
Abstract
Past research suggests that children from two-parent married families fare better than children from other families on many outcomes. Only fragmented evidence on diverse family trajectories in association with child mental health is available. Using multi-channel sequence analysis and data from the UK Household Longitudinal Study, we jointly capture maternal partnership trajectories and type of father co-residence between birth and age 5. We then assess the association between these family trajectories and child mental health at age 5 and 8 using random effects regression. Children whose trajectories include the entrance of a non-biological father or parental separation have the lowest levels of mental health. However, children of never partnered mothers and those who repartner with the biological father have comparable mental health to children of stably married biological parents. Thus, not all types of family complexity or instability appear to be equally detrimental to children’s mental health.
Introduction
Family forms in high-income countries have become more diverse due to increased rates of separation, cohabitation, non-marital childbearing, repartnering, or multi-partner fertility (Thomson, 2014). In turn, children are now more likely than in the past to experience parental separation, living with a lone parent or the entrance of a new parental figure. Previous research consistently finds that children growing up in less common family forms have worse mental health compared to children from two-biological-parent families (Härkönen et al., 2017). However, more intricate associations are revealed when family trajectories are studied longitudinally, with attention to multiple domains of children’s early family life.
For example, previous studies have found that specific family trajectories, such as those including parental separation, lone-motherhood, or repartnering, are differentially associated with child mental health (Lee & McLanahan, 2015; Mariani et al., 2017). Whereas experiencing parental separation is often negatively associated with child mental health, the entrance of a new parental figure or living with a single parent shows weaker or mixed associations. We aim to build on this foundational work; emphasising the need to precisely capture the development of childhood family context over time.
We advance the literature by using a novel child-centred approach that captures children’s maternal partnership trajectories and type of father co-residence as two separate domains in multi-channel sequence analysis. This child-centred approach allows us to achieve a nuanced understanding of children’s early family context and how it relates to their mental health. We emphasise the parallel roles of mothers’ partnership status and co-residence with a biological or non-biological father, which heavily influence children’s experiences and outcomes (Jensen et al., 2017). Taking a child-centred perspective is important as past research yields different results when focussing on children as opposed to adults, for example, in the propensity of experiencing separation (Kalmijn & Leopold, 2021) or socioeconomic disadvantage (McLanahan, 2004). Moreover, taking a child-centred perspective instead of a parent-centred one reveals relational ties that are specific for individual children that might otherwise be overlooked, especially for children within families characterised by parental repartnering or multi-partner fertility (Cancian et al., 2011).
We focus on the key developmental period of early childhood; with pre-adolescent child mental health thought to be largely predictive of future mental health (Bakker et al., 2012). Early childhood is characterised by a shifting focus from the self to the wider social world, attaining friendships, and growing capacity for empathy and understanding of individual differences paired with the event of school entrance (Vygotsky & Cole, 1978). This stage also brings about potential difficulties, both in learning and emotional regulation.
First, we apply multi-channel sequence analysis to data from the UK Household Longitudinal Study to establish children’s family trajectories between birth and age 5. Then, we explore the association between early-life family trajectories and child mental health using random-effects regression. We approach our analysis through the family instability lens, which encompasses not only family change but also relates to further disruption and precarity in broader family circumstances, such as resources, whether material, emotional, or social (Cavanagh & Huston, 2006). We ask two questions: First, how do different early-life family trajectories relate to child mental health? And second, to what extent can the association between these family trajectories and child mental health be accounted for by other factors, such as material or non-material resources or further family transitions?
Further, we aim to explore whether insights on family complexity, instability, and its consequences, largely explored in the US context, apply to children in the UK. The US and UK are similar regarding high divorce, cohabitation, and non-marital childbearing rates. However, in the US, cohabiting mothers’ socioeconomic background and partnership patterns more closely resemble those of lone mothers, whereas in the UK, cohabiting mothers are more similar to married mothers (Kiernan et al., 2011). British mothers also stand out in their relatively higher likelihood of (re)partnering with the child’s biological father rather than with a non-biological or social father (Mariani et al., 2017). Thus, family patterns in the UK sit astride the US and the rest of Europe making it a prime case for analysis and theoretical development on the patterns and implications of diverse family pathways for children.
Background
In the past ten years, family complexity has become a central theme in demography due to increased diversification of the family and the recognition of the need to study less common, marginalised family forms. This line of research engages ideas of the second demographic transition and the de-standardisation of life courses in the context of increased availability of high-quality longitudinal data that has enabled innovative approaches. Nonetheless, ‘complexity’ remains a fuzzy concept without a consensus definition. Whilst some scholars see family complexity as an indicator of non-standard sibling composition (i.e. children residing with other than full biological siblings; Brown et al., 2015), others define complexity as a context different to the ‘non-complex’ two-married-biological-parent family setting (Carlson & Meyer, 2014), or assert that complexity relates to complicated family relationships following separation (i.e. co-parenting and joint custody patterns) or repartnering (i.e. forming new nuclear families, or acquiring new parental figures/siblings) (Thomson, 2014).
Thus, the concept of complexity has been critiqued. For example, a common area of contention is whether living with biological cohabiting or single parents (due to separation or lone motherhood) constitutes living in a complex family. Although evidence shows that these family forms are associated with more precariousness and worse child outcomes than married biological-parent families, family sociologists emphasise the need to understand the (in)stability of family life in connection with child outcomes, rather than (complex) family structures per se (Lee & McLanahan, 2015). The family instability hypothesis asserts that rather than growing up in a complex family itself, it might be the instability experienced by children that negatively affects their mental health (Cavanagh & Fomby, 2019).
We aim to provide further evidence on the temporal patterning of family experiences in association with child mental health. We are guided by past research consistently showing that experiencing a complex and/or unstable family environment is linked to worse child mental health (Amato, 2000; Härkönen et al., 2017; Kiernan et al., 2011). We use the instability lens in our theorisation of family complexity as well as to make a connection between children’s family experiences and mental health. Through this lens, any family change is seen as a form of disruption to the established family system, and periods of heightened stress are expected as all family members need to adjust to new routines, household organisation, and environment (Fomby & Cherlin, 2007). The cumulative effect of family change(s) might then become detrimental for children’s wellbeing (Hadfield et al., 2018).
