
Abstract
Introduction:
Anterior tympanic membrane (TM) defects present a surgical challenge due to the lack of support for the graft, resulting in reduced success rates. Established anchoring tympanoplasty (EAT) techniques usually aim to anchor the graft to the anterior rim of the TM. The “cartilaginous bending spring tympanoplasty” (CBST) secures the graft to the TM by supporting it with a U-shaped bending spring cartilage placed underneath in the middle ear. Initial experimental studies have already shown the feasibility of CBST without impeding sound transmission. This prospective clinical study evaluates the outcome of CBST compared to EAT in terms of closure of TM defects and hearing outcome.
Materials and Methods:
This randomized controlled study was conducted at a tertiary referral center from March 22, 2018 to September 17, 2020. Patients were randomized to surgeon and reconstruction technique (EAT vs CBST). Inclusion criteria were chronic otitis media with TM defects that involved at least the anterior part of the TM, subtotal defects, and an intact ossicular chain. Primary objectives were the successful reconstruction of the TM and the hearing outcome.
Results:
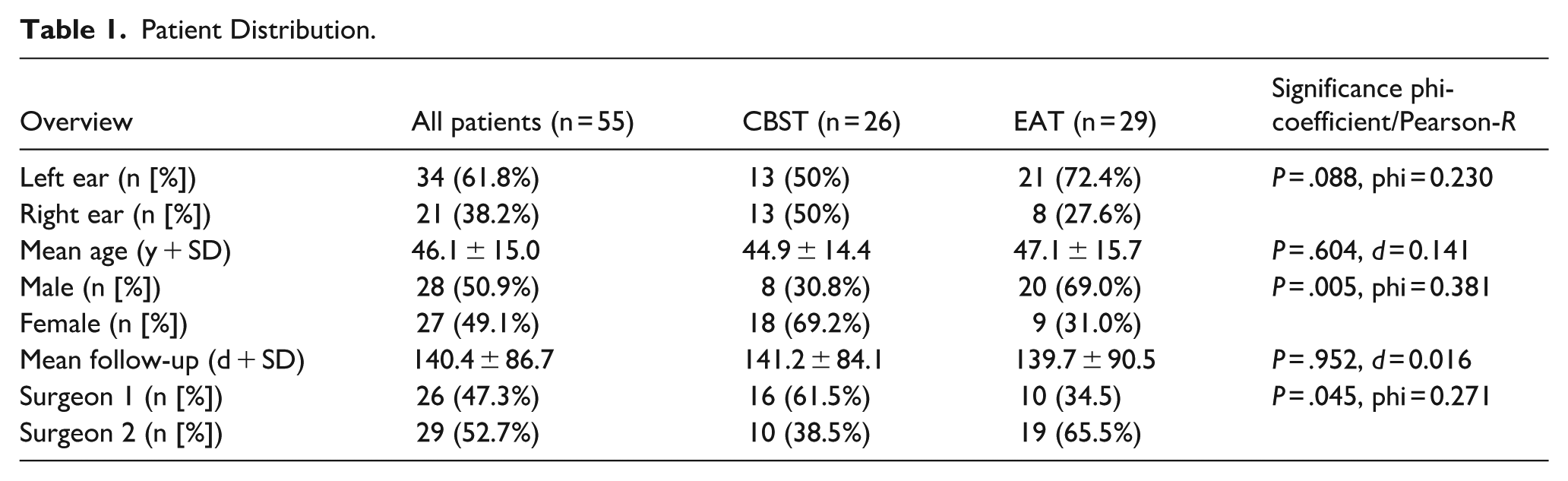
Fifty-five patients (55 ears; CBST n = 26, right ears = 13; EAT n = 28, right ears = 8) with a mean age of 46.1 ± 15.0 years and a mean follow-up of 140.4 ± 86.7 days were included. The TM was successfully reconstructed in 95% of cases in both groups. Hearing improvement was comparable for both groups (improvement of air-bone gap: EAT: 3.0 ± 9.3 dB; CBST: 5.5 ± 6.2 dB; P = .244; Cohen’s d = 0.318).
Conclusion:
CBST allows for comparably high success rates of reconstruction of anterior TM defects and the hearing outcome. Accordingly, the U-spring bending cartilage supporting the graft does not adversely affect hearing outcome. Thus, CBST can be considered a useful technique to close anterior defects of the TM effectively.
Introduction
Since the 1950s and the description of surgical techniques by Wullstein and Zollner,1,2 chronic otitis media mesotympanalis has been treated by tympanoplasty, aiming to reconstruct the tympanic membrane (TM) and restore hearing. Thus, successful surgical closure results in an improvement in quality of life and social participation.3,4 While defects of the posterior quadrants of the TM have had high surgical success rates of 90%,5 -7 anterior defects are surgically challenging. This is due to difficult and therefore inadequate visualization, little residual membrane, and the lack of support for the graft. This leads to a big variation in closure rates, ranging from 67% to 94%.8,9 Established reconstruction techniques, such as the anterior pull-through tympanoplasty 10 techniques, anchor the graft to the anterior rim of the TM. However, over time, medialization of the graft may occur, which reduces the hearing outcome.
