
Abstract
Following the accident at Fukushima Daiichi nuclear power plant in 2011, a series of health literacy training workshops for local health workers was developed and implemented. This study aimed to analyse who among the intended audience gained the greatest benefit from the training. Nine health workers attended a workshop consisting of classroom training and a follow-up feedback assessment of materials they created in the workshop. The materials were assessed by a total of 131 intended readers. Using Sakai’s tool, those items asking readers to rate the accessibility of written information were used to compare the materials before and after revision. The total score for Sakai’s measure showed a significant improvement, and the elderly and those without regular doctor visits were more likely to notice improvements after revision. Such health literacy training could serve as a model programme to prevent inequity in access to health information in the face of a regional health crisis.
1. INTRODUCTION
Improving health literacy skills helps people to understand and use health information for health promotion. Raising awareness of health literacy and offering skills training to health professionals helps to improve their communication with their clients (Nutbeam et al., 2018). Scientific evidence linking these two wings of health literacy interventions to improve health literacy within community populations and to offer skills training among health professionals is needed, but this is scarce, and the fundamental question regarding whether health literacy training among health professionals would help to improve access to health information remains unanswered.
Immediately after the accident at Fukushima Daiichi nuclear power plant in 2011, local healthcare professionals faced extreme difficulties with communicating the health risks of the region-wide radiation contamination. As one of the measures to solve this risk communication issue, the lead author worked with colleagues in Japan and the USA to develop, implement, and evaluate a series of health literacy training workshops for public health nurses (Goto et al., 2015). The training was adapted from Rudd’s ‘Eliminating Barriers – Increasing Access Workshop’ (Rudd, 2010), which was designed to help health professionals to understand and fill the gap between professional and public knowledge.
Aiming at wider implementation, the original training (Goto et al., 2015, 2018) was made more concise. Comparison of the original and shorter version revealed that the increase in participants’ knowledge was comparable, although practical application seemed much less in the shorter versions (Machida et al., 2019). Therefore, the authors upgraded the concise version by requiring participants to assess feedback from the intended audience on written materials that they had revised. This study aggregated the data from feedback assessment training of workshop participants, primarily to see if the accessibility of the materials they created improved after revisions made during the workshop, and secondly to explore who among the intended audience gained the most benefit from the improved materials.