Many studies have supported this perspective. For example, children had worse behavioural outcomes if they had experienced one or more family transitions (Fomby & Cherlin, 2007). However, it is important to consider the nuances of specific family transitions. For example, children of lone mothers who partner with the biological father fare better than children of mothers who remain single or repartner with a non-biological father (Mariani et al., 2017). Similarly, experiencing the entrance of a new parental figure is less detrimental than parental separation for child mental health (Lee & McLanahan, 2015). Moreover, no positive effects of family change were found by any of the studies reviewed, despite a possible decrease in stress for both children and parents after leaving a high-conflict and high-stress relationship or the entrance of a stepparent who is supportive and involved (Hadfield et al., 2018; Hadfield & Nixon, 2018).
Thus, family instability is deemed to be detrimental to child mental health; with the caveat that other interrelated factors may be simultaneously at play. For example, further precarious circumstances, connected to family resources – financial or other – might arise, and constitute the context of instability. Resource theories assert that worse mental health outcomes are partly due to a lack of resources, be it financial resources, time or attention invested by the parents (Thomson et al., 1994). Parental resources are likely to be more constrained in less common family forms due to lower income, heightened labour market demands as well as less available childcare support. This is especially the case for children living with lone or separated mothers (Mikolai & Kulu, 2018); although parental cohabitation is also less beneficial for children’s economic wellbeing than marriage (Manning & Brown, 2006). Especially in the UK context, these patterns also link to high rates of social inequalities with rising housing costs and precarity (Bone & O'Reilly, 2010). Thus, fewer resources might interfere with family routines, parenting styles, time spent on leisure, or parental emotional availability. This, in turn, might influence children’s mental health.
Beyond instability in family structure and material resources, non-material resources may also be important for children’s wellbeing. For example, maternal health could be seen as an emotional and social resource, as mother’s physical and mental health are both crucial predictors of child wellbeing (Cavanagh & Huston, 2006; Hadfield et al., 2018). Children of mothers with poor physical health have worse mental health and levels of social skill than those of mothers with better physical health (Evans et al., 2007). Similarly, children of mothers with lower emotional wellbeing are likely to experience psychological difficulties in childhood and beyond (Goodman & Tully, 2006). In contrast, some maternal characteristics, such as resilience or dispositional optimism, together with social support networks, might help to buffer the detrimental effect of disruptive family circumstances (Taylor et al., 2012).
Bridging insights from demographic and sociological approaches, we argue that considering both the diversity of (potentially complex) family forms as well as their longitudinal (in)stability is needed to get a nuanced understanding of children’s diverse early life family experiences. Thus, we study a variety of early childhood family settings thereby contributing broader insights compared to past studies that focus on specific aspects of family complexity or instability only (e.g. parental separation or lone motherhood; Goisis et al., 2019; Mariani et al., 2017). Furthermore, this study augments the literature by providing a longitudinal, child-centred analysis that considers the intersections of family complexity and stability with attention to both material and non-material resources in the family context, providing a more complete and nuanced articulation of the connections between early-life family trajectories and children’s mental health.
Methods
Data and Sample
We use data from the UK Household Longitudinal Study (UKHLS, also known as Understanding Society) to study the association between family trajectories and child mental health. The UKHLS is a nationally representative household panel survey that provides detailed information on a multitude of individual- and household-level characteristics and collects yearly information on all household members including children. The UKHLS provides a unique opportunity for a detailed investigation of the childhood family context in the UK. It collects data on child development and health, parental physical and mental health, education, financial precarity as well as on households and their composition. Moreover, it collects retrospective information on adult partnership trajectories since age 16.
We use information from Wave 3 to 10 (2011–2020; University of Essex, 2021b) of the main survey and the Marital and Cohabitation Histories dataset containing detailed information on adult partnership histories (University of Essex, 2021a). Specifically, we utilise information about parents, their partnership histories, their children, as well as the household composition. Starting from Wave 3, information on child mental health is reported by the mother at any wave when the child is aged 5 or 8. Thus, we focus on children at these two ages. In total, 11,159 children are observed either at age 5, 8, or at both ages. We keep children who have at least one record of their mental health score (n = 7579) and exclude those who have missing information on any of the covariates (n = 273).
We created a dataset where children are the unit of analyses, linking information on children’s experiences of maternal partnership and type of father co-residence each month between birth and age 5. Maternal partnership trajectories are constructed using information on the start and end dates of up to fourteen co-residential partnerships (cohabitation or marriage) the mother has had since age 16. We focus on the partnership trajectories of children’s biological mothers and exclude those who reside with non-biological mothers, whether adoptive, foster or stepmothers (n = 161). We further exclude children with widowed mothers (n = 8) and those with same-sex parents due to small sample size (n = 18 at Wave 1).
Our sample consists of 7298 children (6380 families), whose maternal partnership trajectories (birth to age 5) and mental health information are available alongside all covariates. At first observation, 4662 children are aged 5 and 2636 children are aged 8. Children are observed once (n = 5133) or twice (n = 2165). The small share of children observed twice is a limitation of the data collection design. Nonetheless, similar results emerge when only analysing children observed at both ages (see Supplementary analyses).
Variables
Total Difficulties Score (TDS)
Starting in Wave 3, information on child mental health is collected at any wave when the child is 5 or 8 years old using the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997). The SDQ is a well-known, broadly utilised 25-item tool for screening children’s psychological attributes. The questions are answered by the primary respondent parent, who is almost always the mother in our sample (99.9%). For statements such as ‘Often fights with other children’ or ‘Often seems worried’, mothers respond ‘not true’ (score of 0), ‘somewhat true’ (score of 1), or ‘certainly true’ (score of 2) for their child. The SDQ has five scales: emotional symptoms, peer relationship problems, conduct problems, hyperactivity, and prosocial behaviour. The outcome variable is the Total Difficulties Score (TDS), made up of scores from the first four subscales, ranging between 0 and 40 points with higher scores indicating worse mental health.
Family Trajectories
The main independent variable is children’s family trajectories between birth and age 5 measured using monthly information on mothers’ partnership trajectories and fathers’ co-residence type. We construct two parallel sequences of maternal relationship status (married, cohabiting, separated, never in union) and type of father co-residence (co-resident biological, co-resident non-biological, not co-resident) for each child as a sequence of 60 monthly states. Mothers who had a previous co-residential relationship are coded as separated whereas those who had not are coded as never in union. This allows us to study different pathways into single motherhood, which may be differentially associated with children’s mental health, although we cannot determine whether mothers who are separated at the child’s birth had separated from the child’s biological father. Nonetheless, these mothers might differ in their sociodemographic characteristics (Lorentzen & Syltevik, 2023), for example, in age at birth, as is the case in our sample where never partnered single mothers are much younger than separated single mothers at birth of the focal child (see Table A1). Thus, children’s experiences might vary due to differences in maternal characteristics, which might, for example, influence mothers’ propensity to repartner.
