 fields at magnification 400×).
cSN (severity of necrosis): grading, determined by the presence of cell debris and inflammation; 0 = not present, l = minimally present, 2 = mild degree, 3 = moderate degree, and 4 = severe degree).
dNV (neovascularization): the extent measured as counts of the number of detectable vasculature under magnification of 400× (0 = no capillaries, l = l–3 capillaries, 2 = 4–7 capillaries, 3 = broad blood vessels, and 4 = extensive vascularisation).
eF (fibrosis): measured as thickness of fibrous capsule, under magnification of 400×, around the implant (0 = absent, 1 = <5 µm, 2 = 6–15 µm, 3= 16–30 µm, and 4 = >30 µm).
fFI (fatty infiltrate): grading determined by the amount of fatty tissue (0 = not present, 1= minimally present, 2 = mild degree, 3 = moderate degree, and 4 = severe degree).
By 4 weeks, the number of polymorphs had reduced and granulation tissue appeared to mature (Figure 1B and E; Table 1). The infiltration of mononuclear cells was higher compared to 1-week samples. There was moderate infiltration of FBGCs throughout the implant tissue. The scaffolds appeared to degrade, as indicated by the reduction in thickness of the implanted material. The degradation of CSIS was more compared to the CDS.
At 12 weeks, there was minimal acute inflammation for CDS-implanted tissues compared to the 1-week or 4-week samples. The number of macrophages and FBGCs was also relatively less in 12-week samples compared to the 4-week samples (Figure 1C and F; Table 1). The number of giant cells, the extent of neovascularization, and the extent of fibrosis were higher in the CDS-induced reaction compared to the CSIS-induced reaction, but the difference was not significant enough to cause appreciable variation in the calculated irritancy score between the 2 materials.
Biocompatibility Evaluation as per ISO 10993 Part-6
The semiquantitative parameters evaluated as per ISO 10993 Part-6 are summarized in Table 1, which indicated similarity in values of CDS and CSIS. The irritancy score for CDS was calculated against the CSIS. The score was zero at 1 week and 4 weeks of implantation. At 12 weeks, the score was 2.25. A score of less than 3 denoted biocompatibility similar