Recently, the technique of the cartilaginous bending spring tympanoplasty (CBST) was described by Mantsopoulos et al 11 with the aim of preventing graft medialization. However, it was suspected that the performed additional non-physiological support of the TM would compromise sound transmission. An experimental study by Rupp et al alongside the first clinical results, proved that CBST did not cause any clinically meaningful sound reduction. 12
Consequently, this prospective controlled randomized clinical study evaluates the clinical outcome with regard to closure of the TM and postoperative hearing of CBST compared to established reconstruction techniques and is the first study to evaluate CBST in a bigger clinical setting.
Primary objectives were defined as the rates of intact TM at follow-up and the improvement of the air-bone gap (ABG). Secondary objectives were the evaluation of surgery time.
Materials and Methods
Study Description
This prospective randomized study was performed at a tertiary hospital and academic cancer center (Department of Otolaryngology – Head and Neck Surgery, Friedrich-Alexander University of Erlangen-Nuremberg, Erlangen, Germany) from March 22, 2018 to September 17, 2020.
This clinical study was conducted according to the Declaration of Helsinki, approved by the Ethics Committee of the University of Erlangen-Nuremberg (application number: 51_18B), and registered in the German Clinical Trials Register (application number: DRKS00014863 – https://drks.de/search/de/trial/DRKS00014863). Each patient gave written informed consent.
The sample size for this study was determined by including all patients who underwent surgical intervention for TM defects during the predefined study period. No prior sample size calculation was performed, as the study aimed to capture the entire population of eligible cases within the specified timeframe. This approach ensures that the data reflect real-world clinical practice during the study period, minimizes selection bias, and maximizes the representativeness of the findings.
Patient randomization was conducted by a member of the investigation group who was not involved in performing surgical procedures or collecting audiometric measurements. A permuted block randomization sequence (blocks of 4) was generated using the random.org online true random number service (integer sets) to ensure balanced group allocation. Patients were assigned to CBST if the corresponding integer was odd and to EAT if the integer was even. The randomizing investigator, who possessed no knowledge of patient details beyond the scheduled surgery, informed the surgeon of the group allocation immediately prior to the procedure. The audiometrists responsible for outcome measurements remained blinded to group assignments throughout the study.
Inclusion criteria were as follows: chronic otitis media mesotympanalis with a TM defect that involved the anterior part of the TM, including subtotal defects, defined as involvement of more than 50% of the pars tensa of the TM, an intact ossicular chain, initial or revision surgery initially operated elsewhere, age ≥18 years, complete medical record. The following exclusion criteria applied: diagnosis of cholesteatoma, implantation of an ossicular replacement prosthesis, former tympanoplasty in our department, and follow-up <30 days.
Hearing outcome is presented by the thresholds of bone condition and air condition using the 4 frequency pure-tone audiometry (0.5-1-2-3 kHz), the respective 4 frequency pure-tone ABG and by speech audiometry using the Freiburg monosyllabic speech test at a presentation level of 65 dB sound pressure level for the word recognition score (WRS). The condition of the TM at the last follow-up was evaluated and used for the closure rate of the TM. A successful reconstruction of the eardrum was defined as the complete reconstruction of the eardrum after dressing removal.
Surgical Procedures
All patients were operated under general anesthesia by 2 senior surgeons (J.H. and A.-O.G.) with either a postauricular or an endaural approach using a microscope. A detailed description of the performed CBST was published by Mantsopoulos et al. 11 In short, after elevation of the remnants of the TM, a cartilage graft and a perichondrium graft are placed in an underlay fashion to reconstruct the TM. Another piece of cartilage is thinned and trimmed to a rectangle of ~6 mm in length, 2 mm in breadth, and 0.1 mm in thickness using a cartilage knife and scalpel. This rectangular piece, which does not vary depending on the size of the perforation, is placed between the reconstructed TM and the medial tympanic wall in the hypotympanon, making sure there is no contact with the bony surrounding of the tympanic cavity to ensure elasticity and uninhibited vibration (see Figure 1).
