
Abstract
Objective
The Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity (POSSUM) is commonly used to predict the risk of postoperative complications in general surgery. However, use of the POSSUM is not absolutely suitable for open pancreaticoduodenectomy (OPD), which has unique complications such as pancreatic fistula formation. This study was performed to establish a new risk score for assessing the incidence of postoperative complications of OPD.
Methods
This retrospective case-control study involved 159 patients who underwent standard OPD from 2 January 2017 to 1 February 2019. The risk factors for post-OPD complications were statistically investigated, and a risk score model was established by multivariate logistic regression.
Results
Among all 159 patients, 72 (42.28%) developed complications. A scoring system was developed based on the following five independent variables: sodium concentration of <141.20 mmol/L, white blood cell count of >6.35 × 109/L, pancreatic texture grade, body mass index of >25.06 kg/m2, and basic respiratory diseases. Our risk score model demonstrated better discriminating power, prediction power, and prediction probability than the POSSUM model in the receiver operating characteristic curve analysis.
Conclusion
This novel risk score may help to predict postoperative complications after OPD with higher accuracy than the POSSUM system.
Keywords
Introduction
Pancreatic cancer is one of the most malignant tumors of the digestive system. Although the prognosis has slightly improved in recent years, the 5-year survival rate is still less than 8%. According to the latest data of the American Cancer Association, pancreatic cancer is the fourth leading cause of death, and an estimated 22,919 men and 21,093 women were projected to die of pancreatic cancer in 2020. 1
With the progress of surgical conditions and postoperative care during the past decade, the mortality rate of Whipple’s surgery in major medical centers worldwide has dropped to less than 5%. However, the incidence of postoperative complications remains high. 2
Although the risk factors for complications following OPD have been identified,3,4 few studies have established a scoring system. Notably, considering the differences in race, lifestyle, and symptoms, the Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity (POSSUM) is not absolutely suitable for predicting the incidence of postoperative complications of OPD. This study was performed to establish a new risk scoring system with which to assess the incidence of postoperative complications of OPD in Shijiazhuang, Hebei Province, China and to provide a reference for doctors in other centers and patients in different regions and of different races and lifestyles to predict postoperative complications following OPD.
Methods
Ethics and informed consent
This study was based on the declaration of Helsinki. It was authorized by the Human Ethics and Research Ethics Committee of the Fourth Affiliated Hospital of Hebei Medical University, Shijiazhuang, Hebei, China (authorization date: 16 March 2019; approval no. 2019MEC066). We have de-identified all data such that the identity of the patients cannot be ascertained in any way. All enrolled patients provided written informed consent for treatment. This was a retrospective case-control study and complies with the STROBE principle in the EQUATOR Network guidelines. 5
Patient recruitment
A total of 159 patients underwent standard OPD from 2 January 2017 to 1 February 2019 for treatment of periampullary malignant carcinoma at the Fourth Affiliated Hospital of Hebei Medical University in Shijiazhuang City, China. No patients underwent preoperative biliary drainage, and all were treated with modified Blumgart anastomosis during pancreatic–intestinal anastomosis. The inclusion criteria were no preoperative biliary drainage and the performance of modified Blumgart anastomosis during pancreatic–intestinal anastomosis. The exclusion criteria were resection of other organs during the operation, intraoperative vascular resection and reconstruction, and an inability to tolerate surgery because of kidney disease. We continuously collected information on eligible patients according to the study’s inclusion and exclusion criteria.
