
Abstract
This paper does not necessarily reflect the views of the International Commission on Radiological Protection.
Keywords
1. RISK PERCEPTION TODAY
Almost 35 years after the accident at Chernobyl nuclear power plant, life in radioactively contaminated areas (RCAs) in Russia have basically returned to normal, with the exception of some aspects of social well-being associated with perceived radiation risk. Indeed, in the national ratings of social and economic well-being and quality of life, the four most contaminated regions in Russia are consistently placed in the middle of the list (RIA Novosti, 2019). At the same time, in the eyes of the residents of RCAs, the radiation-induced consequences for their health remain clear. Chernobyl-related payments from the budget are ongoing; both the public and the authorities (both regional and federal) have no doubt that this is compensation for the radiation effects. Residents have long come to terms with the additional risk, but the economic dimension of this issue continues to be relevant for them. Monetary compensation is a permanent measure, and, naturally, the RCA residents want it to remain for the long term. The federal authorities, referring to scientists, say that the radiation doses do not exceed the established standards, and in the overwhelming majority of cases, health consequences are not expected; therefore, compensation seems to be unnecessary. In 2016, the Russian Government announced the completion of federal programmes to help regions affected by the radiation from Chernobyl. However, attempts by the federal authorities to cancel individual payments and benefits stipulated by the law are blocked at regional level.
Perception of the inevitability of serious consequences for health from radiation, regardless of the dose, is characteristic of both the affected people and society as a whole. In 2012, answering the question about the number of deaths from radiation exposure after the accidents at Chernobyl and Fukushima Daiichi nuclear power plants, respondents in 45 regions of Russia extrapolated this perception to people who could be exposed. The gap between the respondents' assessments and the actual statistics was three to four orders of magnitude, and this was essentially independent of the age, education, social status, and place of residence of the respondents (Fig. 1) (Melikhova et al., 2013).