to the reference material; therefore, the calculated irritancy score given earlier indicated that the CDS was a nonirritant material compared to the reference material CSIS.
Immunohistochemistry
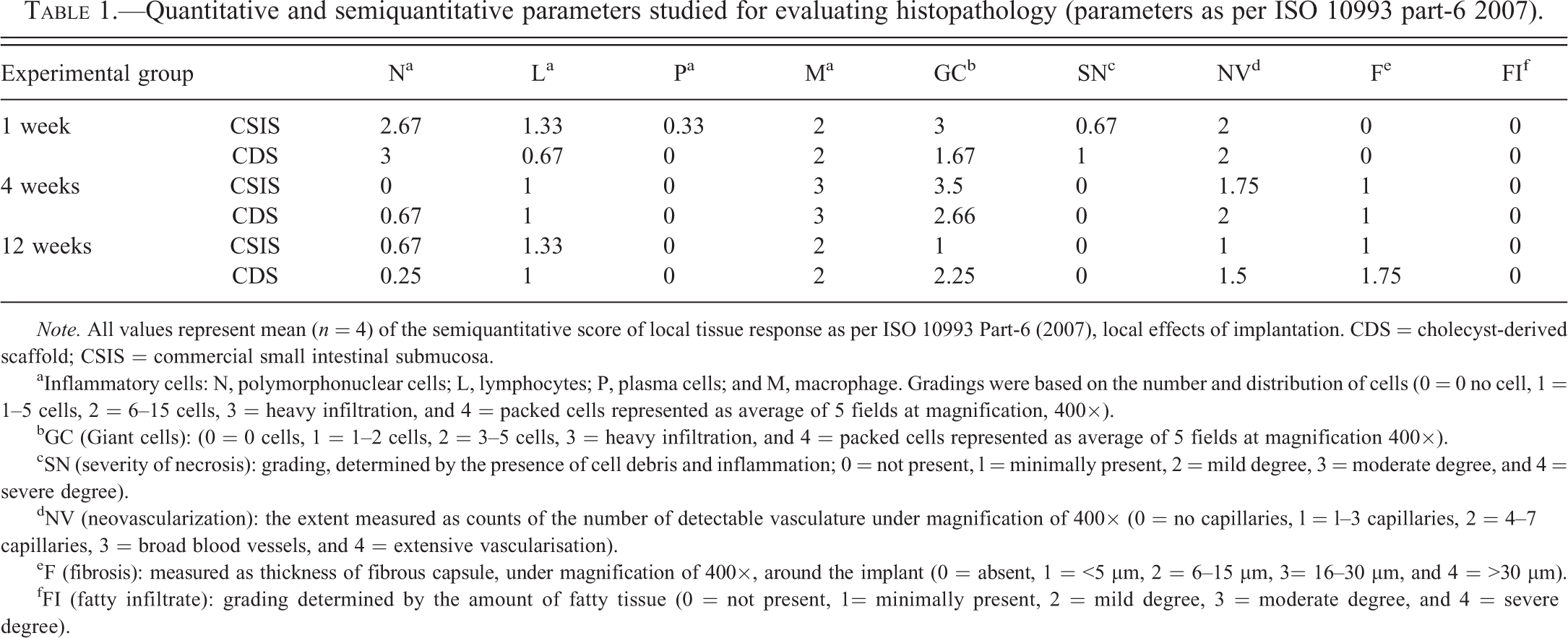
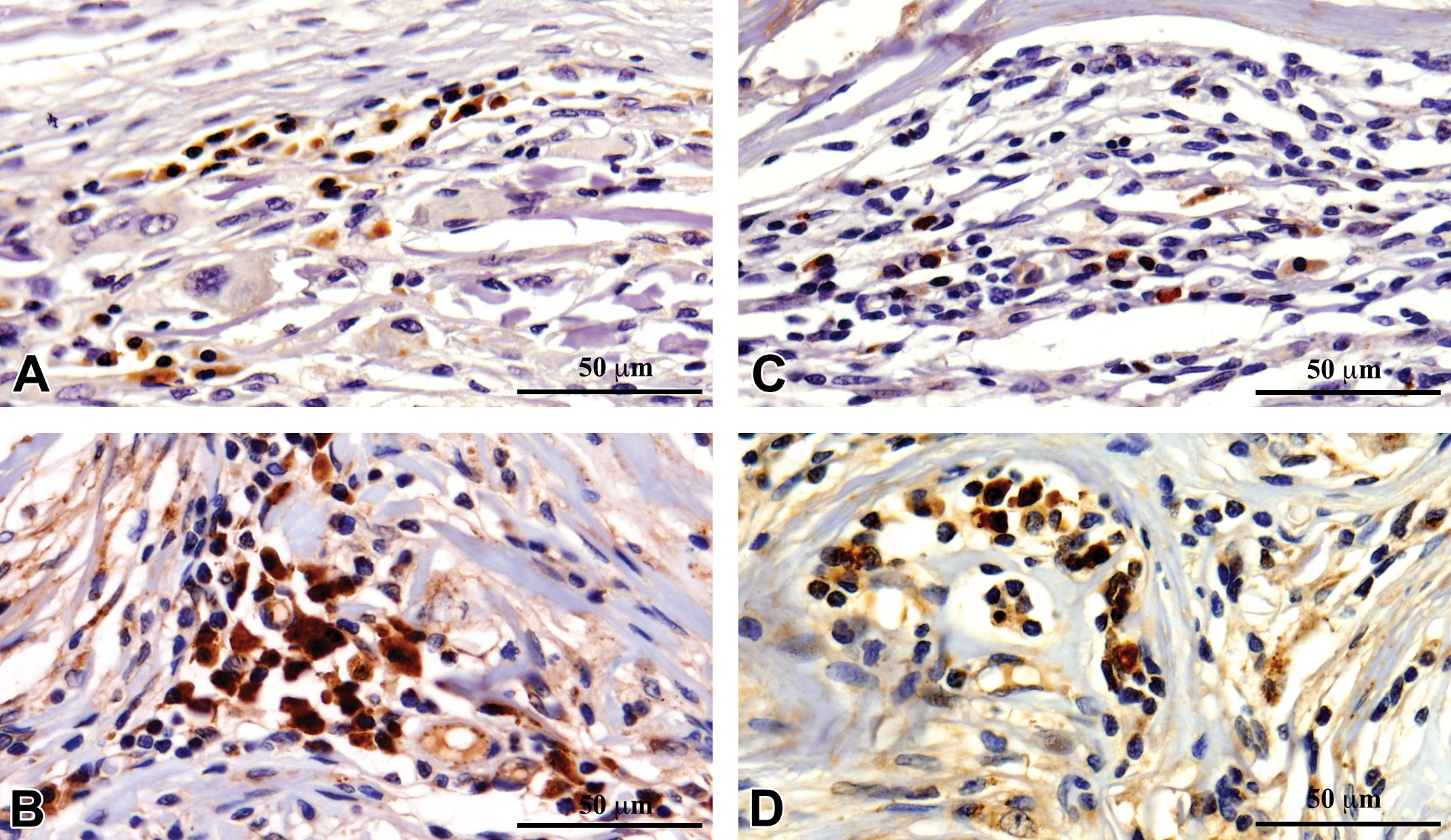
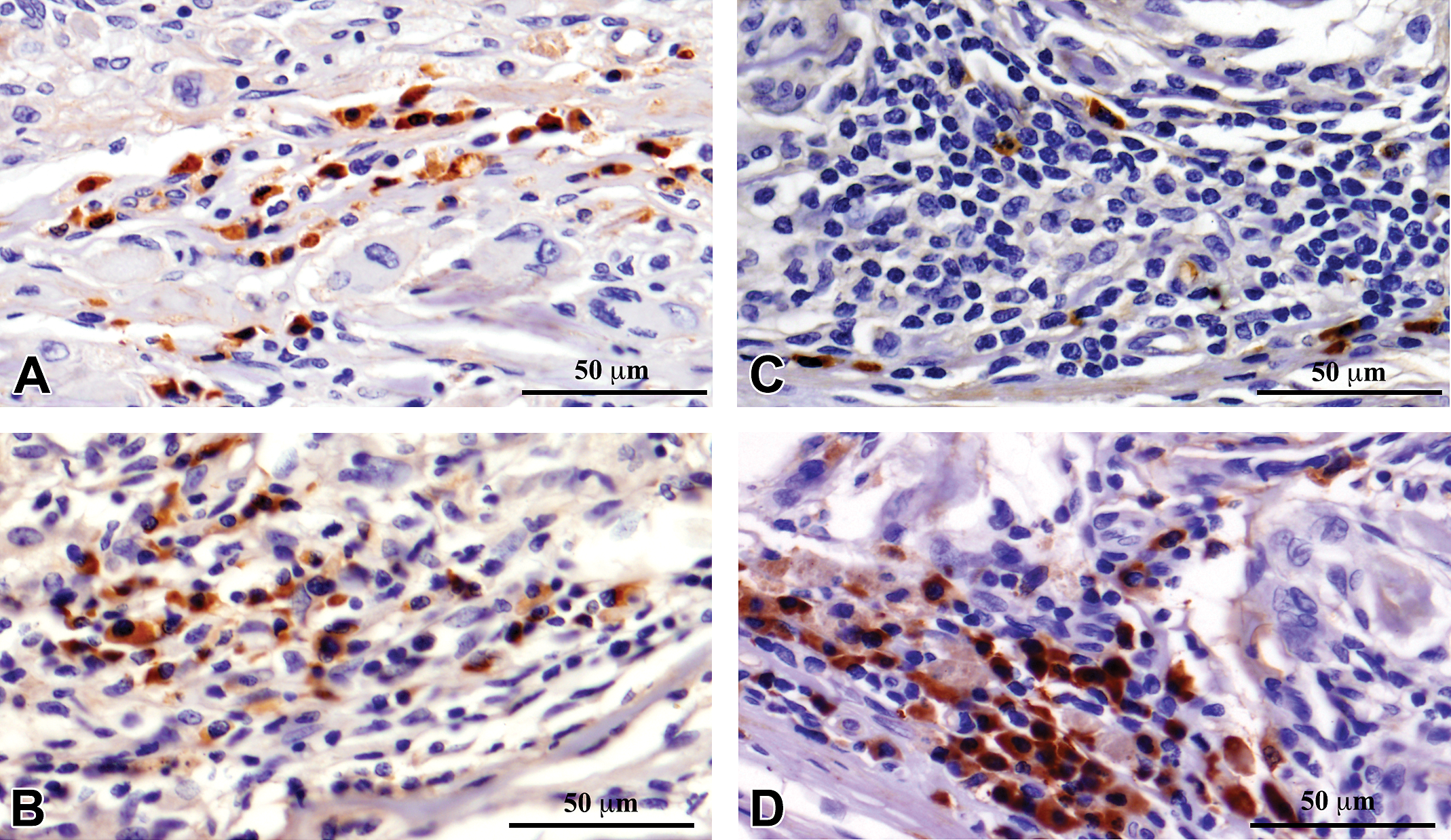
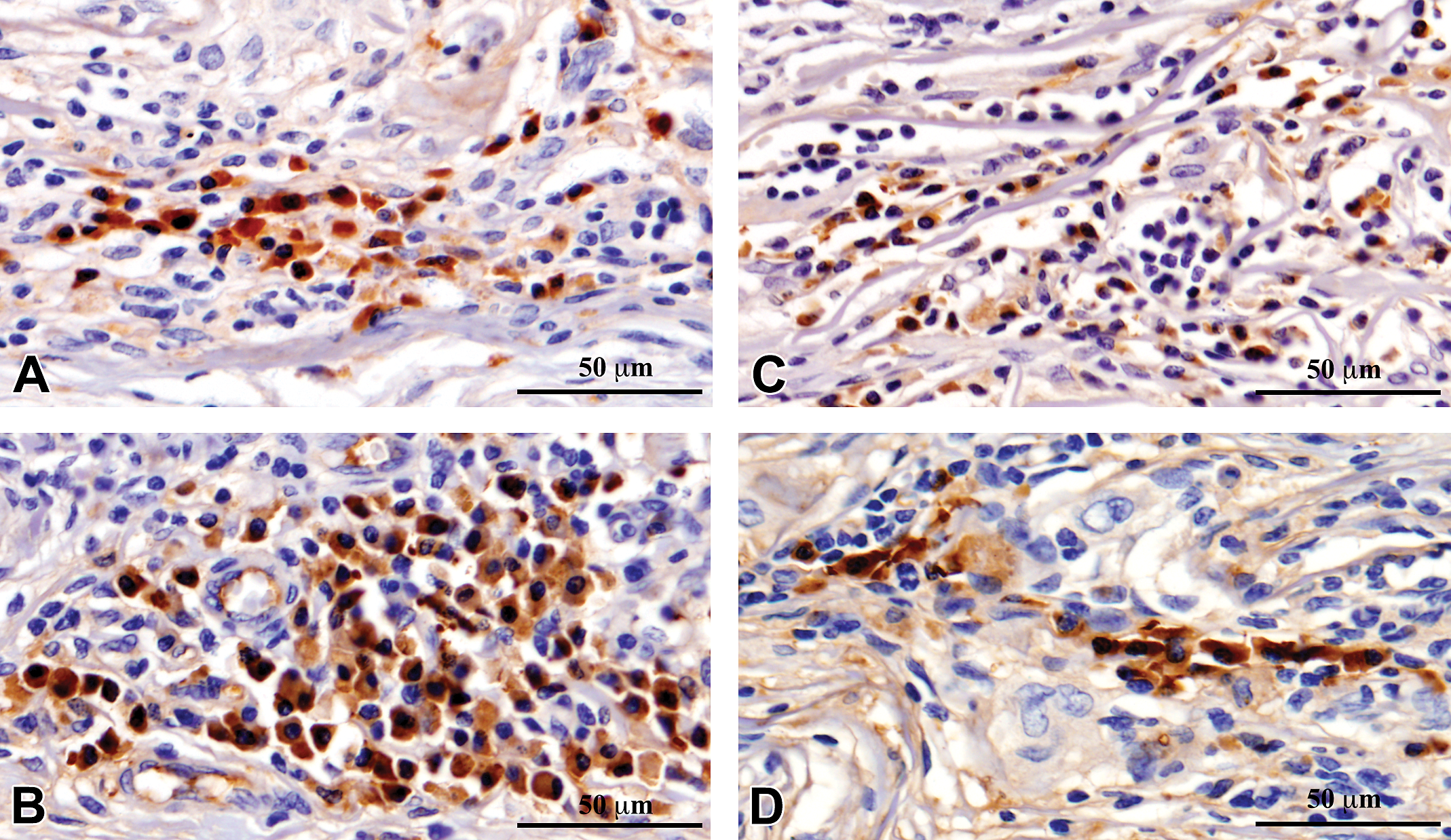
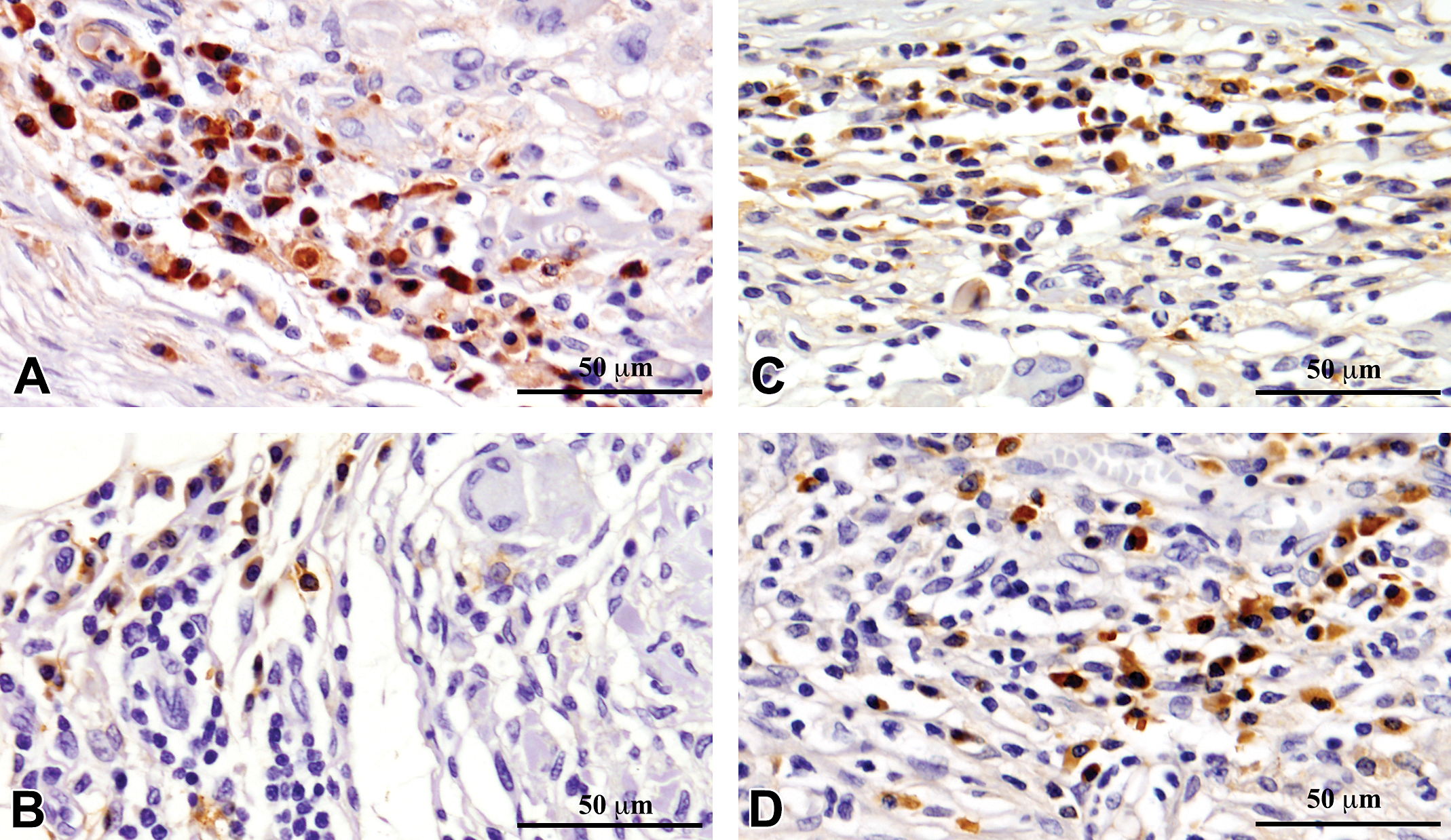
Immunohistochemistry showed significant infiltration of M1 macrophages, CD80 (Figure 2); M2 macrophages, CD163 (Figure 3); Helper T cells, CD4 (Figure 4); and Cytotoxic-T cells, CD8 (Figure 5) into the reaction zone. The ratio of M1 to M2 macrophage in CDS- and CSIS-implanted tissues indicated predominance of M2 macrophages at early time points of 1 week and 4 weeks (ratio < 1), and by 12 weeks there was equal distribution of M1 and M2 cells (Figure 6). The CD4 to CD8 ratio showed predominance of CD8 cells at 1 week and equal distribution by 4 weeks. By 12 weeks, the CD4 cells were predominant with ratio more than 1, but the CSIS had higher CD4 predominance than CDS (Figure 7).
Immunohistochemical detection of CD80-positive M1 macrophages in commercial small intestinal submucosa (CSIS; A and B) and cholecyst-derived scaffold (CDS; C and D) in the tissue reaction induced by subcutaneous implantation in rat at 4 weeks (A and C) and 12 weeks (B and D).
Immunohistochemical detection of CD163-positive M2 macrophages in commercial small intestinal submucosa (CSIS; A and B) and cholecyst-derived scaffold (CDS; C and D) in the tissue reaction induced by subcutaneous implantation in rat at 4 weeks (A and C) and 12 weeks (B and D).
Immunohistochemical detection of helper T cells using antibody against CD4 in the tissue reaction caused by commercial small intestinal submucosa (CSIS; A and B) and cholecyst-derived scaffold (CDS; C and D) subcutaneous implantation in rat at 4 weeks (A and C) and 12 weeks (B and D).
Immunohistochemical detection of cytotoxic-T cells using antibody against CD8 in the tissue reaction caused by commercial small intestinal submucosa (CSIS; A and B) and cholecyst-derived scaffold (CDS; C and D) subcutaneous implantation in rat at 4 weeks (A and C) and 12 weeks (B and D).