Collection of perioperative parameters
In this retrospective case-control study, we collected a series of perioperative clinical and histopathological parameters. The patients’ American Society of Anesthesiologists classification, blood pressure, and pulse rate were measured before entering the operating room on the day of surgery. Cardiac function tests, an electrocardiogram, pulmonary function tests, and imaging examinations were performed on the day of admission. The blood test indicators were taken from the last preoperative laboratory test, which was performed within 3 days before the operation. The following laboratory parameters were measured: hemoglobin concentration, platelet count, potassium concentration, ejection fraction, pulse rate, forced expiratory volume in 1 s, white blood cell count, alanine aminotransferase concentration, prothrombin time, activated partial thromboplastin time, international normalized ratio of prothrombin time, albumin concentration, total bilirubin concentration, blood urea nitrogen concentration, serum creatinine concentration, sodium concentration, CA19-9 concentration, electrocardiogram parameters, and blood pressure. Essential clinical and background data were sex, drinking history, smoking history, history of abdominal surgery, diabetes, basic respiratory diseases, age, height, and weight. Several perioperative parameters were also recorded, including the duration of surgery, intraoperative blood loss, intraoperative blood transfusion volume, and pancreatic texture grade. A pancreatic texture resembling the texture of the lips was defined as grade 5, that resembling the texture of the tip of the nose was defined as grade 3, and that falling between the two textures was defined as grade 4. A pancreatic texture as hard as the forehead was defined as grade 1, and that falling between grades 1 and 3 was defined as grade 2. The diameters of the bile duct and pancreatic duct were recorded intraoperatively. Finally, the diameter and pathological grade of the tumor were recorded based on the histopathological reports.
Outcome measurement
Outcome measurement was carried out according to the Clavien–Dindo classification. 6 Clavien–Dindo grade ≥II complications were considered clinically significant. Complications after OPD included stress ulcers, pancreatic fistulas, gastrointestinal bleeding, pleural effusion, intra-abdominal infection and abscesses, pneumonia, arrhythmia, hemorrhage, acute renal failure, death, and delayed gastric emptying.
Statistical analysis
The Kolmogorov–Smirnov test was used to determine the normality of the data. Continuous variables with a normal distribution are expressed as mean ± standard deviation and were analyzed by Student’s t-test. Data with a non-normal distribution are expressed as median (interquartile range) and were analyzed by the Mann–Whitney U-test. Dichotomous variables were analyzed by Pearson’s chi-square test and are presented as percentages (Table 1). Spearman’s correlation test was used to further analyze the correlation between variables and postoperative complications (Table 2). Additionally, the tolerance and variance inflation factor (VIF) among the variables were calculated by multivariate linear regression, allowing us to determine the collinearity among the variables (Table 3). A VIF of >10 indicates a serious multiple collinear relationship between the independent variable x and other independent variables. As the tolerance approaches 1, the collinearity between independent variables weakens. We used univariate logistic regression, at the univariate stage, to further analyze the relationship between the variables and postoperative complications of OPD, and we calculated the odds ratio (OR) and 95% confidence interval (95% CI) of each risk factor. Univariate (Table 4) and multivariate (Table 5) logistic regression analyses (method: backward, conditional) were used to determine the risk factors for complications after OPD. In the process of the multivariate logistic regression with the backward method, the variables with a p value of >0.1 were removed. After performing the multivariate logistic regression 29 times, we obtained the “best” model. The risk score model was established based on the multiple regression coefficients. Each coefficient was divided by the minimum factor and rounded to the nearest integer.7,8 Summation of each predictor is used to predict the risk of complications after OPD. We applied the Hosmer–Lemeshow test to internally calibration the model. The area under the receiver operating characteristic curve (AUC) and its 95% CI were used to evaluate the reliability of the model and determine the threshold of each risk factor. We use the continuous net reclassification index (NRI) to compare the predictive power of our new risk scoring model with the existing risk scoring model (POSSUM scoring model). The AUC was also compared using the Z test. A p value of <0.05 (two-sided) was considered statistically significant.
Perioperative baseline data of patients who underwent open pancreaticoduodenectomy

Data are presented as n (%), mean ± standard deviation, or median (interquartile range).
*Statistically significant variables.
Pathological classification: 1 represents poorly differentiated malignant tumors, 2 represents moderately differentiated malignant tumors, and 3 represents well-differentiated malignant tumors.
ECG signs: level 1 represents normal ECG findings, level 2 represents abnormal ECG findings without clinical intervention, and level 3 represents abnormal ECG findings requiring clinical intervention.
Pancreatic texture grade: grade 5 indicates that the pancreatic texture is similar to that of the lips, grade 3 indicates that the pancreatic texture is similar to that of the tip of the nose, and grade 2 lies between grades 1 and 3. Grade 1 indicates that the pancreatic texture is as hard as the forehead, and grade 2 lies between grades 1 and 3.
BMI, body mass index; FEV1, forced expiratory volume in 1 second; ALT, alanine aminotransferase; PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio of prothrombin time; ECG, electrocardiogram; ASA, American Society of Anesthesiologists.
