
Abstract
Objective:
This study aimed to investigate the clinical features and risk factors of otomycosis.
Methods:
A case-control study included 160 patients with otomycosis as the case group and 320 healthy individuals as the control group. Clinical data were collected through a standardized questionnaire, including habitual ear picking, ear cleaning at salons, swimming habits, use of earphones/hearing aids, external auditory canal stenosis, and presence of diabetes. Binary logistic regression analysis was used to determine the risk factors.
Results:
The most common symptom was ear fullness/blockage (28.3%). Otoscopic examination before debridement most frequently revealed external auditory canal secretions (45.2%). Aspergillus species were the predominant pathogens, accounting for 80.0% of cases. Binary multivariable logistic regression analysis identified the following as significant risk factors for otomycosis: habitual ear picking (OR = 2.748, 95% CI: 1.669-4.525, P < .001), ear cleaning at salons (OR = 7.434, 95% CI: 3.023-18.281, P < .001), and external auditory canal stenosis (OR = 3.737, 95% CI: 2.384-5.857, P < .001). Swimming habits, frequent use of earphones/hearing aids, and diabetes were not significantly associated with otomycosis.
Conclusion:
Frequent ear picking, ear cleaning at salons, and external auditory canal stenosis are major risk factors for otomycosis.
Introduction
Otomycosis is a common otologic condition frequently encountered in otolaryngology, particularly prevalent in warm and humid subtropical regions. It may present with symptoms such as otalgia, hearing loss, tinnitus, ear fullness or blockage, pruritus, and otorrhea, 1 and is often characterized by recurrent episodes that are difficult to completely eradicate. Therefore, identifying risk factors for otomycosis is crucial for its prevention and for reducing recurrence rates. Various potential risk factors have been proposed, including humid climates, ear picking, immunocompromised status, 2 use of topical antibiotic ear drops, 3 and the presence of cerumen.4 -7 Regional variations in risk factors have also been observed, for example, ear picking is popular in China, while in other countries, practices such as applying coconut oil 8 or wearing headscarves or veils9,10 have been implicated. However, current research on the risk factors for otomycosis remains limited and often lacks methodological rigor, Many studies have not included control groups 6 or have not used regression analysis, 8 making it impossible to determine whether a factor is an independent risk factor. In contrast, the present study included a control group and applied binary multivariable logistic regression to more rigorously identify independent risk factors for otomycosis, which provides strong evidence for assessing whether certain risk factors reported in the existing literature are indeed independent risk factors.
Patients and Methods
Study Design
This study adopted a case-control design and was approved by the Ethics Committee of Zhongshan Hospital of Xiamen University (registered at ClinicalTrials.gov, Registration number: NCT06530069). It is a retrospective study involving adult patients diagnosed with otomycosis in the outpatient department of Zhongshan Hospital of Xiamen University, between April 2024 and June 2025. The sample size was determined by the number of available otomycosis cases during the study period, with controls selected at a 1:2 gender-matched ratio to optimize statistical power. A total of 160 eligible patients were consecutively enrolled during the study period, including 90 males and 70 females, aged 19 to 89 years, with a median age of 38.0 years. The control group consisted of 320 individuals undergoing routine health checkups at the hospital’s physical examination center. These participants reported no ear-related symptoms and were confirmed to be free of otomycosis upon otologic examination. Controls were enrolled consecutively with gender stratification, including 180 males and 140 females, aged 18 to 93 years, with a median age of 41.5 years.
The case group was assessed for the clinical features of otomycosis. Both the case and control groups completed a standardized questionnaire, which included the following items: (1) habitual ear picking (≥1 time per week); (2) history of professional ear cleaning at salons; (3) swimming habit (on average ≥2 times per week during summer); (4) regular use of earphones or hearing aids (use on ≥2 days per week, for at least 30 minutes each time); (5) presence of external auditory canal stenosis (determined via otoscopic examination, where the whole tympanic membrane is difficult to visualize even in the absence of cerumen); (6) history of diabetes.