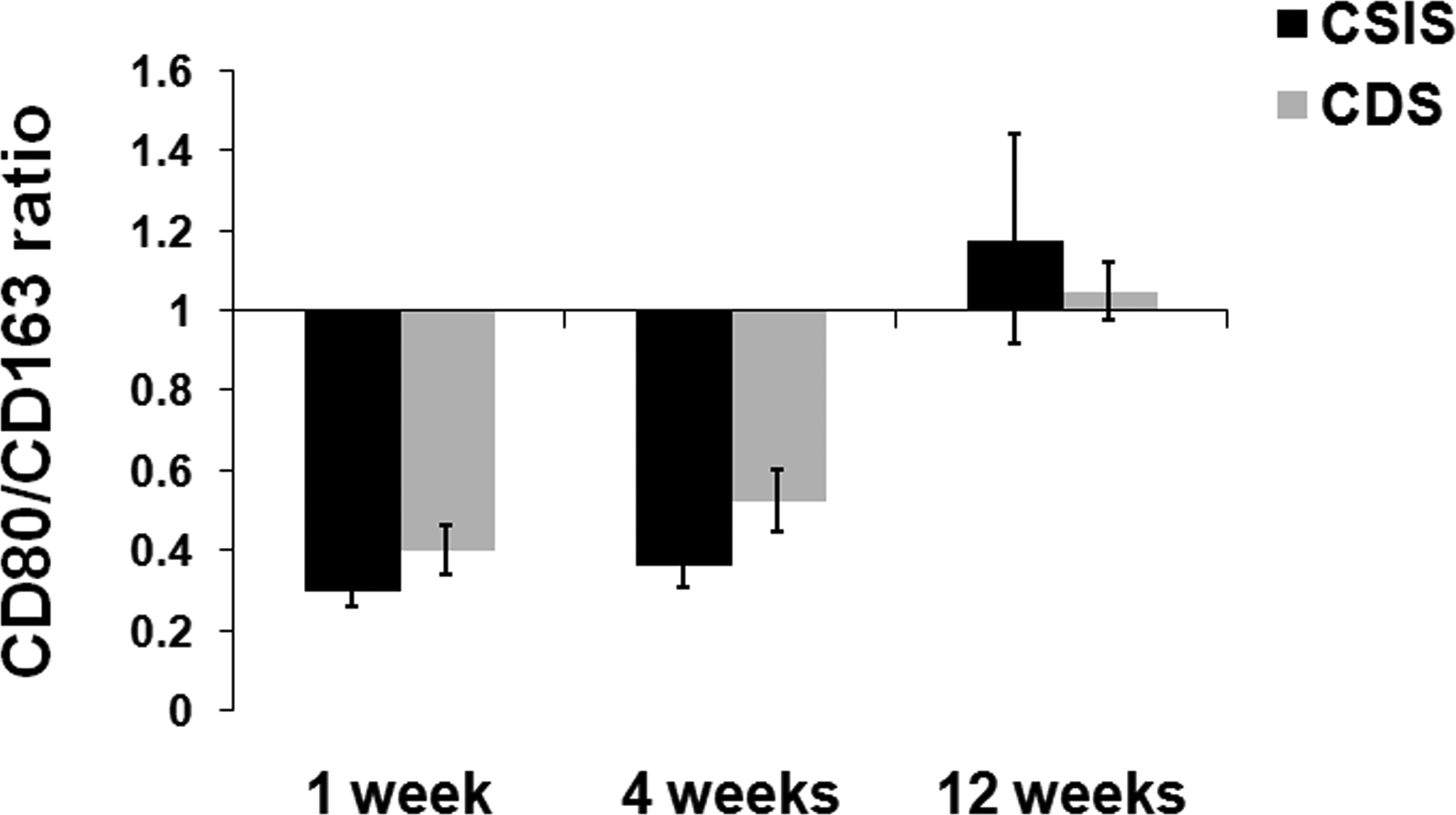
The ratio of number of CD80 M1-positive macrophages to the number of CD163-positive M2 macrophages (mean ± SD, n = 4).
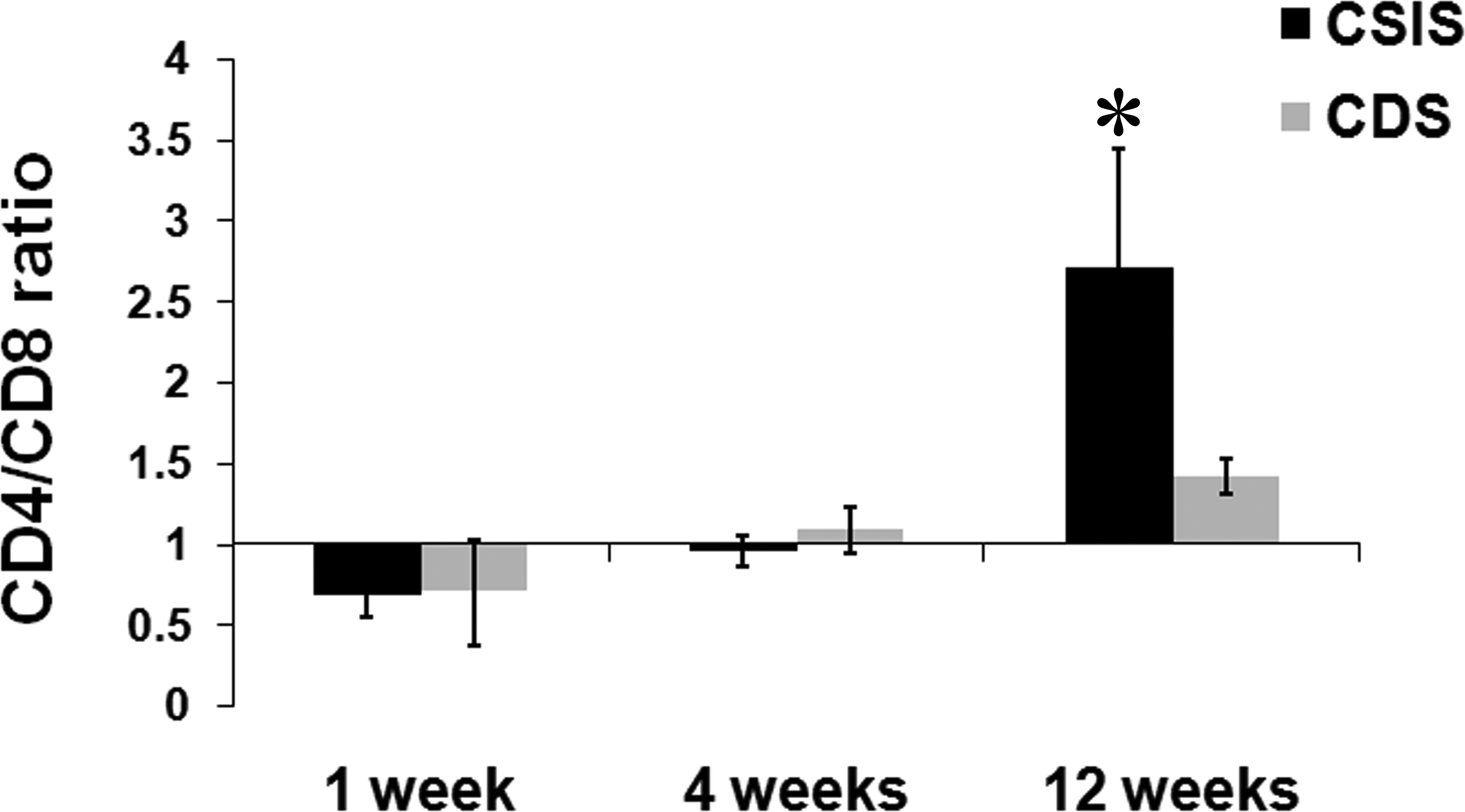
The ratio of number of CD4-positive helper T cells to the number of CD8-positive cytotoxic-T cells (mean ± SD, n = 4). * represents significant difference between the groups, p value < .05.
Gene Expression Analysis
M1/M2 macrophage polarization
Macrophage functional polarization was determined by calculating the ratio of the extent of gene expression of M1 macrophage marker iNOS to the M2 macrophage marker arginase-I. Both the CSIS and the CDS scaffolds