2. METHODS
2.1. Workshop content and participants
Content of the health literacy training programme (1-day version) in Fukushima.
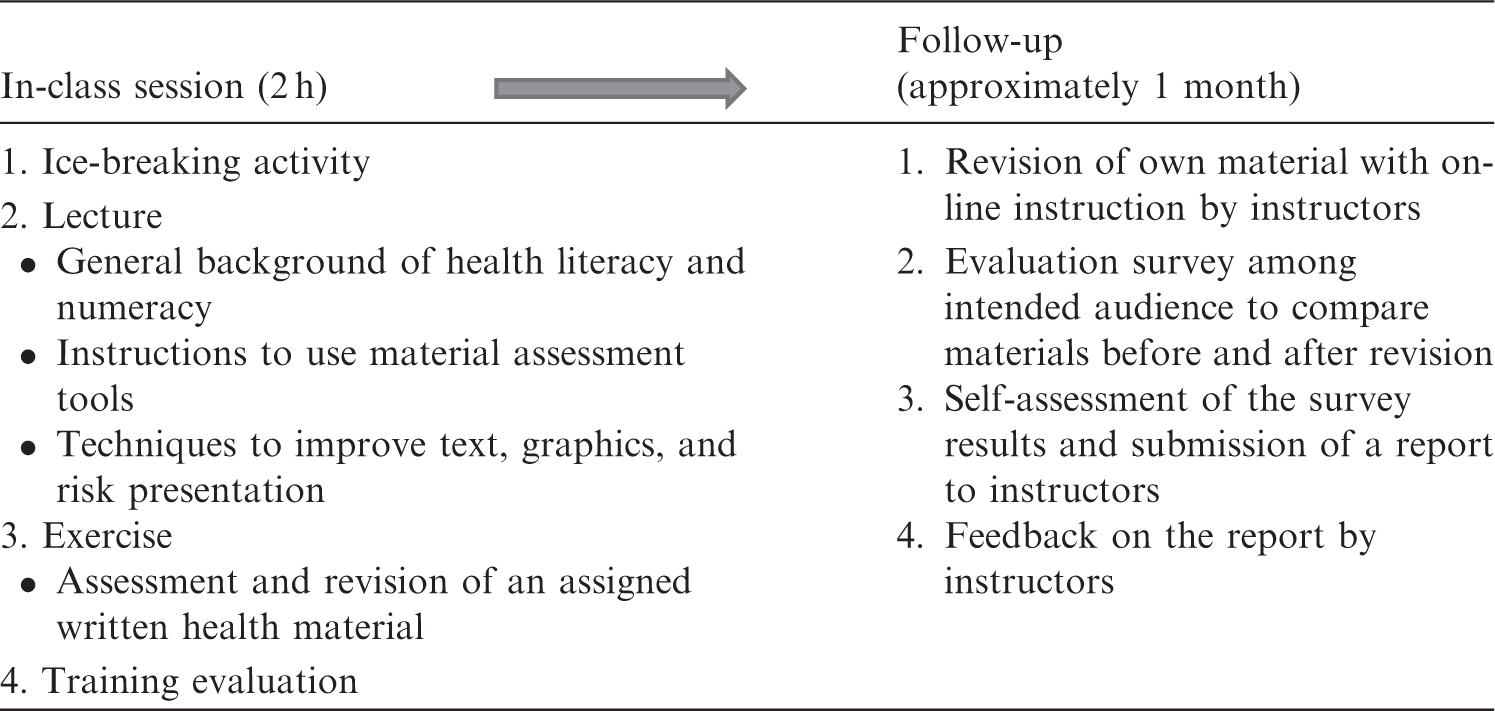

In the present study, three workshops targeting municipality, university, and hospital staff were implemented in 2017 and 2018. These were much smaller in size than previously reported workshops (Goto et al., 2015, 2018) because they were conducted as a pilot study including the feedback assessment component in the training. Five public health nurses attended the municipality workshop; all revised their materials and two succeeded in conducting the feedback assessment. Three participants (two nutritionists and a nurse) attended the university workshop and two feedback assessment reports were returned (the two nutritionists worked as a pair). Individual training was conducted for one doctor, who was from a hospital located outside Fukushima Prefecture but visited Fukushima frequently to implement parenting support activities.
2.2. Feedback assessment items
Basic characteristics of respondents, including sex, age, employment status, whether they attended regular doctor visits, and health literacy level, were collected. Health literacy level was assessed using Tokuda’s one-question instrument (Tokuda et al., 2009). Regarding the main outcome of accessibility of written materials, Sakai’s list of key points to improve Japanese text (Sakai, 2011) was modified and used as a guideline in the training to adapt the original English workshop into Japanese. There were 13 assessment items: Chinese characters (two items); length of sentences and paragraphs (two items); supplementary explanation of terms in parentheses (two items); professional terms (four items); writing style; content; and reading time. Of note, a lower score indicates better accessibility.
2.3. Statistical analysis
Change in the total score for Sakai’s measure before and after revision was examined using Wilcoxon matched-pairs signed-rank test. Regarding analysis of factors associated with improvement of the total score for Sakai’s measure, Chi-squared test was used for univariate analysis and a binominal logistic regression model was used for multi-variate analysis by entering factors that were significant in the univariate analyses. All statistical analyses were conducted using STATA Version 14.0 (Stata Corp, College Station, TX, USA).
2.4. Ethical consideration
The protocol of this study was reviewed and approved by the Ethics Committee of Fukushima Medical University (No. 29116).
3. RESULTS
Five reports with data from feedback assessment surveys were collected from three nurses, one pair of nutritionists, and one doctor. They developed leaflets on health check-ups, cancer screening, prevention of osteoporosis, healthy life expectancy, and support for children with disabilities. The total number of survey respondents, who were the intended audience of the participants’ written materials, was 131.