We use multi-channel sequence analysis (MCSA) to capture childhood family trajectories by investigating the two interrelated dimensions of children’s family trajectories. Sequence analysis represents individual life courses as unique sequences of states, in this instance, a sequence of states for each child (Mikolai & Lyons-Amos, 2017). Cluster analysis is used to create groups of individuals such that sequences in one group are most similar to each other whilst most different to the sequences in the other groups. We use Optimal Matching Analysis (OMA) to determine the distances between each two sequences. As we employ multi-channel instead of ‘single-channel’ sequence analysis, OMA is done in a way that accounts for simultaneously occurring states defined as separate channels (Gauthier et al., 2010). Thus, the cluster solution jointly shows distinct but interrelated dimensions of family trajectories in a single cluster. As a result, we define a typology of children’s family trajectories (for more information, see the technical note in Appendix A3).
Based on the results of the MCSA and linked quality indices (Table A2), we choose a seven-cluster solution indicating the types of family trajectories experienced by children from birth to age 5 (Figure 1): (1) married, biological father, (2) cohabiting, biological father, (3) separated, father not co-resident, (4) never in union, father not co-resident, (5) transition to separation, (6) transition to union, biological father
1
, and (7) transition to union, non-biological father. The typology of family trajectories using multi-channel sequence analysis.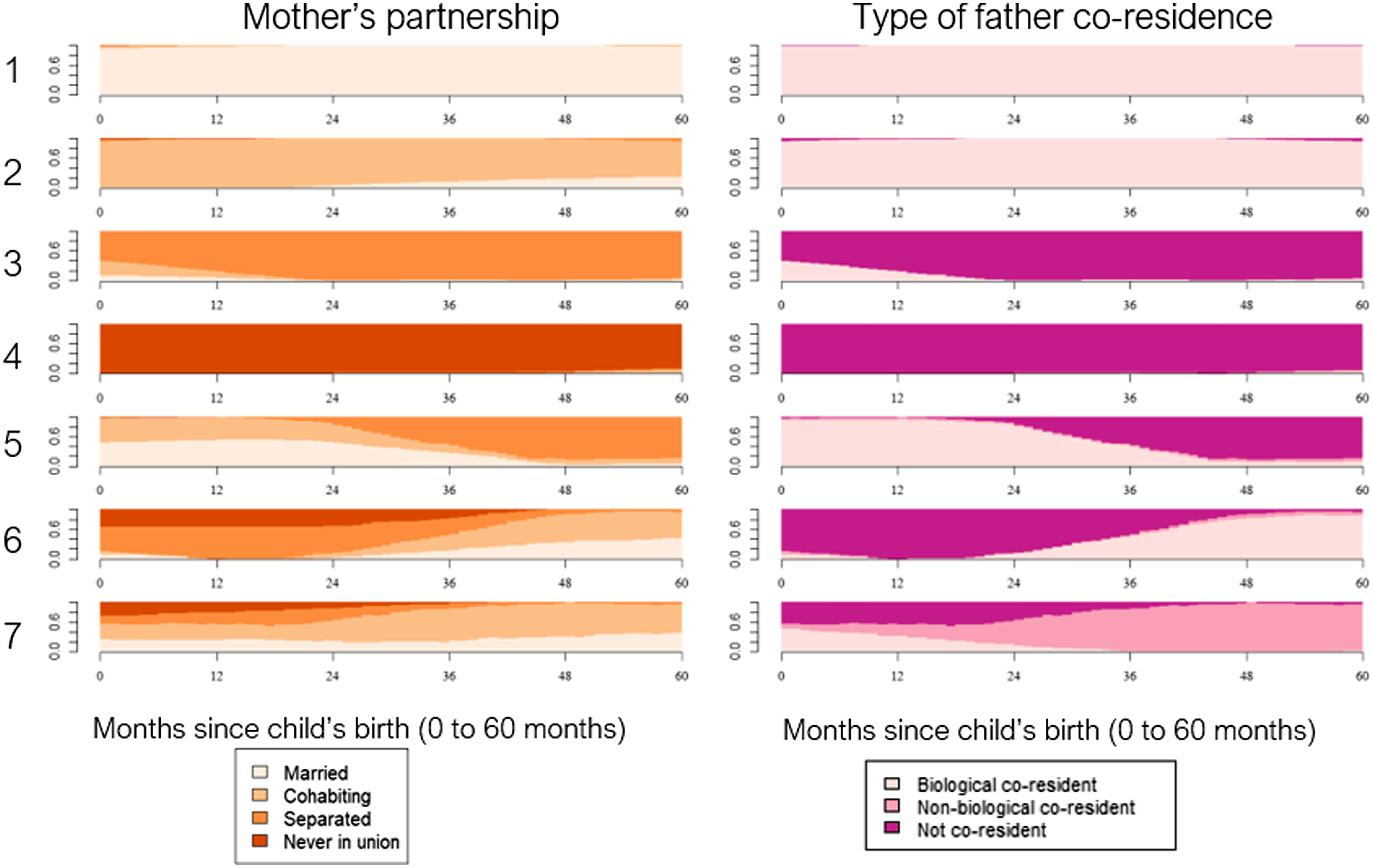
Child Characteristics
Child sex (male/female; time-constant) and age (5 or 8 years; time-varying) are included as categorical covariates. Child ethnicity (time-constant) is mother-reported and measured differentiating between Indian, Pakistani, Bangladeshi, Other Asian, African, Caribbean, White British/White Other, and Mixed/Other ethnic groups. We keep a more fine-grained ethnic categories as previous research shows distinct levels of child mental health for children of different ethnicity in the UK context (Goodman et al., 2008).
Maternal Characteristics
Time-varying maternal education is coded as high (degree-educated or higher), medium (A-levels or equivalent) or low (GCSE or lower). Time-varying maternal employment is categorised as employed (including self-employment), unemployed, or other (e.g. caring responsibilities or in education). Mothers also report their perceived financial situation (time-varying), coded as good (living comfortably and doing alright), getting by, or difficult (finding it quite or very difficult). Time-constant maternal age at birth is coded as below 20, 20–25, 26–30, 31–40, and 41+. Self-reported maternal physical health (time-varying) is grouped as good (excellent, very good, or good) or poor (fair or poor). Self-reported maternal mental health (time-varying) is controlled for, using the SF-12 Mental Component Summary (Ware Jr et al., 1996), a continuous variable, ranging from 0 to 100, with higher scores indicating better mental health. We further include two time-varying variables indicating whether the child has experienced their mother’s transition from a union (both marriage and cohabitation) to separation (n = 150), or from being single (either never partnered or separated) to forming a union (n = 356), inferred from family structure between age 5 and age 8 differing from the family trajectory category. Household characteristics. We distinguish between children residing with natural siblings, other siblings (i.e. at least one half-, step-, adoptive or foster in the household), or no siblings 2 using a time-varying variable.