Inclusion criteria: For the case group, patients presented with symptoms such as tinnitus, ear fullness or blockage, pruritus, otalgia, otorrhea, and hearing loss. Physical examination findings included fungal hyphae, crusts, secretions, and masses within the ear canal. A positive fungal culture result was required for inclusion. The control group exhibited none of these symptoms or findings.
Exclusion criteria: Patients with otitis media, tympanic membrane perforation, or those who had undergone radiotherapy were excluded.
Statistical Methods
Statistical analyses were performed using SPSS version 27.0 (IBM SPSS, Armonk, NY, USA). The age difference between the case and control groups was compared using the non-parametric Mann-Whitney U test. For univariate analysis, univariate logistic regression was performed to estimate odds ratios (ORs) with corresponding 95% confidence intervals (CIs) for each potential risk factor and for comparing ear-picking tools between the 2 groups. Analysis of risk factors was conducted using binary multivariable logistic regression. P < .05 was considered statistically significant. All candidate variables were entered simultaneously into the multivariable logistic regression model using the enter method, without stepwise selection.
Results
Clinical Features of the Case Group
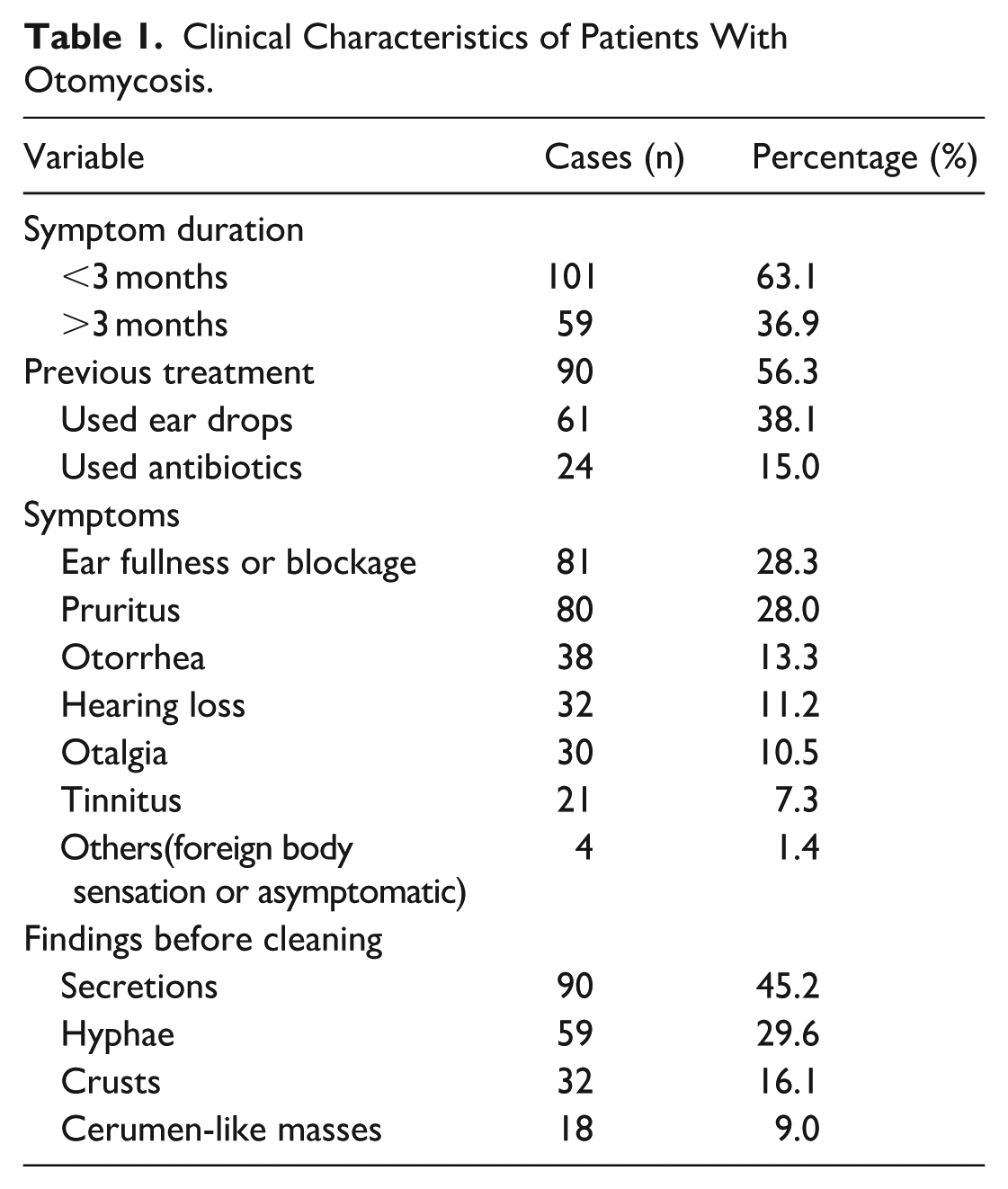
In the case group, the proportion of male patients (56.3%) was slightly higher than that of females (43.8%). Bilateral ears involvement was most common (36.9%), while among unilateral cases, the left ear (35.0%) was affected more frequently than the right ear (28.1%). Clinical information is summarized in Table 1. More than half of the patients (63.1%) had a short disease duration (<3 months), and the majority (56.3%) had received prior treatment, with ear drops being the most commonly used intervention (38.1%). Regarding symptom distribution, ear fullness or blockage (28.3%) and pruritus (28.0%) were the most frequently reported, together accounting for over half of the cases. On otoscopic examination prior to cleaning, the presence of secretions (45.2%) and fungal hyphae (29.6%) were the most prominent features.
Clinical Characteristics of Patients With Otomycosis.
Distribution of Fungal Culture Results