The total score for Sakai’s measure decreased significantly from 6 (range 0–13) to 0 (range 0–13) (P < 0.001), indicating better accessibility. When examining at subscale level, the proportion of those who reported improvement was lower for ‘supplementary explanation of terms’ and ‘content’.
Feedback assessment results and respondents’ characteristics.
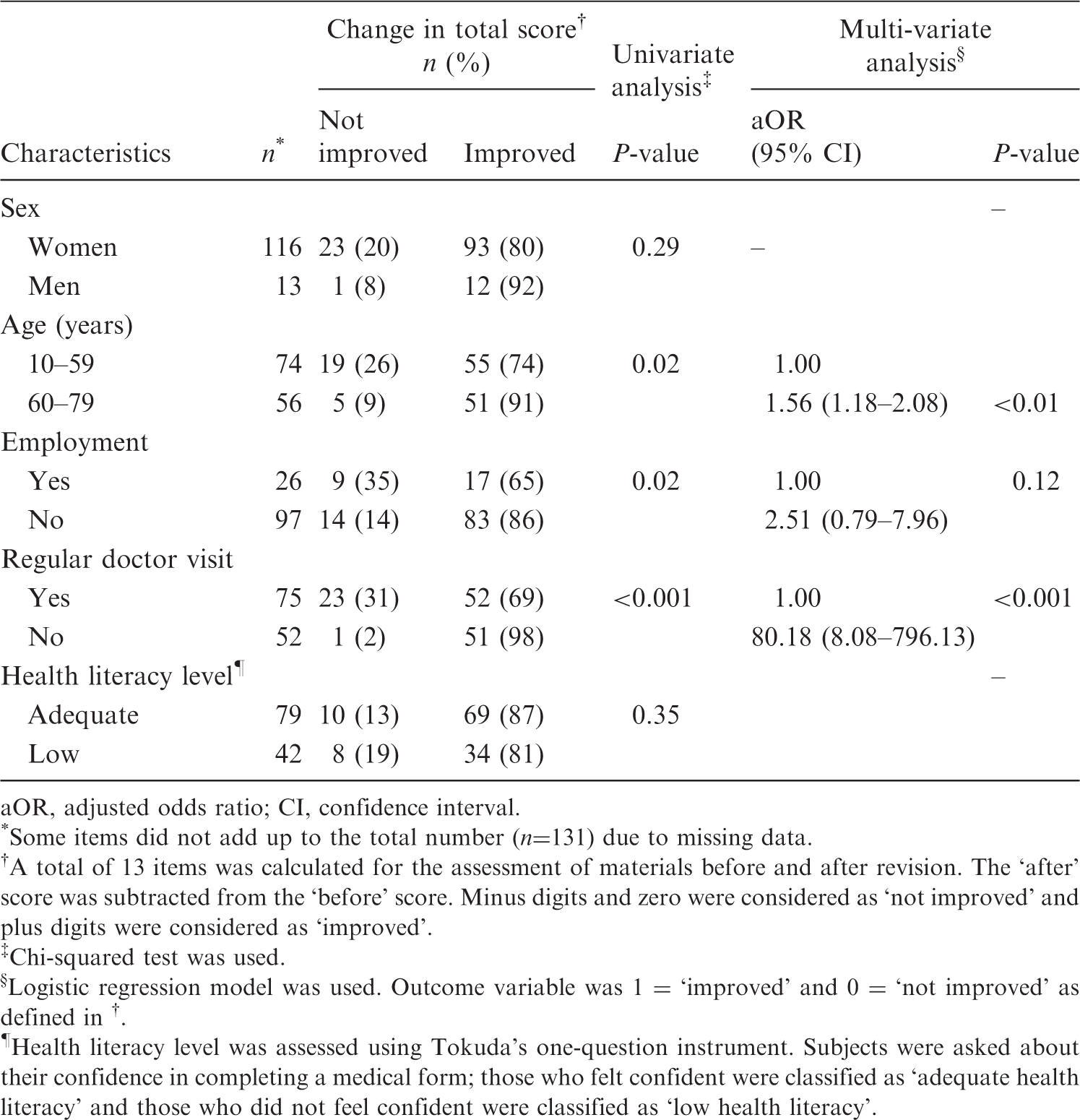
aOR, adjusted odds ratio; CI, confidence interval.