Distribution of respondents' answers to the question ‘In 1986 there was an accident at the Chernobyl nuclear power plant. In your opinion, how many people died from radiation exposure as a result of this accident?’ Results given as percentage of the total number of respondents. The survey was conducted by the Russian sociological service ‘The Public Opinion Foundation’ on 26–28 October 2012; 1500 people were interviewed at their place of residence in 44 regions of the Russian Federation.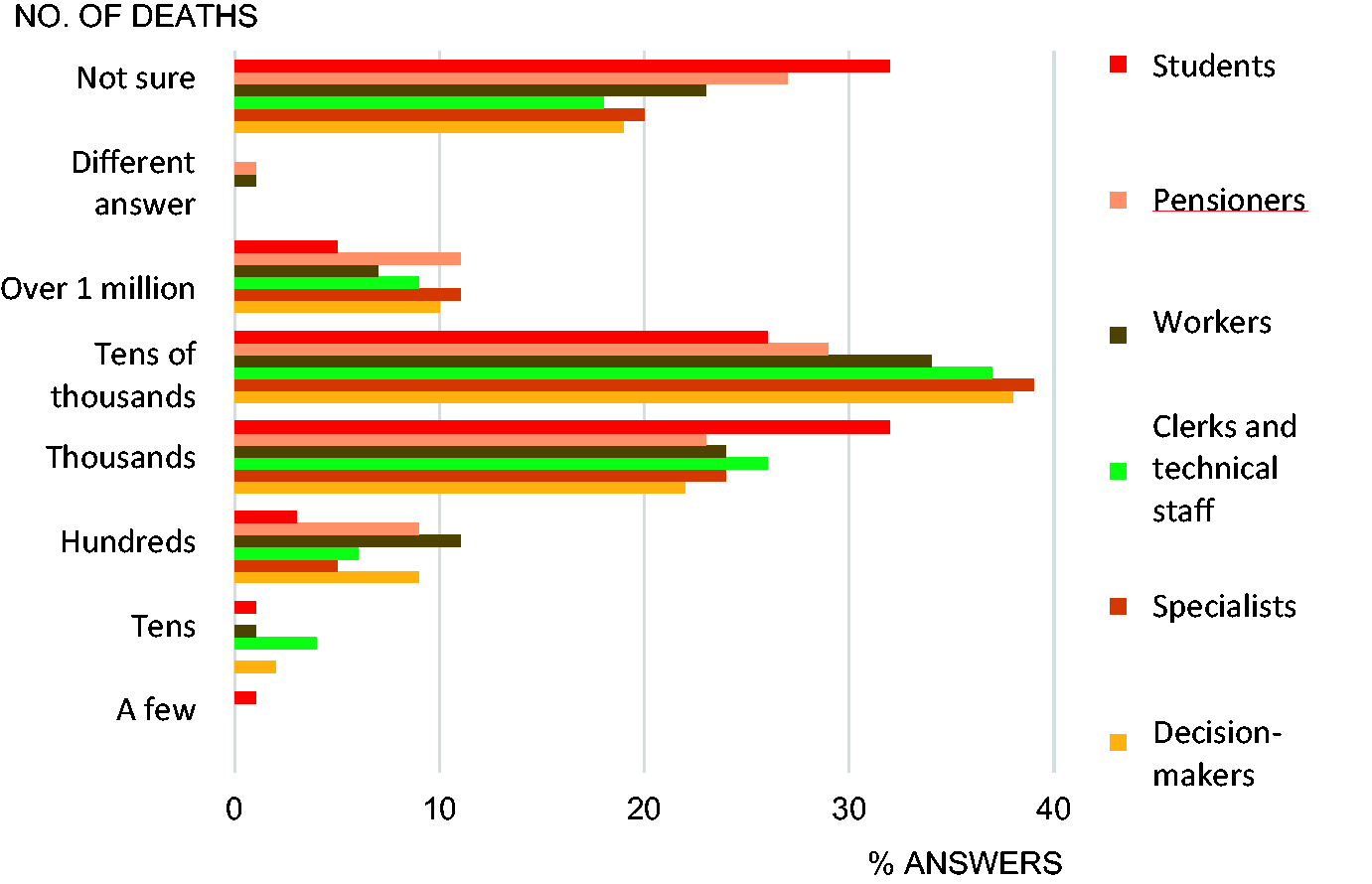
2. THE KEY ROLE OF RISK PERCEPTION IN THE TRANSITION TO RECOVERY
Leading Soviet radiologists and radiation protection specialists (RP experts) faced the problem of a specific public perception of low-dose radiation risk in the late 1980s, when the Government put forward the concept of living safely in the areas with residual radiation contamination developed by the National Commission on Radiation Protection of the USSR (NCRP) for broad public discussion (Ilyin, 1995). The leitmotif of this concept was the removal of restrictions on the mode of life for people living in the zone of strict control, and ensuring that the established level of lifetime dose was not exceeded. From the radiologically acceptable range (≤1 Sv in 70 years), after long discussions, 350 mSv was chosen as an intervention criterion for the critical group of the population (children). Such a level, on the one hand, ensured compliance with the national radiation safety standards; however, on the other hand, it made it possible to ensure a high degree of protection of the population at significantly lower material cost (IBRAE, 2016).
However, this option for optimising RP did not receive the support of either society or international experts invited by the Soviet Government in 1989 for a comprehensive assessment of the protective measures proposed by domestic scientists, including the ‘350 mSv’ concept. The reasons for criticism were diametrically opposed. Leading foreign scientists assessed the concept as overly conservative. The international Chernobyl project, in which nearly 300 leading experts worldwide participated, including experts from the World Health Organization, the Food and Agriculture Organization, and the International Atomic Energy Agency, lasted for 3 years. During this time, as well as the decisions made, the entire situation in the contaminated areas, including the health status of residents, was assessed. Criticising the ‘350 mSv’ concept, foreign scientists noted excessive conservatism in assessing life-long doses, including account for the doses already received by the population. In their opinion, in the post-Chernobyl situation, the criterion for resettlement could be higher (Ilyin et al., 2016).