Analytical Strategy
We use random-effects linear regression (estimated in Stata using the xtreg command) to investigate the association between children’s family trajectories and mental health. We pool information for all children whose mental health scores are available at either age 5 or age 8. As for some children the scores are available at both ages, they can be repeated within individuals. This data structure implies that the assumption of independence of observations in standard linear regression is violated and would lead to biased estimates and an underestimation of standard errors. Moreover, some children come from the same families implying that their mental health scores are not independent from each other. Their levels of mental health as well as the association between family trajectories and their mental health is likely to be more similar to each other than among children from different families due to unobserved factors. Therefore, the TDS (of at least some children) is likely to be correlated due to factors in parents’ and children’s lives that are not accounted for by the covariates (Rabe-Hesketh & Skrondal, 2008). A random-effects specification allows us to correct for these interdependencies between observations and obtain robust estimates (Clark & Linzer, 2015) as well as to include both time-constant and time-varying variables.
We conduct a stepwise analysis to assess how the association between family trajectories and child mental health changes as we adjust for additional factors related to family instability. In line with our theoretical framing, we estimate four models. The baseline model includes family trajectories and sibling presence capturing children’s family setting, with child sex, age, and ethnicity as control variables. The second model adds characteristics that are closely tied to (in)stability in the family’s socioeconomic circumstances (i.e., maternal education, employment, subjective financial situation, and age at birth) possibly mediating or confounding the relationship between family trajectories and child mental health. The third model additionally includes maternal physical and mental health, as proxy measures of non-material resources in the context of (in)stability, which could also act as mediators or confounders. Lastly, the fourth model further adjusts for maternal relationship change (separation or union formation) between age 5 and 8, controlling for further family instability and change.
Results
Descriptive Results
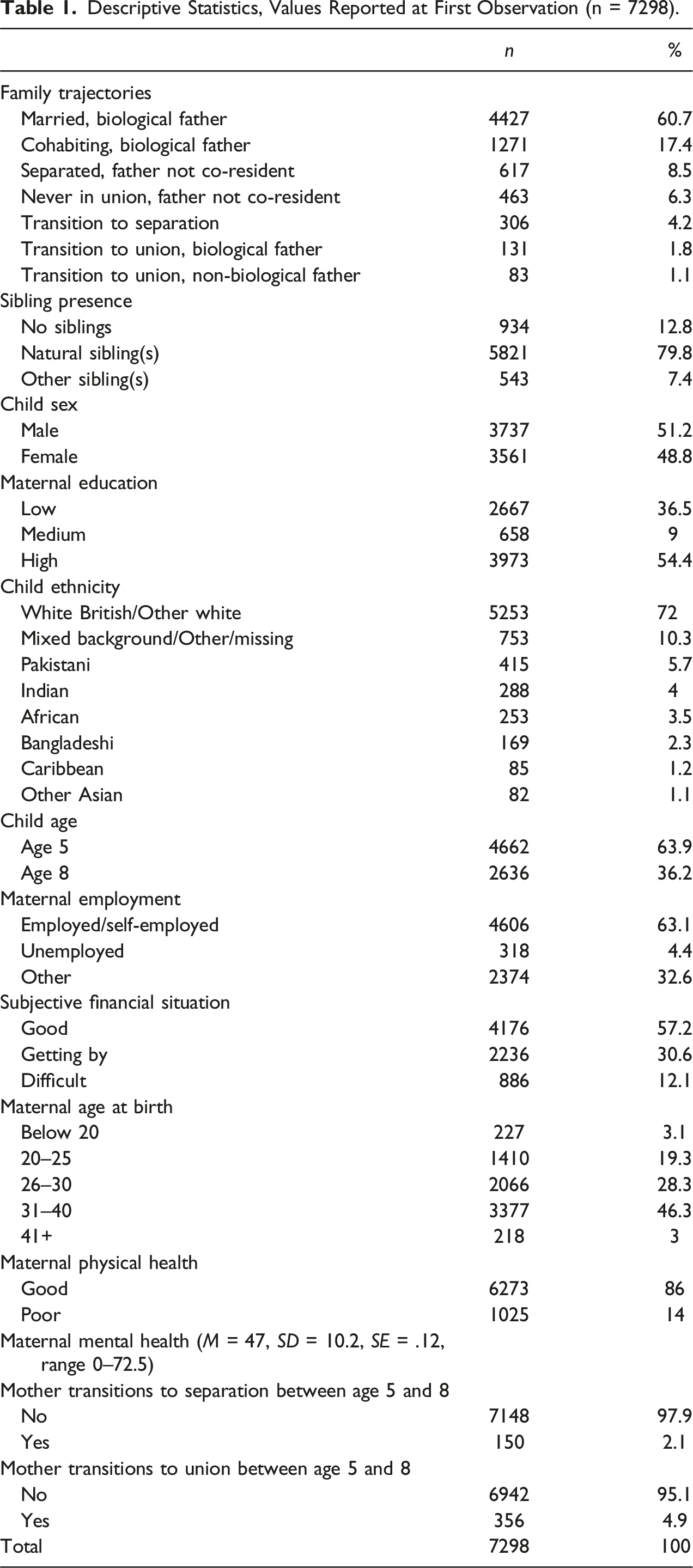
Descriptive Statistics, Values Reported at First Observation (n = 7298).