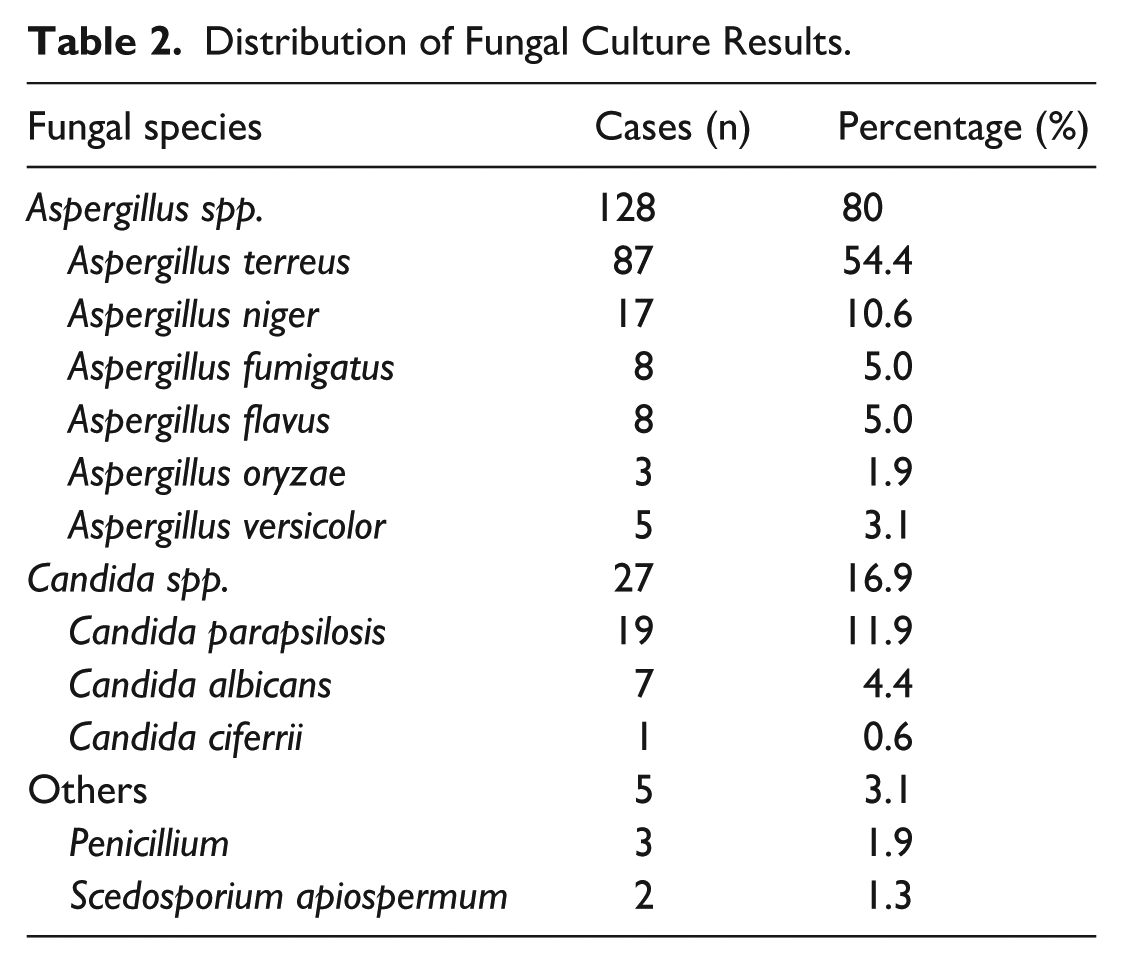
The distribution of fungal culture results is presented in Table 2. Aspergillus species were the overwhelmingly dominant pathogens, accounting for 80% of all isolates. Among these, Aspergillus terreus was the most prevalent species (54.4%), followed by Aspergillus niger (10.6%) as the second most common. Candida species represented a minority of isolates, with Candida parapsilosis being the predominant yeast (11.9%). Other fungal species were rare and infrequently detected.
Distribution of Fungal Culture Results.
Univariate Screening of Risk Factors for Otomycosis
Univariate screening revealed that the proportions of habitual ear picking, professional ear cleaning at salons, and external auditory canal stenosis were significantly higher in the case group compared to the control group (P < .05), indicating statistically significant associations. In contrast, no significant differences were observed between the 2 groups in terms of swimming habits, frequent use of earphones/hearing aids, and the presence of diabetes mellitus (see Table 3).