Spearman’s correlation test between perioperative baseline data and complications of open pancreaticoduodenectomy
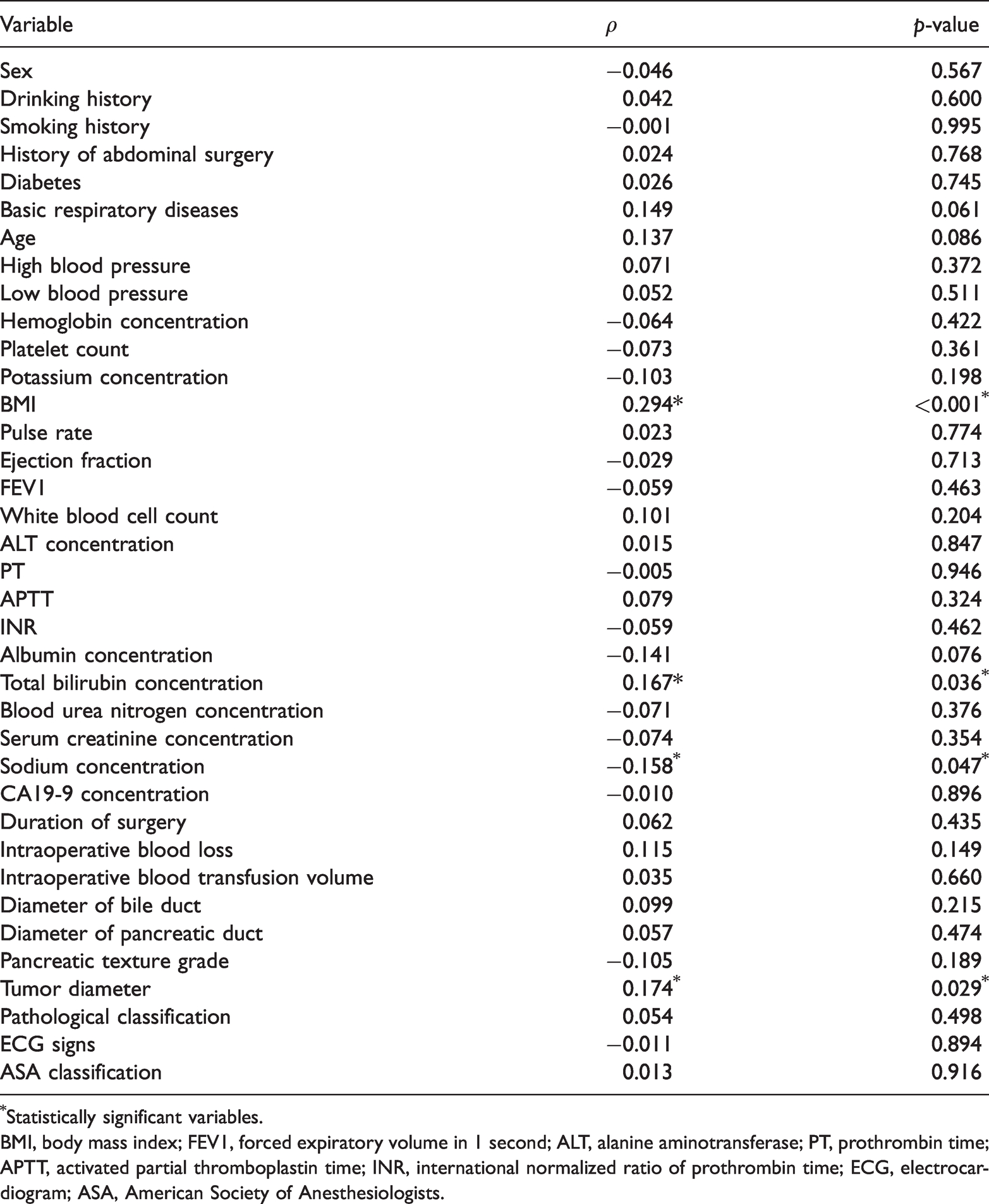
*Statistically significant variables.
BMI, body mass index; FEV1, forced expiratory volume in 1 second; ALT, alanine aminotransferase; PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio of prothrombin time; ECG, electrocardiogram; ASA, American Society of Anesthesiologists.