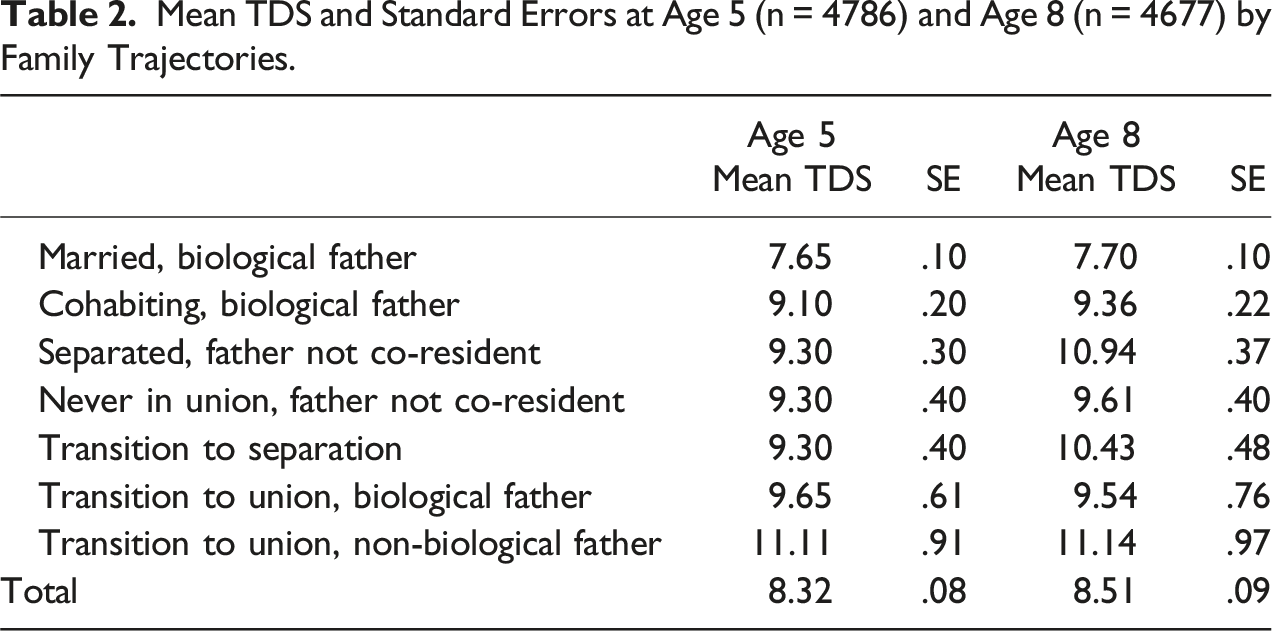
Mean TDS and Standard Errors at Age 5 (n = 4786) and Age 8 (n = 4677) by Family Trajectories.
Regression Models
Random-Effects Linear Regression on Mental Health (TDS) at age 5 and 8.
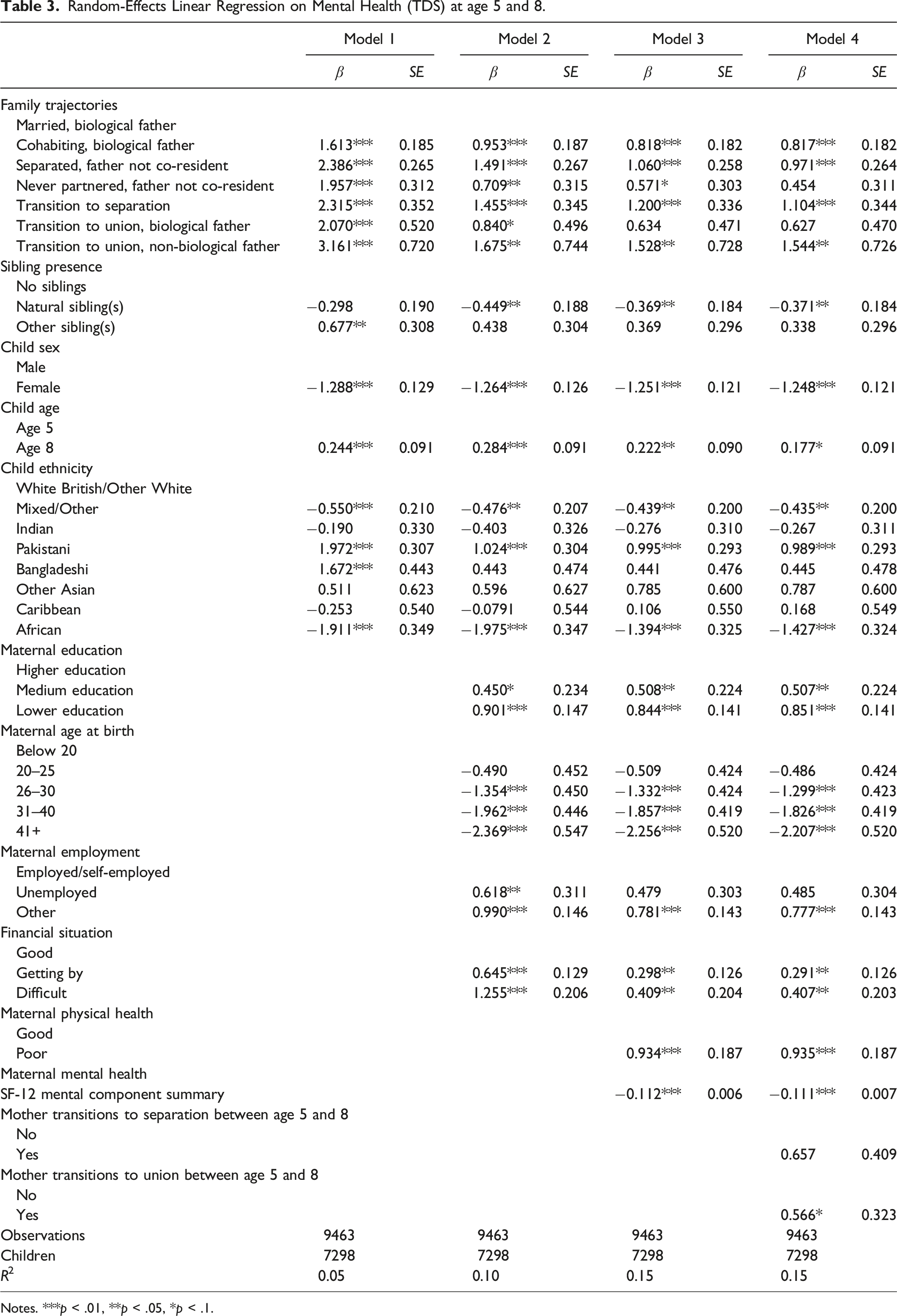
Notes. ***p < .01, **p < .05, *p < .1.