induced M2 macrophage polarization at all time points of the study (ratio < 1), with higher M2 polarization for CDS than CSIS at 4 and 12 weeks after implantation. However, the CSIS appeared to have induced more M2 macrophage at the first week of implantation (Figure 8).
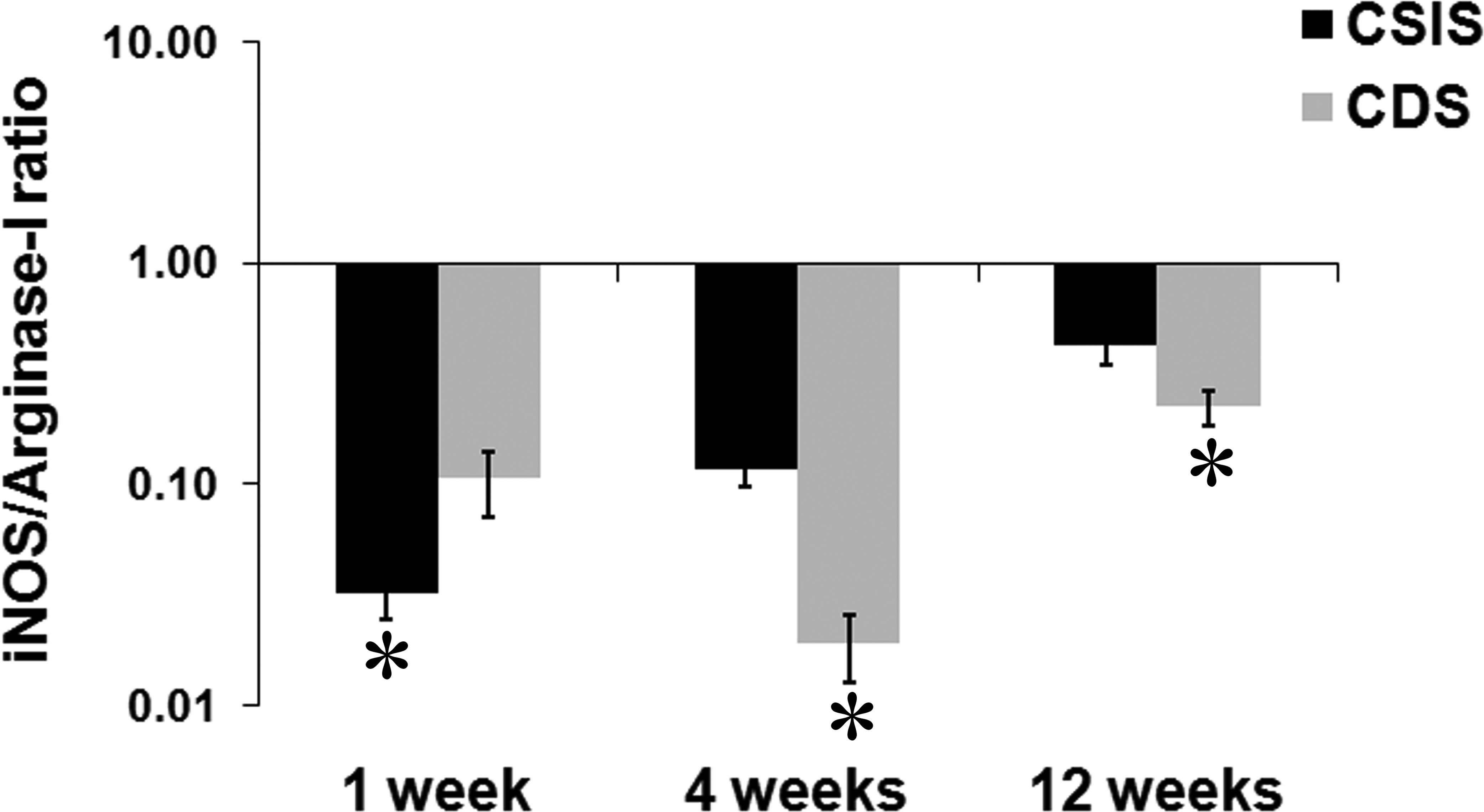
The phenotypic polarization of macrophages in the tissue reaction demonstrated by the ratio of fold change in mRNA expression of inducible nitric oxide synthase (iNOS) to that of arginase-I (mean ± SD, n = 4) which are functional markers for M1 and M2 macrophages, respectively. * represents significant difference between the groups, p value < .05.
