
Abstract
Due to vigorous efforts to decontaminate the environment following the accident at Fukushima Daiichi nuclear power plant, the size of the difficult-to-return zone has reduced significantly and people have started returning to their homes. As the population has increased, medical needs have ensued. A marked increase in traffic as well as decontamination and reconstruction projects has led to an increase in the number of road traffic and occupational accidents. Acceleration of population aging has resulted in an increased number of elderly residents with multiple medical problems. Uncontrolled/untreated medical problems among middle-aged to older workers have made them susceptible to deterioration of health conditions. Insufficient social support for elderly people living alone has resulted in delayed access to medical care. Early intervention and the prevention of health deterioration are instrumental. When responding to medical needs, proactive approaches, including home visits for elderly patients and health promotion, have been implemented. Human resource development is crucial to ensure the sustainability of these activities.
1. Background
Since the accident at Fukushima Daiichi nuclear power plant (NPP), vigorous efforts have been made to decontaminate the environment. The size of the difficult-to-return zone has reduced significantly and people have started returning to their homes.
Soon after the accident, 12 municipalities, including eight towns and villages in Futaba region, were ordered to evacuate. In total, 98,000 people were evacuated. In 2014, the Japanese Government started lifting the evacuation order for Kawauchi Village, and this was extended gradually to other municipalities. In 2019, the evacuation order was lifted for the first time in part of Okuma Town, the municipality where Fukushima Daiichi NPP is located. Currently, 22,000 people live in areas where the evacuation order has been lifted. The difficult-to-return zone has now reduced to one-third of its size in 2011, representing 2.7% of Fukushima Prefecture.
As the population living in areas where the evacuation order was lifted has increased, medical needs have ensued. For example, the number of calls to the emergency medical services (EMS) in Futaba region has been increasing by 10% every year for the last 6 years (Fukushima Prefecture, 2019). The main reasons for EMS calls are acute illnesses. However, there has been a marked increase in traffic, as well as decontamination and reconstruction projects, and the proportion of injuries caused by road traffic and occupational accidents is much higher in these areas than national data. Also, interhospital transfer is more common than the national average. This reflects a shortage of medical resources in areas where the evacuation order was lifted. Until Futaba Medical Centre (FMC) was established, there was no emergency hospital in this region.
2. Development of medical service systems in Futaba region
Before the accident at Fukushima Daiichi NPP, there were 100 medical facilities in Futaba region (Fig. 1). After the accident, all medical facilities within 20 km of the NPP were forced to close, and only four medical facilities around the evacuation zone continued or recommenced medical practice soon after the accident. Since some of the evacuation orders have been lifted and people have started returning to their homes, medical needs have grown. Several outpatient clinics have re-opened; however, medical practice in the area is difficult due to a shortage of medical staff, the financial burden, and uncertainty about the future.