The second model investigates how material resources impact the association between family trajectories and child mental health. Including maternal education, age, employment, and financial situation weakens the association for children across trajectories. Differences in the predicted TDS between children who grow up with two married biological parents and the TDS of children experiencing other family trajectories decline but stay significant. Children whose mothers transition to a union with either a non-biological or biological father, children of never partnered mothers, and both those whose mother is separated or transitions to separation continue to have higher TDS than those growing up with two married biological parents. Predicted TDS also decreases for children of cohabiting parents, although not as dramatically. Children of mothers with lower education, whose employment status is other, and who report financial difficulties have higher TDS than those whose mothers are highly educated, employed, and do not report financial difficulties. Conversely, children of mothers older than 26 have notably lower TDS compared to mothers younger than 20 at birth.
Differences in predicted TDS between children of two married biological parents and children across all other family trajectories decline further when adding maternal physical and mental health (Model 3), although the decrease is much smaller compared to when we adjusted for family resources (Model 2). Notable decrease in predicted TDS is seen mainly for children of separated mothers. Compared to children whose mothers have good health, those with mothers reporting poor health have higher TDS. In terms of mental health, the better the mental health of the mother, the lower children’s TDS.
Finally, controlling for whether the child’s mother has separated or formed a new union (Model 4), we find that although both transitions are linked to higher TDS, only children whose mother transitions to a new union between age 5 and 8 have significantly higher TDS compared to children not experiencing this transition (0.6 points). However, the overall association between family trajectories and child mental health remains the same, except for the TDS of children whose mothers had never been partnered, for whom this association is no longer significant.
Supplementary Analyses
To ensure the robustness of our results, we conducted additional analyses. We estimated identical models with five- and six-cluster solutions. We found similar patterns regardless of the number of clusters; however, the advantage of the seven-cluster solution is that we can distinguish between union formation with the biological or non-biological father. This allows us to highlight that different associations with mental health emerge for these two trajectories characterised by family instability due to maternal repartnering. We replicated the analyses only including children whose TDS is available at both ages 5 and 8. Although this leads to a reduced sample size (n = 2165), the findings are similar to what is shown in the paper. We also explored whether changing the cost specification of insertions, deletions or substitutions would change the obtained family trajectories, but this was not the case. To capture further family complexity and instability, we included covariates on grandparental co-residence and residential mobility. These variables did not make a difference to the results and did not significantly influence child mental health. To check for the robustness of the results related to resources, we estimated models including lagged equivalised household income quintiles (before and after accounting for costs of living; n = 6924). We drew the same conclusions regardless of the variables used.
Many studies have focused on internalising (hyperactivity and conduct problems) and externalising scores (emotional symptoms and peer relationship problems) separately (e.g., Mariani et al., 2017). Whereas we find evidence for higher externalising scores for children whose mothers enter a union with a non-biological father, who separate or transition to separation, or who enter a union with the biological father, we find smaller associations for internalising scores once all covariates are accounted for. Notably, children of mothers who partner with either a non-biological or the biological father, as well as those of never partnered mothers, do not show significant increases in internalising behaviours.
Conclusion and Discussion
We have extended knowledge on the association between early life family trajectories and child mental health using an innovative child-centred approach. In the context of increasing diversity of family forms internationally, we have demonstrated a nuanced way to capture childhood family trajectories from birth to age 5 and their association with child mental health. Studying fathers’ co-residence type and patterns in parallel with mothers’ relationship histories allowed us to highlight a diverse set of family pathways children experience. Using this measure, we then investigated the association between family trajectories and children’s mental health at ages 5 and 8.
Our findings bring further evidence about the diversity of children’s family experiences in the UK. Whilst most children grow up with their biological married or cohabiting parents, over 21% experience a different family trajectory in their first five years. Most of these children live in stable separated- or never-partnered-mother families, with a minority experiencing family instability in the form of maternal repartnering in early childhood. These insights highlight the value of conceptualising childhood family settings through the intersection of family complexity and (in)stability over time to achieve a more nuanced understanding of children’s early life experiences and how these are associated with child outcomes. We proceed to reflect on the insights provided by our paper.
Our findings partially affirm those of previous studies – children experiencing family trajectories that differ from the two-married-biological-parents setting in their first five years generally have worse mental health (Fomby & Cherlin, 2007; Kiernan et al., 2011; Lee & McLanahan, 2015; Mariani et al., 2017). However, using a novel measure of family trajectories, we point out several crucial findings relating to heterogeneity in the interplay of family complexity and instability patterns. Children whose mothers transition into a union with a non-biological father appear to be at the largest mental health disadvantage, followed by those who either experience separation in their first five years, are born to separated mothers, or grow up with cohabiting biological parents. In contrast, compared to children of married biological parents, no difference in mental health scores is observed for either children of never partnered mothers or those whose mothers later form a union with the child’s biological father.
We can interpret these findings through the family instability lens: in their first five years, children of never partnered mothers might experience more family stability than children of separated mothers, those who later separate, or who repartner with a non-biological father and this might be linked to better mental health among these children (Fomby & Cherlin, 2007). Although socioeconomic circumstances seem to be crucial for mental health levels of children living with a never partnered mother, other factors, such as maternal psychological resources, childcare arrangements, and support networks might explain why the mental health of children of never partnered mothers, all things considered, does not dramatically differ from children of stably married biological parents (Taylor et al., 2012).
It is unclear why the mental health advantage for children of mothers who later partner with the biological father is not observed for children of cohabiting biological parents. For children of cohabiting parents, predicted mental health scores fluctuate less as factors are adjusted for compared to children in more complex trajectories but remain comparable to the levels of children whose mothers separated prior to birth. This disadvantage may be due to pre-existing unobserved factors linked to selection into cohabitation as opposed to marriage as well as broader social inequalities experienced by these couples.
Overall, we found that children’s mental health was contingent upon family resources regardless of family type: factors linked to family resources considerably weakened the association between family trajectories and mental health for all children, and especially for children of never partnered mothers and of those who repartner with a non-biological father. Thus, we find some support for the notion that growing up in a non-traditional family, even when there is stability in the early life family trajectory, might negatively influence child mental health in a context of resource deficiency. Furthermore, Bussemakers and colleagues (2022) found that family resources were associated with selection into family complexity/instability more than they were negatively influencing child mental health per se. As our results indicate, maternal physical as well as mental health seem to be important for the mental health of children, particularly those living with separated mothers, or those whose mothers transition to separation in their first five years. Thus, we show that both material and psychological resources underlie the complexity and instability of family contexts in shaping children’s mental health in early life.