TH1/TH2 lymphocyte polarization
Helper T cell polarization was also determined by calculating the ratio of the extent of gene expression of TH1 marker INF-γ to TH2 marker IL-4. The CSIS induced TH1 polarization (ratio > 1) at 1 week and 4 weeks. By 12 weeks, there was a switch to TH2 polarization (Figure 9). However, the CDS scaffold induced TH2 polarization (ratio < 1) at all time points of the study.
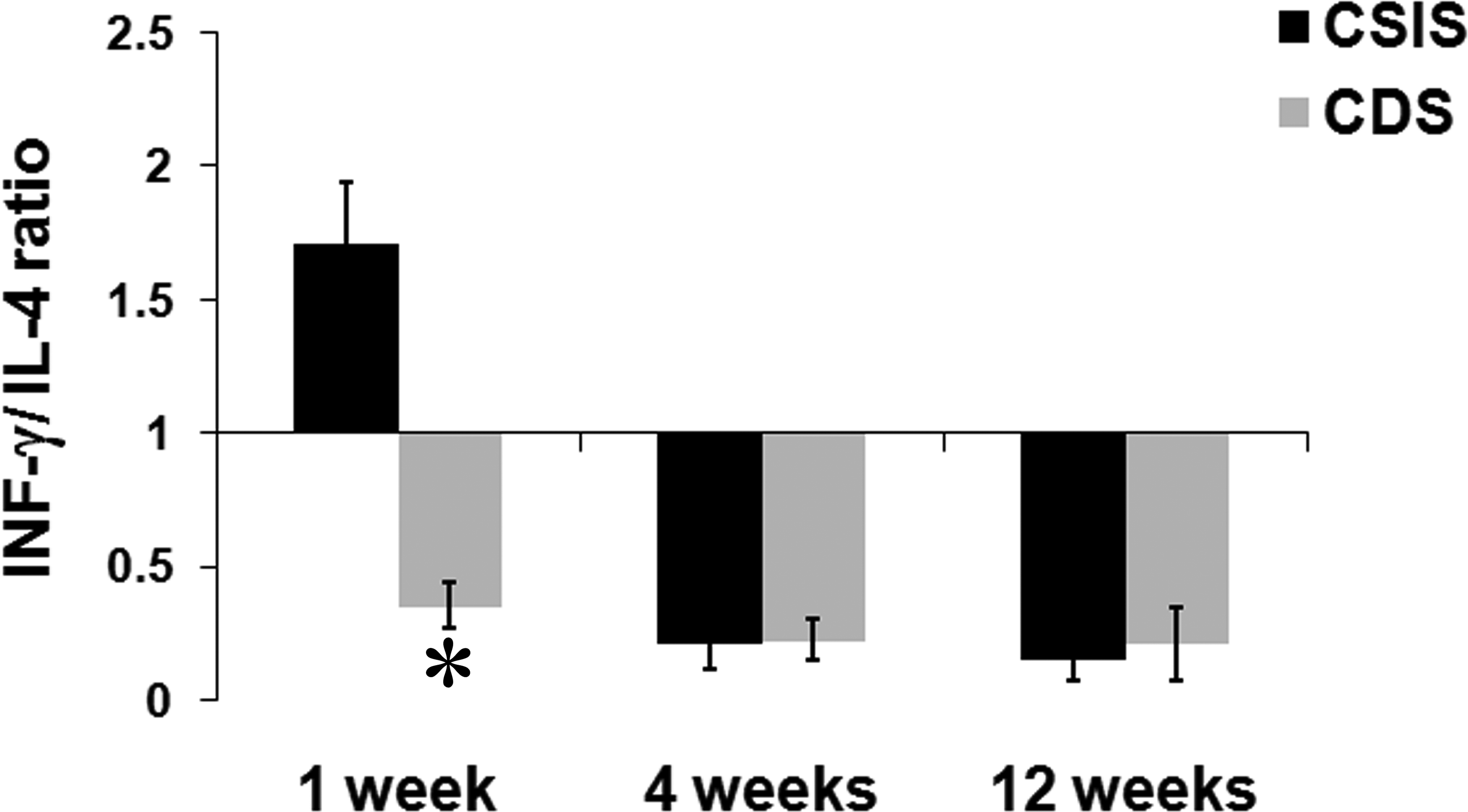
The phenotypic polarization of T-lymphocytes in the tissue reaction demonstrated by the ratio of fold change in mRNA expression of interferon gamma (INF-γ) to that of interleukin-4 (IL-4), which are functional markers for TH1 and TH2 cells, respectively (mean ± SD, n = 4). * represents significant difference between the groups, p value < .05.
Discussion
The safety evaluation of the local tissue response to CDS has been expanded to include local immunopathologic response. The biocompatibility results as per ISO10993, Part-6 indicated that CDS was similar to the reference material CSIS, as indicated by the calculated irritancy score at each time point. But this and similar protocols are designed for materials of nonbiological origin, such as polymers that are not necessarily immunogenic. Xenogeneic grafts can induce inadvertent immunogenic reaction in man (Badylak and Gilbert 2008). Clinical complications of severe pain, inflammation, and graft-versus-host disease associated with the use of intestine-derived scaffolds have been attributed to the immunogenicity of the graft material (Kalota 2004; Ho, Witte, and Bird 2004; Petter-Puchner 2007; John et al. 2008; Wang, Hsu, and Long 2009).