Some items did not add up to the total number (n=131) due to missing data.
A total of 13 items was calculated for the assessment of materials before and after revision. The ‘after’ score was subtracted from the ‘before’ score. Minus digits and zero were considered as ‘not improved’ and plus digits were considered as ‘improved’.
Chi-squared test was used.
Logistic regression model was used. Outcome variable was 1 = ‘improved’ and 0 = ‘not improved’ as defined in †.
Health literacy level was assessed using Tokuda’s one-question instrument. Subjects were asked about their confidence in completing a medical form; those who felt confident were classified as ‘adequate health literacy’ and those who did not feel confident were classified as ‘low health literacy’.
In the reports that training participants submitted with their feedback assessment data, they wrote about recognising the importance of altering material content in accordance with the aim of providing information, and the characteristics of the intended audience. One nurse wrote, ‘it is important to make it a routine to have difficult parts reviewed by the intended audience and revise based on their comments’.
4. DISCUSSION
A clear improvement was observed in the accessibility of written health information following health literacy training. Technically, supplementary explanations in parentheses, and, more intrinsically, conveying the main message clearly requires careful attention when developing materials. Incorporating the feedback assessment survey into the training served two purposes: evaluation of the revised materials by the intended audience; and the provision of training for participants to help recognise the importance of obtaining feedback from the intended audience, as described in their submitted reports. One of the teaching tools in this training programme is the translated version of the US Centres for Disease Control and Prevention’s clear communication index. This tool assesses the accessibility of both text and numerical information. Prior to scoring, the index asks users to identify the characteristics of the intended audience in addition to the aims of the information provided. This message was well conveyed in the study workshop, and the recent training evaluation reported that participating nurses had more positive attitudes towards feedback from community members compared with non-participants (Yumiya et al., 2000).
This study found that feedback assessment respondents who were elderly and did not have regular doctor visits were more likely to notice improvement in the materials. One nationwide survey in Japan reported that the elderly were less confident about seeking health information (Ishikawa et al., 2012). Their vulnerability to access information could be enhanced by advancing technology. Another national survey among the elderly in the USA found a negative loop between low health literacy and use of the internet; elderly people with low health literacy tend not to use the internet to obtain health information and are left behind in the digital information age (Levy et al., 2014). This does not only affect elderly people; as Protheroe et al. (2009) wrote, ‘a person can be literate within a familiar environment and context, but functionally illiterate when required to comprehend and respond to unfamiliar vocabulary and concepts in an unfamiliar environment’. Healthcare settings are unfamiliar environments for many, and universal precaution is key to promoting health literacy at health organisations (Brega et al., 2015). This training programme showed that one way of reaching out to populations at risk of not receiving health information is to train health professionals to have a health literacy perspective and skills.
This study had two main limitations. First, results from the analysis regarding who gained the greatest benefit from the improved materials need to be interpreted cautiously. It is not conclusive whether the materials assessed among the non-elderly were less improved or whether the elderly actually gained greater benefit from the revision. Second, a conventional one-question item was used to assess the health literacy level of respondents in the feedback assessment. Use of a more precise measure may have resulted in a significant association with health literacy level rather than age and familiarity with health services.
Almost a decade has passed since the accident at Fukushima Daiichi nuclear power plant. Since then, the authors have developed, implemented, continuously evaluated, and upgraded their health literacy training. The training programme is expanding to integrate the workshop into medical and nursing education (Murakami and Goto, 2019) and on-the-job training for various health professionals within and outside Fukushima. Such training could serve as a model programme to prevent inequity in access to health information in the face of a health crisis.