Univariate Analysis of Risk Factors for Otomycosis.
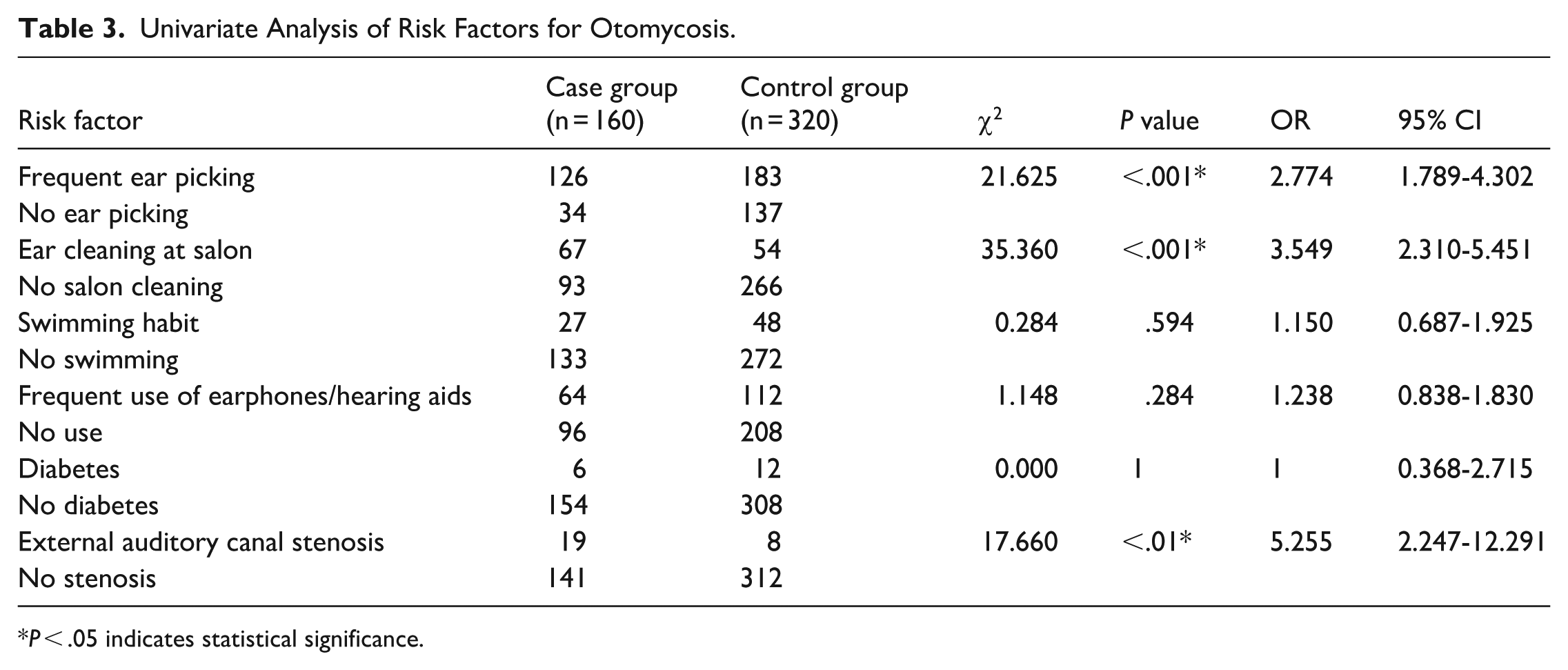
P < .05 indicates statistical significance.
Binary Multivariable Logistic Regression Analysis of Risk Factors
A binary multivariable logistic regression analysis (Table 4) was performed to identify independent risk factors for otomycosis. The results indicated that professional ear cleaning at salons, external auditory canal stenosis, and habitual ear picking were all significantly associated with an increased risk of the disease (all P < .001). Among these factors, professional ear cleaning at salons showed the strongest association, with an OR of 7.43 (95% CI: 3.02-18.28), suggesting that individuals who undergo this practice are over 7 times more likely to develop otomycosis. This was followed by external auditory canal stenosis (OR = 3.74, 95% CI: 2.38-5.86) and habitual ear picking (OR = 2.75, 95% CI: 1.67-4.53). The effect sizes of all candidate variables in the multivariable model are illustrated in a forest plot.
Independent Risk Factors for Otomycosis.
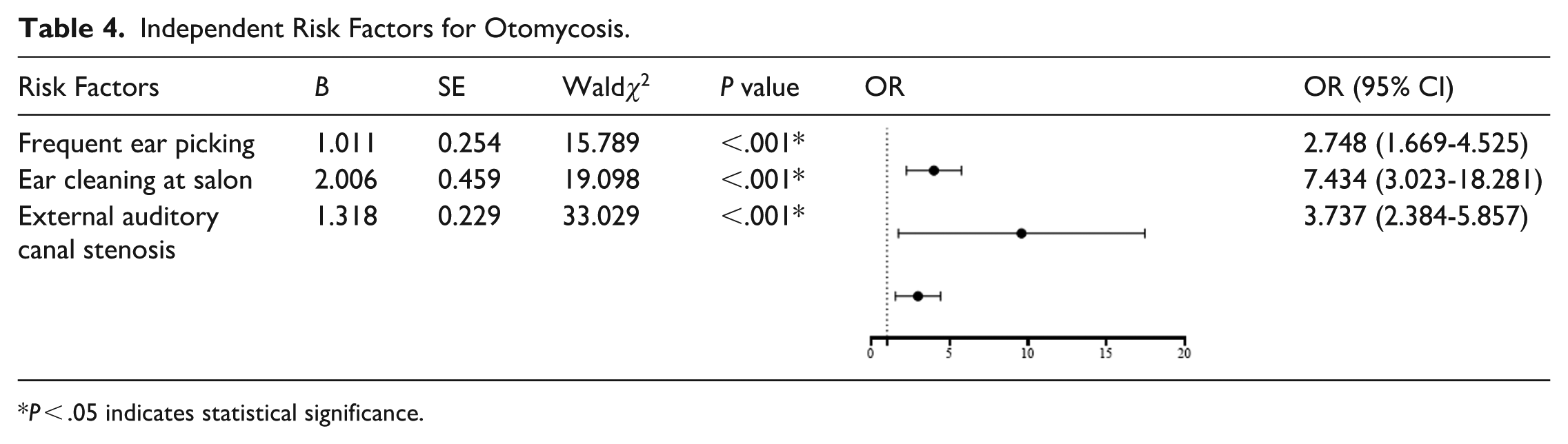
P < .05 indicates statistical significance.