On the contrary, Soviet society, including the medical and scientific elite, considered it unfair and inhumane to suggest that people innocent of the accident should take additional health risks by living in contaminated areas, regardless of the small size of the risk. The authors of the ‘350 mSv’ concept were accused of inhumanity, attempts to destroy the gene pool of the nation, etc.
Completely ignoring the findings of the International Chernobyl Project, the Soviet Government sided with the public and supported an alternative concept that followed the public perception of risk. The good intention to broaden social support measures to those who were ‘to live with Chernobyl radiation’ led to the adoption, in 1991, of a law that drastically increased the area of territories where protective measures were applied. The number of residents affected by these measures increased from 0.5 million to 7 million (Arutyunyan et al., 2016).
3. COMMUNICATION EFFORTS OF RP EXPERTS
3.1. Communication at federal level
Subsequently, the Russian RP experts tried to convey the following arguments to the federal authorities and legislators: (i) radiological consequences of the accident, including medical consequences, are limited; and (ii) establishment of compromise and, in fact, incorrect criteria for classifying areas as ‘exposed to radiation’ in legislation led to unjustified scaling of non-radiological consequences.
In the conditions of a severe economic crisis, the Russian authorities realised within 2–3 years that it would be impossible to fulfil the social obligations guaranteed by the law in full, and began to listen to the RP experts again. At federal level, more favourable conditions for risk communication emerged. However, to obtain verified and methodologically consistent estimates of the true causes of deterioration in public health indicators, years of observation were required. At the same time, the situation was different at regional level. Counting on funding from the federal budget, the ruling elites of the contaminated territories of 19 regions presented more and more ‘evidence’ of radiation consequences for the health of the population. The legislative decision to involve medical authorities in the search for radiation consequences, as well as relatively good funding against a backdrop of chronic underfunding of non-Chernobyl research fields, led to a tangible influx of scientists from other fields without special radiological education. As a result, a powerful stream of hasty and methodologically untenable ‘evidence’ of radiation consequences fell upon the RCA residents and the public (Melikhova et al., 2012).
By the 10th anniversary of the accident, the Russian Government, solving the acute problems of the budget deficit, adopted the dose concept and prepared amendments to the Chernobyl legislation. However, over the same period, the management paradigm had not changed at all: monetary compensation can only be provided for radiation exposure; non-radiation consequences for the population because of the Chernobyl accident are not an issue. It is not surprising that the federal government's attempts to cut payments from the federal budget have repeatedly encountered tough resistance from the population and regional authorities. Government opponents turn the management paradigm to their advantage: if money is provided, there are consequences. The Chernobyl law on social protection is still in force; society is not ready to abandon it.
The continuing status quo in Chernobyl legislation shows the long-term consequences of overtly broad interpretation of the areas that ‘suffered’ from radiation and their residents. These are political costs (forced continuity of outdated legislation and inability of ‘playing back’ in fear of public protest), economic problems of the areas (Chernobyl status ‘does not attract money’), and permanent reproduction of public ideas about the danger of radiation in general and radiation from Chernobyl in particular.
3.2. Communication with concerned residents and the public
Much effort has been invested in informing concerned residents of RCAs and the public about the scientific position regarding the consequences of the Chernobyl accident through federal and regional media. In the late 1980s and early 1990s, the accident and its consequences were extremely painful topics for the post-Soviet society, and the media was almost completely closed to RP professionals. Over time, journalists have become more willing to lend a voice to scholars challenging public consensus. However, RP experts were only one side in the dialogue and often gave conflicting assessments. No matter how successful their media appearances, they could not change anything.
Public opinion about the scale of the medical consequences of the accident largely originates from the belief that radiation is dangerous at any dose. RP experts cannot say that this is not true, as the linear non-threshold (LNТ) hypothesis is the core assumption for radiation safety regulation.