Collinearity of the relationship between patient variables and complications of open pancreaticoduodenectomy based on linear regression

VIF, variance inflation factor; BMI, body mass index; FEV1, forced expiratory volume in 1 second; ALT, alanine aminotransferase; PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio of prothrombin time; ECG, electrocardiogram; ASA, American Society of Anesthesiologists.
Correlation between patient variables and complications after open pancreaticoduodenectomy, based on univariate logistic regression

*Statistically significant variables.
BMI, body mass index; FEV1, forced expiratory volume in 1 second; ALT, alanine aminotransferase; PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio of prothrombin time; ECG, electrocardiogram; ASA, American Society of Anesthesiology.
Predictive model constructed by multivariate regression logistic regression (method: backward, conditional)

OR, odds ratio; CI, confidence interval; BMI, body mass index.
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 23.0 (IBM Corp., Armonk, NY, USA). A p-value of <0.05 was considered statistically significant.
Results
Baseline characteristics
The patients’ baseline characteristics are shown in Table 1. Of the 159 patients who underwent OPD, 72 (45.28%) patients developed Clavien–Dindo grade ≥II complications. The patients’ mean age was 59 ± 9.11 years (Table 1). The patients with complications had a higher body mass index (BMI) (p < 0.001), higher total bilirubin concentration (p = 0.036), larger tumor diameter (p = 0.029), and lower sodium concentration (p = 0.047) than patients without complications (Table 1).
Associations by Spearman’s correlation test
To confirm whether each variable plays a potential role in postoperative complications after OPD, Spearman’s correlation test was used for further correlation analysis. Spearman’s correlation coefficient indicated that the BMI (ρ = 0.294, p < 0.001), total bilirubin concentration (ρ = 0.167, p = 0.036), and tumor diameter (ρ = 0.174, p = 0.029) were positively correlated with postoperative complications, whereas the sodium concentration (ρ = −0.158, p = 0.047) was negatively correlated (Table 2).
Multivariate linear regression
We used multivariate linear regression analysis to diagnose the collinearity of each variable. A VIF of >10 indicates serious collinearity between the independent variable x and other independent variables. As the tolerance approaches 1, the collinearity between independent variables weakens. Table 3 shows that the VIF of each variable was <4, indicating no significant collinearity among the variables. All variables were suitable for inclusion in the process of model construction (Table 3).
Univariate logistic regression
The OR for a high BMI was 1.221 (95% CI, 1.093–1.364; p < 0.001) compared with a low BMI. A lower albumin concentration was associated with a higher risk of postoperative complications (OR, 0.885–0.999; 95% CI, 0.885–0.999; p = 0.047). Patients with a high total bilirubin concentration had a higher risk of postoperative complications than those with a low total bilirubin concentration (OR, 1.003; 95% CI, 1.0002–1.006; p = 0.038). The OR for postoperative complications in patients with a larger tumor diameter was 2.026 (95% CI, 1.073–3.826; p = 0.029) compared with a smaller tumor diameter. The other factors were not significantly associated with postoperative complications after OPD (Table 4).
Multivariate logistic regression and construction of predictive model
We applied multivariate logistic regression to analyze the data (Table 5). Eventually, after repeating the multivariate logistic regression 29 times, we constructed the “best” model. We identified five risk factors for complications after OPD and calculated their ORs and 95% CIs at the multi-factor level. Patients with a higher BMI had a higher risk of postoperative complications than those with a low BMI (OR, 1.346; 95% CI, 1.172–1.545; score of 3; p < 0.001). The OR for postoperative complications in patients with basic respiratory diseases was 3.780 (95% CI, 1.689–8.463; score of 12; p = 0.001). Patients with a higher white blood cell count also had a higher risk of complications (OR, 1.220; 95% CI, 1.004–1.482; score of 2; p = 0.045). The OR for complications in patients with a low sodium concentration was 1.121 (95% CI, 1.026–1.225; score of 1; p = 0.011). In patients with a soft pancreatic texture, the adjusted OR for complications was 1.305 (95% CI, 1.005–1.694; score of 2; p = 0.011). The Hosmer–Lemeshow test showed a p value of 0.124, which is greater than 0.05 and thus indicates that the variables included in the parsimonious model were sufficient; i.e., the explanatory power was not different from the saturated model.