Comparison of Ear-Picking Tools Between Case and Control Groups
As shown in Table 5, there was no statistically significant difference in the choice of ear-picking tools between the case and control groups (P = .603). In both groups, cotton swabs were the most commonly used tool (58.7% in the case group vs 59.0% in the control group), followed by ear scoops (27.8% vs 29.0%, respectively).
Comparison of Ear-Picking Tools Between Case and Control Groups.

Discussion
Otomycosis is a common condition with a high incidence rate. It is often misdiagnosed, requires a prolonged treatment course, and imposes both time and economic burdens on patients. Identifying its independent risk factors and promoting community-based health education could play a crucial role in disease prevention and in reducing recurrence after treatment, thereby carrying significant clinical and public health implications.
Our study identified several notable clinical features and diagnostic challenges associated with otomycosis. Unilateral infection was the predominant presentation, accounting for 63.1% of cases. Interestingly, left ear involvement was more common than right ear, which may be attributed to the non-dominant hand being more prone to causing trauma during ear picking. This finding contrasts with that of Borlingegowda Viswanatha, 2 who reported a higher incidence in the right ear, attributing it to the dominance of the right hand and its more frequent use in ear cleaning. In terms of disease duration, acute cases (history <3 months) accounted for the majority (63.1%), while chronic cases (history >3 months) made up 36.9%. Pruritus was the most frequently reported symptom of otomycosis, although some patients also experienced otalgia. Notably, the presence of characteristic fungal hyphae was not a dominant clinical sign, observed in only 29.6% of patients. In contrast, non-hyphal manifestations were more common, with secretions (45.2%) and crusts (16.1%) being the primary clinical features. Aspergillus species were the most frequently identified pathogens, with a detection rate of 80%, followed by Candida species at 16.9%, consistent with the findings of Keyvan Kiakojuri et al. 11 Aspergillus infections often present with hyphae of varying colors, while Candida infections are characterized mainly by secretions, which may solidify and be misdiagnosed as cerumen impaction. It is important to note that in patients with water exposure in the ear canal or those using ear drops, Aspergillus infections may also present with discharge, further complicating the diagnosis. However, since most cases did not exhibit the classical signs of fungal infection—such as pruritus and visible hyphae—but rather symptoms like pain, discharge, and crusting, clinicians may easily misdiagnose the condition as bacterial otitis externa or even otitis media. Such misdiagnoses often lead to the inappropriate use of topical or systemic antibiotics, which not only delay correct antifungal treatment but may also exacerbate the infection. The high treatment failure rate of 56.3% observed in this study underscores the need for improved clinical awareness and diagnostic precision in managing otomycosis.
Traditionally, humid environments, cerumen accumulation, ear cleaning practices, immunosuppression, and overuse of topical medications have been considered potential risk factors for otomycosis.8,12 However, most of these associations are derived from observational studies and lack control groups for robust evidence from randomized controlled trials. Consequently, the risk factors for otomycosis remain a subject of ongoing debate in the academic community.