Advances in molecular biology techniques are beginning to be used as standard procedure (Maronpot 2012; Ettlin 2013) for supplementing safety evaluation data collected from animal experiments. The use of immunohistochemistry as an adjunct tool for histomorphological safety assessment is being contemplated widely (Dahe et al. 2011; Muhamed et al. 2013). These procedures largely elucidate the nature of cellular and molecular mechanisms responsible for modulating biological responses to foreign materials. In this article, adjunct tools were used to elucidate the nature of local immunopathology. Biologic scaffold materials induce constructive tissue remodeling by inducing M2 macrophage response (Brown et al. 2009). Similarly, a preferred TH2 lymphocyte polarization has been observed in association with graft acceptance reaction (Allman et al. 2001). It is also pertinent to note that the relative proportion of cell-types was relevant, assuming that there was optimal function of these cells in the niche, rather than their actual numbers in determining the outcome. Therefore, in this study, the relative abundance/expression of M1 to M2 macrophages, helper to cytotoxic T-lymphocytes, and TH1 to TH2 lymphocytes was studied.
M1 phenotype macrophages are proinflammatory and promote aggressive chronic inflammation while M2 phenotype macrophages are anti-inflammatory and promote a constructive remodeling process (Mills et al. 2000). In any tissue reaction, both these phenotypes can be expected, but the predominance of either one of these macrophage phenotypes determines the outcome of the tissue reaction, largely by regulating the cytokine milieu of the microenvironment (Stout et al. 2005). Although CD80 immunopositivity is not restricted to M1 macrophages, it is frequently used for identifying these cells in histology sections while studying tissue response to biomaterials (Badylak et al. 2008). Therefore, in this study, macrophage phenotypes were detected by immunohistochemistry and in each case the number was quantified (Figures 2, 3, and 6). At the end of the 1st and 4th week, M2 macrophage reaction appeared to dominate in the tissue section but switched to M1 dominance by the 12th week for both CSIS and CDS. There was no significant difference in the relative proportion of these cells at the reaction site. However, significant difference was observed in the expression of iNOS and arginase-I genes for M1 and M2 macrophages, respectively (Figure 8). Results of the gene expression studies indicated that both the CSIS and the CDS induced a desirable M2 macrophage polarization at all stages of the evaluation. However, the M2 reaction was relatively less at the end of the 1st week in CDS-implanted tissue. A reversal was seen later at 4th week and 12th week. Therefore, the CDS was deemed to have induced a macrophage reaction favoring graft acceptance, at least after the 1st week.
In this study, the numbers of TH1 and TH2 cells were not enumerated due to lack of adequately validated immunohistochemisty markers. However, gene expression analysis was performed for 2 candidate genes, namely INF-γ and IL-4, markers for studying the extent of TH1 and TH2 polarization. The CSIS caused a TH1-polarized reaction at 1 week but subsequently harmonized to the desirable TH2-polarized reaction. On the other hand, the CDS-implanted tissue consistently had TH2 polarization at all time points indicating its capability to promote graft acceptance rather than rejection (Figure 9). Hence, the results suggested that CDS and CSIS have different immunologic potential in the rat model.
Assessment of relative proportion of CD4 and CD8 cells is an important determinant of T-cell function during transplant acceptance/rejection reaction (Amadori et al. 1995; Hautz et al. 2012; Li et al. 2013). So, in this study, T-cell subtypes were stained immunohistochemically and the ratio was calculated. Considering that a few nonhelper T cells (e.g., monocytes and dendritic cells) can be CD4-immunoreactive, manual counting ensured identification of immunopositive lymphocytes (Figures 4, 5, and 7). Both CDS and CSIS induced CD4/CD8 ratio less than 1 showing the cytotoxic T-cell predominance at 1 week. By 12 weeks, the ratio reached more than 1, indicating CD4 predominance and this was significantly high for CSIS compared to CDS (Figure 7). This observation cannot be considered a desirable reaction because higher CD4 predominance is also sometimes observed with graft rejection (Hautz et al. 2010). However, it may be inferred that the CDS is not likely to induce an undesirable cytotoxic reaction.
It was not the primary objective of this article to demonstrate that CDS, in comparison with CSIS, is the superior scaffold for regenerative medical application. However, the supplementary data on local immunopathological reaction presented here indicates CDS and CSIS have different immunologic potentials. The CDS is not a market product, and the significance of these complementary data may not become evident until vigorous clinical use of CDS fabricates. Nevertheless, the article highlights the differential ability of xenogeneic grafts to induce local immunopathologic reaction, despite similarities in the nature of histomorphological reaction recorded at safety evaluation. Certainly, the adjunct procedures similar to those used here provide wider dimensions to the safety evaluation data on animal-derived scaffolds/biomaterials. It is important to note that no additional animal experiment was needed to collect these extra data in support of the safety of CDS. However, extensive standardization may be needed to avoid inherent deficiencies while using immunohistotechnology as a test procedure. Further, a comparative study of the local immunopathological reaction induced by other scaffolds of mammalian origin may also be useful in judging the scope of using these markers for routine use.
Conclusion
This article presents data on the nature of local immunopathologic tissue reaction, in a rat subcutaneous model, for porcine CDS in comparison with a medical grade scaffold. Despite the similarity in biocompatibility, as per standard ISO-safety testing, the CDS induces differential immunopathologic responsiveness that needs further characterization.
Footnotes
Acknowledgment
The authors thank the Department of Biotechnology, Government of India for financial support (BT/PR15461/MED/32/167/2011).
Authors’ Note
Mr. Jaseer is a senior research fellow of the Indian Council of Medical Research and Mrs. Deepa is a senior research fellow of the Council of Scientific and Industrial Research.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Department of Biotechnology, Government of India (BT/PR15461/MED/32/167/2011).