Further interrogation of these complex associations is hampered by limitations of this study which largely relate to data constraints. We capture children’s family trajectories in early childhood and cannot draw conclusions about patterns beyond this period. Capturing longer trajectories might reveal more diverse patterns, but at the expense of sample size and representativity. Although our family trajectories show distinct patterns of the timing, duration, and order of states in the context of mostly stable family settings, the timing of specific family transitions is not modelled. We do not investigate a change in mental health following a change in family setting, which should be a priority for future research if repeated information on child mental health is available. The data also did not allow us to follow the family trajectories of children living with non-biological mothers, to capture joint custody arrangements, mothers’ non-resident partnerships, or frequency of contact with non-resident fathers. Moreover, paternal repartnering might bring about further family complexity (Heard, 2007). Children might become a part of more than one family system, or acquire more siblings (Thomson, 2014). Simultaneously tracking both biological parents’ partnership trajectories, non-resident parent–child contact frequency, as well as detailed sibling constellations from either parent’s side is a promising avenue for future research. Finally, as for the majority of studies on young children’s mental health, only a mother-reported measure of child mental health was available, which may be subjective and further influenced by maternal characteristics. To reduce such bias, we have controlled for mothers’ characteristics, including maternal mental health. However, we agree with prior studies calling for data collection on child mental health to include a multi-informant approach (e.g., Ringoot et al., 2015).
We remain cautious in making conclusions regarding the implications of not growing up in a ‘non-complex’, stable family. Most studies report overall effects which might be clouded by large variation for each individual child, of whom most end up being ‘just fine’ regardless of experiencing some form of family complexity/instability; and are rather influenced by the quality of familial relationships (Amato & James, 2010). It must be noted too that not all marriages are equally beneficial for children as some might be affected by high levels of parental conflict, violence or abuse (McNeal & Amato, 1998). Nonetheless, there are many avenues for fruitful investigation for which we have laid a foundation by demonstrating the advantages of a child-centred longitudinal approach to studying family trajectories and thereby showing the need for attentiveness to not all early life family complexity and instability being equally detrimental to children’s mental health.
Footnotes
Acknowledgements