Medical facilities in areas where the evacuation order has been lifted (as of 1 April 2020).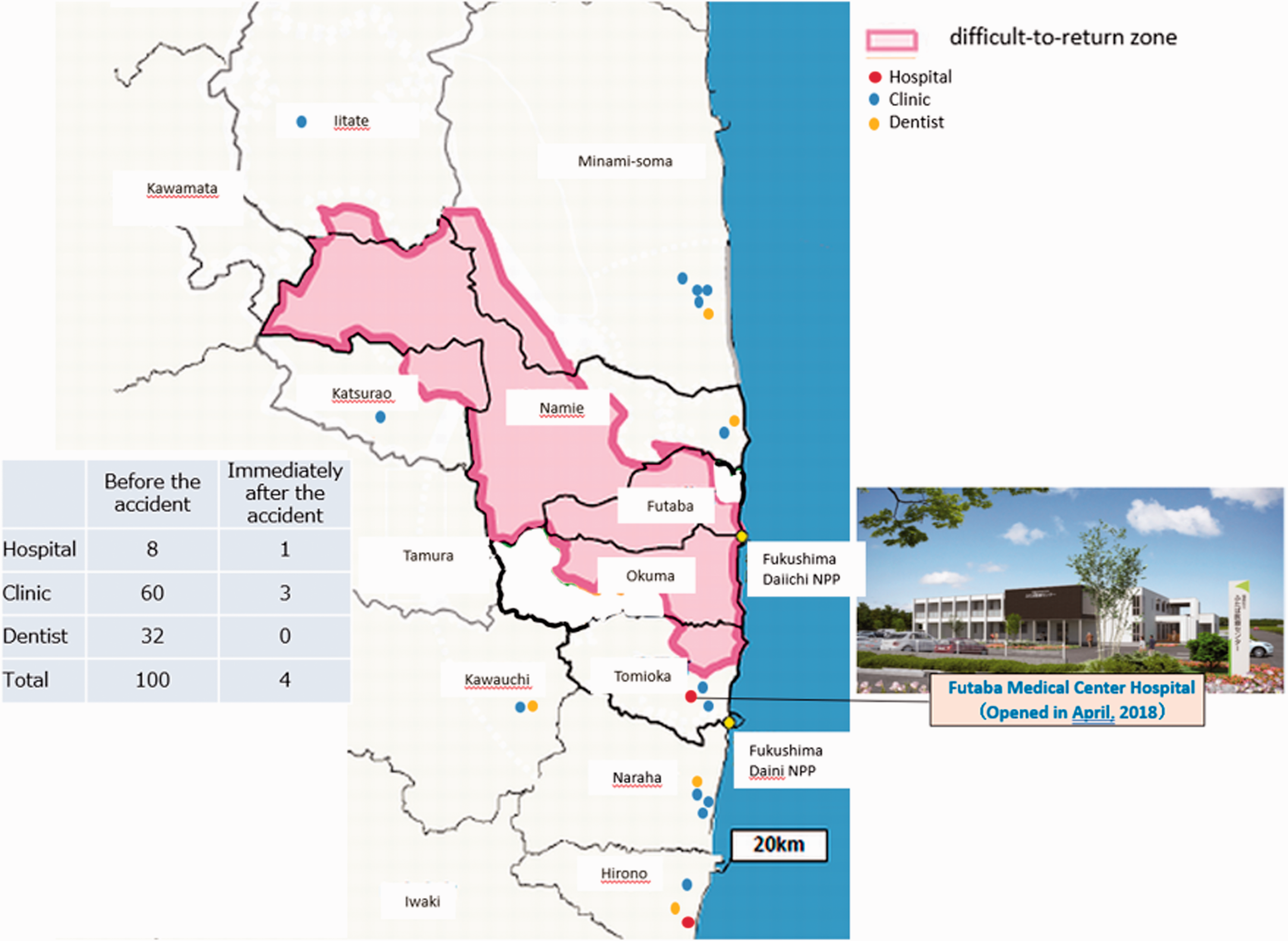
Acceleration of population aging has resulted in an increase in the number of elderly residents with multiple medical problems requiring careful medical attention. Uncontrolled/untreated medical problems among middle-aged to older workers have made them susceptible to deterioration of health conditions, requiring emergency and more intensive treatment. Insufficient social support for elderly people living alone has resulted in delayed access to medical care.
To respond to increasing emergency medical needs in Futaba region, Fukushima Prefectural Government established an emergency hospital – FMC – in Tomioka Town in 2018. FMC is located 8 km south-west of Fukushima Daiichi NPP. The main role of FMC is to provide emergency medical care and disaster responses, including radiological emergency responses. Although it is a small hospital with 30 beds, it operates 24 h per day, 7 days per week, 365 days per year to meet local emergency needs. Also, it is expected to provide home care and contribute to comprehensive community care following the return of elderly people with physical disabilities to the area. Health promotion efforts are required for residents with multiple medical problems and workers with health risks such as diabetes and hypertension. In order to achieve these goals, good collaboration is needed with other medical facilities, healthcare providers, and local municipalities inside and outside the region. In particular, good cooperation with Fukushima Medical University is prerequisite to ensure the quality of care and continuity of projects.