The LNT hypothesis confuses the medical community and regulators, provoking unwarranted hygiene fears, including lowering regulatory levels and looking for evidence of harm to public health in the low-dose range. Stochastic effects have a long latency period, so medical and epidemiological programmes stretch over decades. National experts from different scientific schools interpret the intermediate results obtained in opposing ways. As a result, three decades later, RP professionals cannot give an unambiguous answer about the actual number of victims of the radiation accident (Astafiev, 2016; NMRRC, 2016; Tukov et al., 2020).
RP experts participating in various measurement programmes in contaminated areas were looking for effective ways to influence the perception of radiation hazard by RCA residents. Some lessons of risk communication in a situation where negative expectations about health have already formed, together with mistrust of visiting scientists for collection of experimental material and who do not want to delve into the real problems of the residents, can be summarised as follows.
First, it is necessary to demonstrate the safety of living in the contaminated areas, and only then convince. Generally, specialists who travelled with their families to the contaminated south-western districts of the Bryansk region, and lived there as rural residents, were able to overcome the mistrust of local authorities and residents, and explain their arguments. Radiation risk should be communicated in a context relevant to local communities. It makes no sense to talk to people about the risk and to give scientific arguments if they are worried about other aspects. For example, in the late 1990s, residents of the south-western districts of the Bryansk region were very sensitive to a possible reduction in Chernobyl benefits. In one of the conversations, this concern was voiced as follows, ‘Why are you telling us that we have little radiation? We are ready to eat radiation with a spoon if paid for it’. The dominance of economic interests was also demonstrated in the course of sociological surveys in the autumn of 2003. Answering the question ‘What worries you the most today?’, residents chose the option ‘low standard of living’ three times more often than ‘radioactive contamination’ (ICRIN, 2005). The high professional qualifications of an expert must be complemented by a wealth of life experience and personal charisma. To influence people's opinions, an expert must not only be able to answer questions about individual risks in different situations, but must also understand how these people think, what they believe, and how to put their own ideas into the population’s belief system with minimal resistance. Trust in information is formed through trust in the personality of an expert. The tasks of experts do not usually include immersion in the problems of the local community and individuals; it remains a personal choice. Experience in contaminated areas has confirmed the thesis that empathy and compassion are much more important than the risk information provided (Covello, 2014). Information will not necessarily be perceived, especially the first time, but respect for people's needs will be appreciated. It is often difficult for RP experts to admit that not all people are willing to act logically on risk information. The fear of radiation is a normal human reaction. Telling anxious people that there is nothing to be afraid of (i.e. it is stupid to be afraid) is counterproductive. In such situations, one should focus on rational measures to manage individual risks. Subjective risk perception is formed under the influence of different and often contradictory information signals coming from different sources. To explain the apparent contradictions, one needs to understand the positions of all interested parties, and put radiation risk into perspective. Many years of personal experience of a normal ‘life with radiation’ does not lead to automatic correction of the subjective perception of radiation risk which has developed under the influence of generally accepted ideas. The task of reformatting generally accepted concepts requires systemic approaches at state level (professional development of doctors, teachers, etc.). At state level, this task is not set as it is much easier to maintain the status quo in the current situation.
4. CONCLUSIONS
To conclude, the perception of radiation risk by society is a complex and still poorly studied social phenomenon that plays a key role in decision-making during the recovery stage. After the accident at Chernobyl nuclear power plant, it was the public perception of risk that led to rejection of the NCRP/International Commission on Radiological Protection approaches to risk management in the low-dose range. In the conditions of a severe economic crisis, the federal authorities quickly recognised the need to switch to scientifically based dose criteria, but they are still not ready to recognise the responsibility of the state for non-radiation consequences. Therefore, it has not yet been possible to ‘play back’ and change the Chernobyl legislation.
The absence of changes in the public perception of radiation risk indicates the low efficiency of the communication efforts of the RP community, based on a simplified approach of ‘explaining risks in simple language’. One of the main barriers is disagreement between RP professionals regarding the validity and expediency of using the LNT hypothesis in the range of fundamental scientific uncertainty. The significance of a consolidated expert opinion for public perception of risk is clearly underestimated, and there are certain reasons to believe that the issues discussed go far beyond the national boundaries of the Russian Federation.