Receiver operating characteristic curve
Our risk score model demonstrated better discriminating power than the POSSUM model in the receiver operating characteristic (ROC) curve analysis after the Z test (AUC, 0.787 vs. 0.553; 95% CI, 0.716–0.858 vs. 0.464–0.643; p < 0.001 vs. p = 0.247) (Figure 1). Compared with the POSSUM scoring system, the novel risk score had better prediction power (NRI = +39.9%, p < 0.05). In addition, we used integrated discrimination improvement to compare the difference in the prediction probabilities between the two models (new score vs. POSSUM score: IDI = +0.231, p < 0.05). Considering all these data, the predictive value of our model was significantly better than that of the POSSUM system. Finally, the ROC curve analysis indicated that when the patient’s score is >22.50, the probability of postoperative complications is >50%.

(a) ROC curve analysis of the ability of the new scoring system to predict complications after open pancreaticoduodenectomy. (b) ROC curve analysis of the ability of the POSSUM scoring system to predict complications after open pancreaticoduodenectomy. ROC, receiver operating characteristic; AUC, area under the curve; CI, confidence interval.
Discussion
To the best of our knowledge, pancreaticoduodenectomy is still the most effective treatment method to prolong the survival time of patients with pancreatic head cancer, lower bile duct cancer, ampullary cancer, and other periampullary malignancies. 9 However, the incidence of complications after pancreaticoduodenectomy is still higher than 45%,10,11 which seriously affects patients’ prognosis, prolongs the hospital stay, increases the cost of hospitalization, and causes postoperative systemic inflammation, multiple organ failure, and even death.9,10 Although the risk factors for complications after OPD have been confirmed by many studies, few studies have constructed a scoring system to predict the occurrence of complications after OPD. Therefore, it is necessary to establish effective postoperative complication risk stratification tools for patients undergoing OPD.
Based on the discovery of high-risk factors, after further model construction, we have established a new scoring system to predict postoperative complications after OPD. This model can predict postoperative complications after OPD sensitively and accurately; importantly, it is more effective than the POSSUM scoring system.
The POSSUM scoring system is a recognized scoring system used to predict postoperative complications of general surgery. After our ROC analysis, however, the AUC of the POSSUM system was significantly lower than that of our new scoring system. In addition, the new scoring system had a higher NRI and IDI. This shows that the ability of the new scoring system to predict post-OPD complications is significantly higher than that of the POSSUM system.
In this study, 72 (45.28%) patients developed Clavien–Dindo grade ≥II complications, which is consistent with some previous studies. At the single-factor level, our research results allow us to make the following conclusions. In the correlation analysis and logistic regression analysis, the incidence of complications after OPD was significantly associated with a high BMI, lower albumin concentration, high total bilirubin concentration, and larger tumor diameter. More importantly, at the multi-factor level, a higher BMI, basic respiratory diseases, a higher white blood cell count, a low sodium concentration, and a soft pancreatic texture were considered to be high-risk factors for complications after OPD.
Previous studies have proven that patients with a high BMI have a higher risk of complications after pancreaticoduodenectomy.12–14 Mungroop et al. 13 retrospectively analyzed 1924 cases and found that a high BMI was a high-risk factor for postoperative pancreatic fistula (per 1-kg/m2 increase: OR, 1.07; 95% CI, 1.04–1.11). Hu et al. 14 obtained similar results; they analyzed 539 successive cases of pancreaticoduodenectomy and found a significant correlation between postoperative pancreatic fistula and BMI (≤25 vs. >25 kg/m2: 46.94% vs. 57.82%, respectively; p = 0.024). We consider that the three main reasons for these findings are as follows: first, the higher abdominal fat and peripancreatic fat content increases the difficulty of exposing the pancreas during surgery; second, the fat-rich pancreas is soft and fragile, increasing the risk of damaging the pancreas during surgery; and third, during pancreatic jejunostomy, sutures and knotting are more likely to damage the fatty pancreatic tissue and pancreatic duct, leading to a higher risk of pancreatic fistula.