In the present study, individuals who engaged in habitual ear picking were found to have approximately 2.748 times the risk of developing otomycosis compared to those who did not. A substantial proportion (78.9%) of patients in the case group reported a habit of ear picking, which aligns with the findings of Jia et al. 13 This behavior commonly occurs after bathing. The skin of the external auditory canal functions as a physical barrier that protects against pathogenic invasion. Ear picking can disrupt the integrity of this barrier, thereby facilitating fungal entry. Indeed, trauma to the external auditory canal has been reported as one of the most frequent predisposing factors. 6 The external auditory canal also possesses a natural self-cleaning mechanism. Its secretions help maintain a mildly acidic environment that inhibits bacterial and fungal growth. Excessive cleaning may disrupt this balance, creating conditions favorable for fungal proliferation. 14 Our study found that both the case and control groups most commonly used ear scoops and cotton swabs as cleaning tools (Table 5). A minority reported using fingernails or towel fibers. However, the differences in tool usage between the 2 groups were not statistically significant. Nonetheless, if ear-picking tools are not properly sterilized—or if cotton swabs are left exposed after opening and become moldy—they may introduce fungal spores into the ear canal during use, potentially triggering otomycosis.
In several Asian countries such as China, Japan, and Vietnam, professional ear cleaning—or “ear-picking”—is a culturally ingrained practice often performed in barbershops or specialized salons. It is considered not only a method of hygiene but also a form of traditional healthcare and relaxation. Practitioners use a variety of specialized instruments, including ear scoops, ear picks, and feathered tools. However, this practice poses significant health risks. In addition to causing mechanical trauma to the ear canal and disrupting its natural defense mechanisms, inadequate sterilization procedures in many ear-picking establishments may facilitate cross-infection. In our study, the proportion of patients in the case group who had a history of professional ear cleaning was significantly higher than that in the control group. This practice emerged as a stronger independent risk factor than habitual self-cleaning. Individuals who underwent professional ear cleaning were found to have approximately 7.434 times the risk of developing otomycosis compared to those who did not. This finding is consistent with the study by Chen et al, 15 which also identified professional ear cleaning as a significant risk factor. These results highlight the urgent need for public education on safe ear hygiene practices and the formulation of hygiene regulations or guidelines by health authorities. It should be noted, however, that professional ear cleaning practices are strongly influenced by regional and cultural factors. In East Asian countries, including China, salon-based ear cleaning is a culturally embedded practice with considerable variability in hygiene standards, instrumentation, and sterilization procedures. Therefore, although salon ear cleaning showed the strongest statistical association in this study, residual confounding related to cultural practices and unmeasured environmental factors cannot be fully excluded. Caution is warranted when generalizing this finding to populations with different cultural habits.
Previous studies report that the average diameter of the adult external auditory canal is approximately 0.6 cm. 16 However, there is currently no standardized definition of canal stenosis. Some researchers consider a canal diameter of less than 4 mm as indicative of stenosis, 17 but in clinical practice, precise measurement is challenging. We employed a practical diagnostic criterion: if the tympanic membrane cannot be fully visualized using an otoscope in the absence of cerumen, subsequently, a 4-mm cotton swab was gently inserted to assess canal patency. Failure of the swab to pass through the isthmus of the external auditory canal was defined as canal stenosis. This study is the first to demonstrate that patients with external auditory canal stenosis have a significantly higher prevalence of otomycosis. The risk of developing otomycosis in individuals with canal stenosis was 3.737 times that of individuals without stenosis. A narrower canal increases the likelihood of cerumen impaction, 18 which may prompt more frequent ear cleaning and consequently cause microtrauma that facilitates fungal invasion. Moreover, a stenotic canal reduces ventilation, creating a moist and warm environment ideal for fungal proliferation. During infection, the narrowed canal may also hinder the delivery of topical medications, potentially compromising treatment efficacy.
It is often assumed that frequent use of earphones/hearing aids may impede air circulation or cause mechanical trauma to the ear canal, thereby increasing the risk of otomycosis. However, our findings did not support this hypothesis. The proportion of individuals who frequently used earphones or hearing aids was similar in both the case group (40%) and the control group (35%), showing no statistically significant difference. This result diverges from the perspective of Khasanov et al, 19 who regarded device use as a contributing risk factor. One possible explanation is that earphones and hearing aids are typically worn near the entrance of the ear canal, whereas fungal infections tend to occur in its deeper regions. As such, these devices may have limited impact on the microenvironment where otomycosis typically develops.