We gratefully acknowledge funding from the Economic and Social Research Council (ESRC); grant number 2460061.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We gratefully acknowledge funding from the Economic and Social Research Council (ESRC); grant number 2460061.
Notes
Appendix
Description of Family Trajectories by Covariates at First Observation (n = 7298).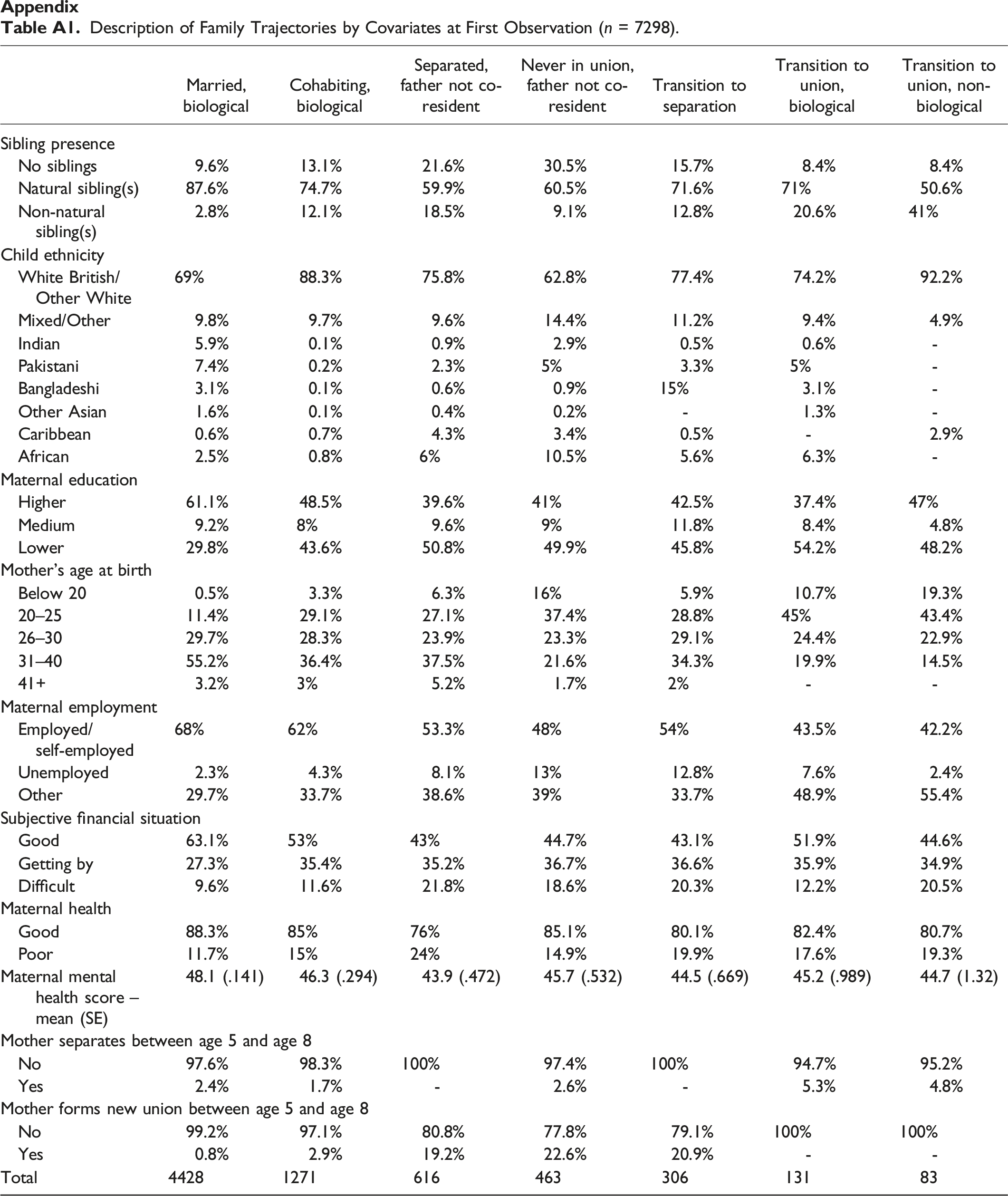
Married, biological
Cohabiting, biological
Separated, father not co-resident
Never in union, father not co-resident
Transition to separation
Transition to union, biological
Transition to union, non-biological
Sibling presence
No siblings
9.6%
13.1%
21.6%
30.5%
15.7%
8.4%
8.4%
Natural sibling(s)
87.6%
74.7%
59.9%
60.5%
71.6%
71%
50.6%
Non-natural sibling(s)
2.8%
12.1%
18.5%
9.1%
12.8%
20.6%
41%
Child ethnicity
White British/Other White
69%
88.3%
75.8%
62.8%
77.4%
74.2%
92.2%
Mixed/Other
9.8%
9.7%
9.6%
14.4%
11.2%
9.4%
4.9%
Indian
5.9%
0.1%
0.9%
2.9%
0.5%
0.6%
-
Pakistani
7.4%
0.2%
2.3%
5%
3.3%
5%
-
Bangladeshi
3.1%
0.1%
0.6%
0.9%
15%
3.1%
-
Other Asian
1.6%
0.1%
0.4%
0.2%
-
1.3%
-
Caribbean
0.6%
0.7%
4.3%
3.4%
0.5%
-
2.9%
African
2.5%
0.8%
6%
10.5%
5.6%
6.3%
-
Maternal education
Higher
61.1%
48.5%
39.6%
41%
42.5%
37.4%
47%
Medium
9.2%
8%
9.6%
9%
11.8%
8.4%
4.8%
Lower
29.8%
43.6%
50.8%
49.9%
45.8%
54.2%
48.2%
Mother’s age at birth
Below 20
0.5%
3.3%
6.3%
16%
5.9%
10.7%
19.3%
20–25
11.4%
29.1%
27.1%
37.4%
28.8%
45%
43.4%
26–30
29.7%
28.3%
23.9%
23.3%
29.1%
24.4%
22.9%
31–40
55.2%
36.4%
37.5%
21.6%
34.3%
19.9%
14.5%
41+
3.2%
3%
5.2%
1.7%
2%
-
-
Maternal employment
Employed/self-employed
68%
62%
53.3%
48%
54%
43.5%
42.2%
Unemployed
2.3%
4.3%
8.1%
13%
12.8%
7.6%
2.4%
Other
29.7%
33.7%
38.6%
39%
33.7%
48.9%
55.4%
Subjective financial situation
Good
63.1%
53%
43%
44.7%
43.1%
51.9%
44.6%
Getting by
27.3%
35.4%
35.2%
36.7%
36.6%
35.9%
34.9%
Difficult
9.6%
11.6%
21.8%
18.6%
20.3%
12.2%
20.5%
Maternal health
Good
88.3%
85%
76%
85.1%
80.1%
82.4%
80.7%
Poor
11.7%
15%
24%
14.9%
19.9%
17.6%
19.3%
Maternal mental health score – mean (SE)
48.1 (.141)
46.3 (.294)
43.9 (.472)
45.7 (.532)
44.5 (.669)
45.2 (.989)
44.7 (1.32)
Mother separates between age 5 and age 8
No
97.6%
98.3%
100%
97.4%
100%
94.7%
95.2%
Yes
2.4%
1.7%
-
2.6%
-
5.3%
4.8%
Mother forms new union between age 5 and age 8
No
99.2%
97.1%
80.8%
77.8%
79.1%
100%
100%
Yes
0.8%
2.9%
19.2%
22.6%
20.9%
-
-
Total
4428
1271
616
463
306
131
83
Cluster Quality Measures for Five-, Six- and Seven-Cluster Solutions.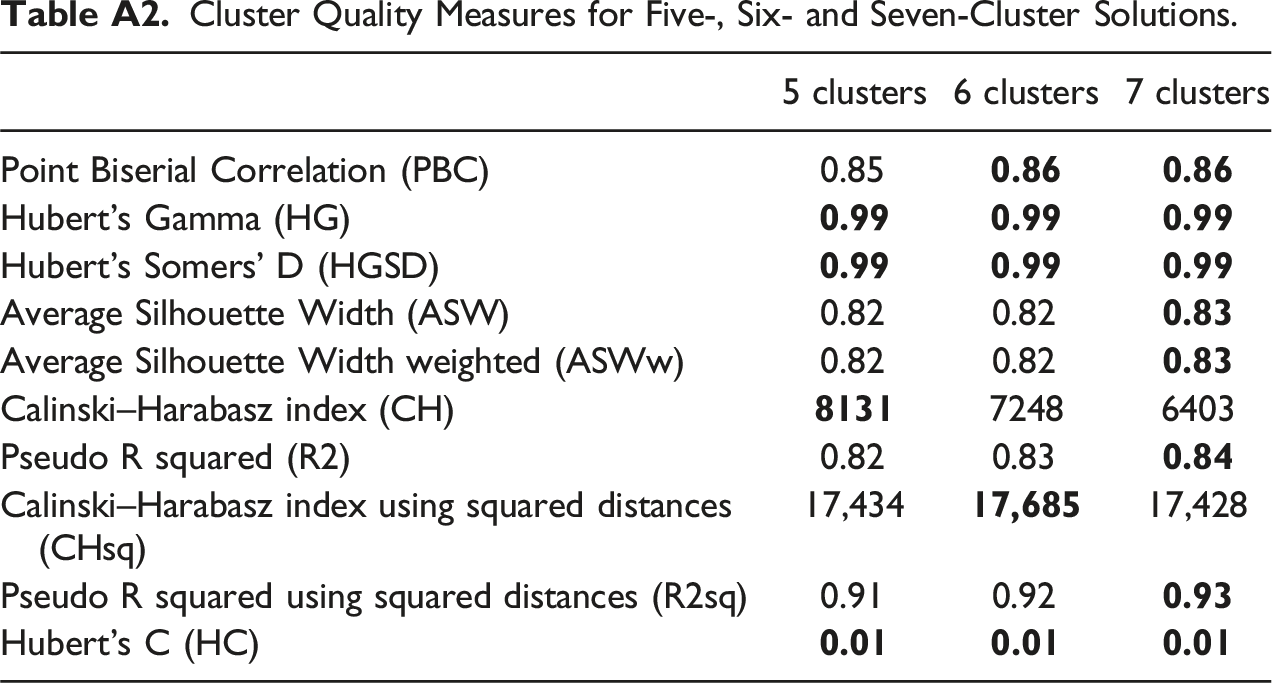
5 clusters
6 clusters
7 clusters
Point Biserial Correlation (PBC)
0.85
Hubert’s Gamma (HG)
Hubert’s Somers’ D (HGSD)
Average Silhouette Width (ASW)
0.82
0.82
Average Silhouette Width weighted (ASWw)
0.82
0.82
Calinski–Harabasz index (CH)
7248
6403
Pseudo R squared (R2)
0.82
0.83
Calinski–Harabasz index using squared distances (CHsq)
17,434
17,428
Pseudo R squared using squared distances (R2sq)
0.91
0.92
Hubert’s C (HC)