With regard to a higher white blood cell count as a risk factor, Aasvang et al. 15 found that after pancreaticoduodenectomy, the neutrophil–lymphocyte ratio was more closely related to surgical complications than Clavien–Dindo grade III complications and postoperative pneumonia. Aizenshtein et al. 16 found that the preoperative white blood cell count was related to the length of hospitalization (B = 0.392, p < 0.01). A preoperative white blood cell count of >8150/μL can predict a longer hospitalization time (Z = 2.090, p = 0.03). We consider that this can be explained as follows. To some extent, the preoperative white blood cell count reflects the severity of inflammation around the patient’s preoperative lesion. Surgical damage amplifies the inflammation around the lesion, especially around the anastomosis. Inflammation affects the healing of the anastomosis,17,18 increasing the risk of bile duct jejunostomy fistulas, pancreatic jejunostomy fistulas, and gastrointestinal anastomotic fistulas.
With respect to the sodium concentration, an observational study by Chen et al. 19 showed that a low sodium concentration was an independent risk factor for postoperative complications based on the logistic regression analysis. In surgical operations other than OPD, an abnormal sodium concentration also indicates a higher risk of postoperative complications.20–22
Finally, we examined the pancreatic texture in terms of its association with the risk of complications after OPD. Many previous studies have shown that a harder pancreatic texture predicts a lower risk of complications after OPD.23–25 In addition, a prospective randomized controlled study by Bassi et al. 26 showed that the incidence of pancreatic fistula formation in a fibrotic pancreas was low.
Through verification using the ROC curve, we found that the new scoring system in our study (AUC = 0.787; p < 0.001; 95% CI, 0.716–0.858) is more effective than the traditional POSSUM scoring system (AUC = 0.553; p = 0.247; 95% CI, 0.464–0.643). Specifically, our new scoring system can more accurately predict postoperative complications after OPD than the traditional POSSUM scoring system. The POSSUM is based on the perioperative data of all surgical patients, comprehensively predicting the incidence and mortality of postoperative complications. This score can be applied to various types of surgery, but it is difficult to apply to a specific surgery. The new scoring system established in our study provides a more suitable tool for predicting postoperative complications in patients undergoing OPD by collecting the perioperative data of patients specifically undergoing OPD. Our risk score shows that the predictive ability of our scoring system for postoperative complications after OPD is better than that of the POSSUM system (NRI = +39.9%, p < 0.05; IDI = +0.231, p < 0.05). After the Z test, the AUC of our score was significantly higher than that of the POSSUM (AUC = 0.787 vs. 0.553; 95% CI, 0.716–0.858 vs. 0.464–0.643; p < 0.001 vs. p = 0.247) (Figure 1). This indicates that our new scoring system is significantly more effective than the POSSUM in predicting complications after OPD. In addition, McMillan et al. 27 reported that the ACS-NSQIP score used to predict postoperative complications after pancreaticoduodenectomy has a C-statistic of <0.61. This is significantly lower than the C-statistic of our model (0.787), indicating that our model may also be more effective than the ACS-NSQIP model. Moreover, our model includes fewer variables, is more convenient to calculate, and may provide more realistic results.
This study has several limitations. The first limitation is the research design. This was a retrospective study, not a prospective randomized controlled study, and therefore has some inherent drawbacks. The second limitation is that the data in this study were obtained from a single institution. Thus, there many have been some inconsistencies in the patients’ preoperative treatment, such as surgical methods or placement of drainage tubes. Finally, there are many potential predictors of complications after OPD that have not yet been identified. Many such factors were not included in the study. Our research team plans to continue to identify risk factors and continuously improve our model in future. Because this study has several potential limitations and its results have not been confirmed, our results should be verified and improved in multi-institutional, prospective, randomized controlled trials.
Conclusion
We have developed a novel risk scoring system to help predict postoperative complications after OPD. This scoring system may have higher accuracy than the POSSUM scoring system.
Footnotes
Acknowledgements
We thank Dr. Peng for his important role in the data collection. We also thank Dr. Zhang for his valuable comments on this article. Finally, we thank Drs. Wang and Li for their support.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
Lian Chen performed the statistical calculations using the clinical data. Li Peng collected the clinical data. Meng Zhang guided this research.
Consent for publication
All authors agree to the publication of this manuscript.
Availability of data and material
All data and material were obtained from the clinical treatment process. To protect the patients’ privacy, we are unable to share the patient-related data.