Although water entry into the external auditory canal during swimming can theoretically create a moist environment conducive to fungal growth, our study found no statistically significant difference in the proportion of individuals with a swimming habit (defined as swimming more than twice per week) between the case and control groups. This contrasts with the findings of Abdelazeem et al, 6 who reported that swimming (45%) was the second most common risk factor for otomycosis, following external auditory canal trauma (59%). This discrepancy may be attributed to differences in swimming frequency and duration. The definition of a swimming habit used in our study may not reflect sufficient exposure to significantly elevate the risk of infection. In contrast, professional swimmers or individuals who spend extended periods in the water may face a substantially higher risk. These results suggest that evaluating swimming as a risk factor for otomycosis requires a more nuanced approach, taking into account specific parameters such as frequency, duration, and water quality. Future research should explore the differential impact of varying levels of aquatic activity on the incidence of otomycosis.
Patients with diabetes are generally more susceptible to infections due to compromised immune function. However, our study did not find diabetes to be a significant risk factor for otomycosis in the general population. The prevalence of diabetes was identical in both the case and control groups (3.75%), aligning closely with the rate reported by Khurshid Anwar (5%). 20 Although Jia et al 13 and Khurshid Anwar 20 suggested that diabetes may be a potential risk factor for otomycosis, their findings did not show a significantly higher prevalence of diabetes in the case group compared to the general population. This may be attributed to the localized nature of otomycosis, which is more strongly influenced by local environmental and mechanical factors than by systemic conditions. Unlike invasive fungal infections that exploit systemic immunosuppression, otomycosis primarily involves superficial colonization and growth in the external auditory canal, where factors such as skin integrity, humidity, and local trauma play a more decisive role. Thus, in non-severe or community-based cases of otomycosis, diabetes alone may not significantly elevate infection risk. Although swimming and diabetes were not significantly associated with otomycosis in the present study, these findings should be interpreted cautiously. The number of participants with diabetes and frequent swimming habits was relatively small, which may have limited statistical power. Exploratory analyses did not suggest meaningful interaction effects; however, the study was not powered for formal interaction testing; however, their potential role in specific subgroups cannot be definitively excluded and warrants further investigation in larger, prospective studies.
This study has several limitations. First, its retrospective design may introduce recall bias, particularly for self-reported behavioral variables. Second, the control group consisted of individuals undergoing routine health examinations, who may differ from outpatient cases in socioeconomic status, health-related behaviors, and hygiene awareness, potentially leading to selection bias. Third, although multiple candidate variables were included in the multivariable regression model, unmeasured confounders—such as environmental humidity, detailed salon hygiene conditions, or frequency and intensity of exposures—could not be fully accounted for. Fourth, the single-center design may limit the generalizability of the findings. Future multicenter, prospective studies with more detailed exposure assessment are needed to further validate these results.
Conclusion
By comparing the case and control groups, this study identified key risk factors for otomycosis, including habitual ear picking, professional ear cleaning at salons, and external auditory canal stenosis. These findings offer important clinical guidance for the prevention and management of otomycosis and may contribute to reducing both incidence and recurrence rates.
Footnotes
Ethical Considerations
This study has been approved by the Ethic Committee of Zhongshan Hospital of Xiamen University (registered at ClinicalTrials.gov, Registration number: NCT06530069).
Consent to Participate
Written informed consent was obtained from all participants.
Author Contributions
Peng Liu: wrote the paper, conceived and designed the analysis, collected the data, recruitment of subjects. Chunsheng Ye: recruitment of subjects, substantial contributions to conception and design, or acquisition of data. Lili Zhuang: statistics, analysis and interpretation of data. Song Zou: involved in revising it critically for important intellectual content, recruitment of subjects.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.