Over the last 2 years, FMC has responded to 60% of emergency medical needs in Futaba region (Miyagawa and Tanigawa, 2020). The number of emergency room (ER) visits increased by 50% in 2019 compared with the previous year. Regarding the areas of residence of patients, Naraha, Tomioka, and Hirono account for more than half of patients, reflecting the populations of these municipalities and their proximity to FMC. Patients from outside Futaba region or Fukushima Prefecture account for 35% of ER visits. These patients have mainly suffered injuries due to road traffic or occupational accidents. Two peaks have been observed in the age distribution of patients: 50–59 years and >80 years. Injury is the most common reason for visiting the ER, followed by respiratory problems. The younger group generally visit the ER with injuries, and the older group generally present with respiratory problems. Regarding admitted patients, those aged >80 years account for 60% of admissions. Similar to diagnoses in the ER, the two main reasons for admission are injury and respiratory problems. Most injuries requiring admission are fractures related to osteoporosis, and the majority of respiratory problems are due to pneumonia. Osteoporosis and pneumonia are very common medical problems among elderly people. Patients with major trauma, acute myocardial infarction, or acute stroke require advanced medical intervention, and are generally transferred to designated medical facilities such as level 1 trauma centres or stroke centres outside the region, such as in Iwaki or Minamisoma.
Health issues are not limited to medical problems. More than 40% of residents are aged >65 years and most of them have chronic illnesses. Early intervention and the prevention of health deterioration are instrumental. There is a need to undertake more home visits for elderly patients. There is also a need for health promotion in collaboration with local municipalities, such as holding educational seminars for residents and comprehensive community care events. The key concept is a proactive approach. In order to address family and community issues, it is imperative to get involved in comprehensive community care, which is organised by the municipal government and social welfare liaison. Last but not least, development of human resources is crucial to implement the abovementioned activities. Close collaboration with academic institutions, organisations, and municipalities is needed.
3. Issues and Challenges
Evacuation orders have been lifted and people are returning. However, 80% of former residents have not yet returned. What do they think?
In Tomioka and Namie Town, where the evacuation order has been lifted for 3 years, those who have already returned or wish to return account for only 16–18% of the population (Reconstruction Agency, 2019). Approximately half of the residents have decided not to return. In Okuma and Futaba Town, where the evacuation order was lifted most recently, only approximately 10% of former residents want to return and 60% have decided not to return. Most former residents have re-established their lives in the evacuation site. The longer the evacuation order is in place, the fewer people want to return. It has been reported that concerns about consuming locally sourced food and tap water in Tomioka were significantly more prevalent among those who were undecided about returning and those who had decided not to return compared with residents who had returned to their homes in Tomioka (Orita et al., 2020). The proportion of residents who felt that cancer would occur due to radiation exposure and that genetic effects would arise in the next generation due to living in Tomioka was significantly higher among those who decided not to return and those who were undecided about returning. Studies have indicated that the perception of risk of radiation exposure was closely associated with the intent to return home. Given their well-being and re-established lives in the evacuation site, it would not be unreasonable to say that returning is one of the options, not the only option.
There are two challenges here: universality and rarity. Firstly, before the nuclear accident, Futaba region had been suffering from an aging population, depopulation, and a shortage of medical resources. The accident at Fukushima Daiichi NPP underscored those issues. However, in Japan, these issues are not unique to Futaba region, and the accident clearly highlighted medical and public health issues that exist elsewhere in the country. The other challenge is rarity; trying to rebuild a sustainable community where all residents were once evacuated after a major nuclear accident is unprecedented. These experiences provide a basis for future planning following a major nuclear accident.