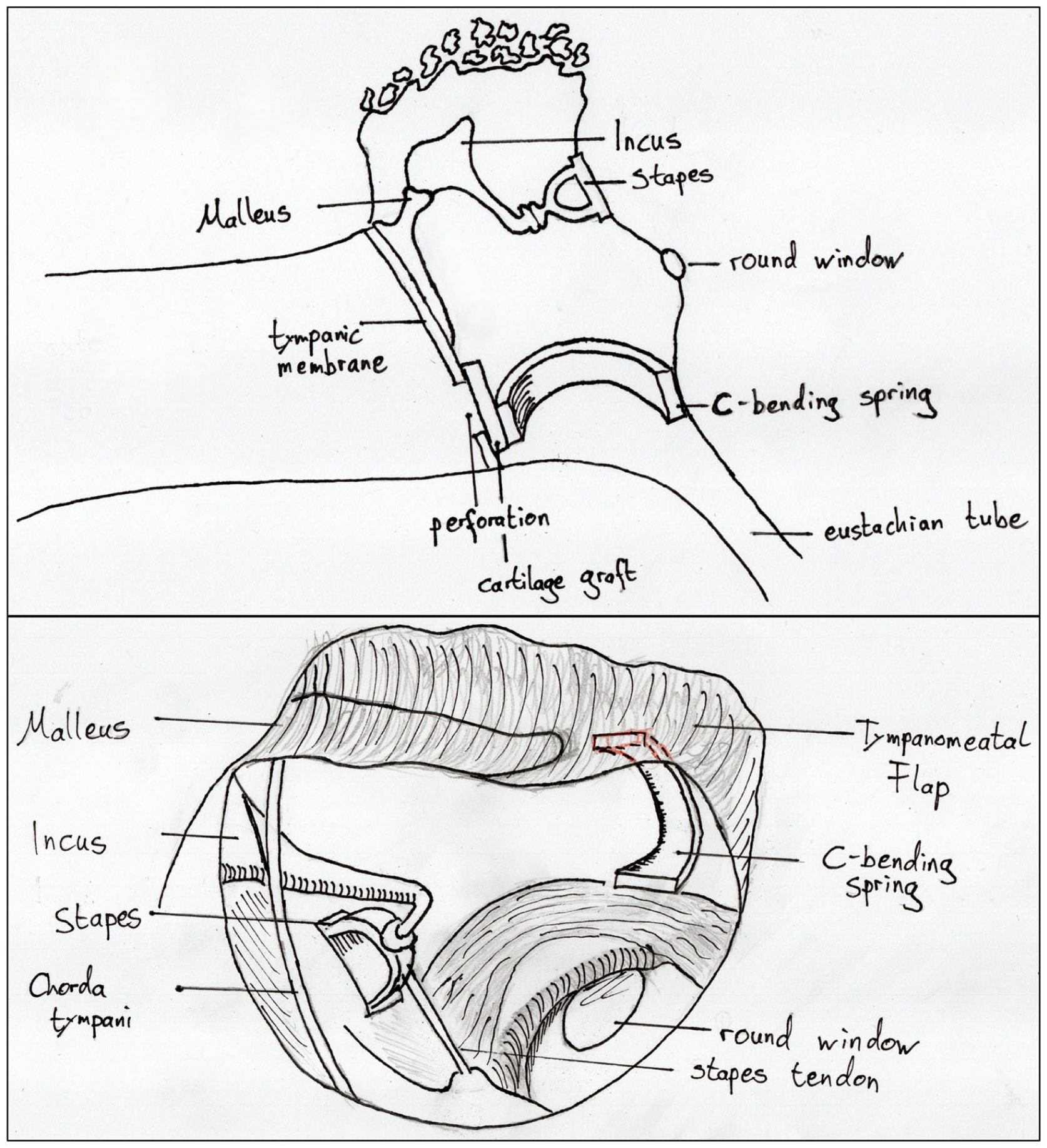
Schematic drawing of the surgical placement of the spring (top: side view and bottom: surgical view).
Besides CBST, reconstructions of the TM were performed according to the anchoring technique as described by Hung et al 13 and the anterior pull-through tympanoplasty as described by Harris et al. 10 The decision to use either of these 2 techniques was left at the surgeon’s discretion. In the following, we refer to both techniques as “established anchoring tympanoplasty” (EAT).
Statistical Analysis
Statistical analysis was performed using SPSS (IBM SPSS Statistics 29; IBM, New York, NY, USA). Normal distribution was assessed by performing the Kolmogorov-Smirnov test and assessing each variable’s histogram and Q-Q plot. Metric variables are presented as mean ± standard deviation in case of normal distribution, or additionally as median (25th and 75th percentiles) in case normal distribution was not given or data were ordinal scaled. Accordingly, independent and dependent t-tests were performed to evaluate hearing improvement after surgery in the case of normal distribution. In case variables were not normally distributed or ordinal scaled – the Wilcoxon or the Mann-Whitney U test was performed. For t-tests, Cohen’s d is presented as an effect size with 0.2 equaling a small, 0.5 a moderate, and 0.8 a strong effect. For the Mann-Whitney U and the Wilcoxon test, the effect size r is presented with 0.1 equaling a small, 0.3 a moderate, and 0.5 a strong effect.
Nominal scaled variables are reported as absolute and relative frequencies (n [%]), and groups were compared via cross-tables and the χ2 test. Phi is reported as an effect size, with 0.1 equaling a small, 0.3 a moderate, and 0.5 a strong effect.
Results
Tympanoplasty was indicated in 750 patients during the study period. Five hundred and eighty-three patients did not meet the inclusion criteria, and the remainder (167 patients) were randomized to either group. Intraoperatively, 94 patients (56%) were excluded from the study due to cholesteatoma or ossicular chain damage. Eighteen (33%) out of 57 of the remaining patients did not return for 30-day follow-up. These patients were excluded from the study. The analysis revealed 2 patients in the CBST group who experienced postoperative sensorineural hearing loss due to inner ear infection. These patients were also excluded from the study (Table 1 and Figure 2).
Patient Distribution.
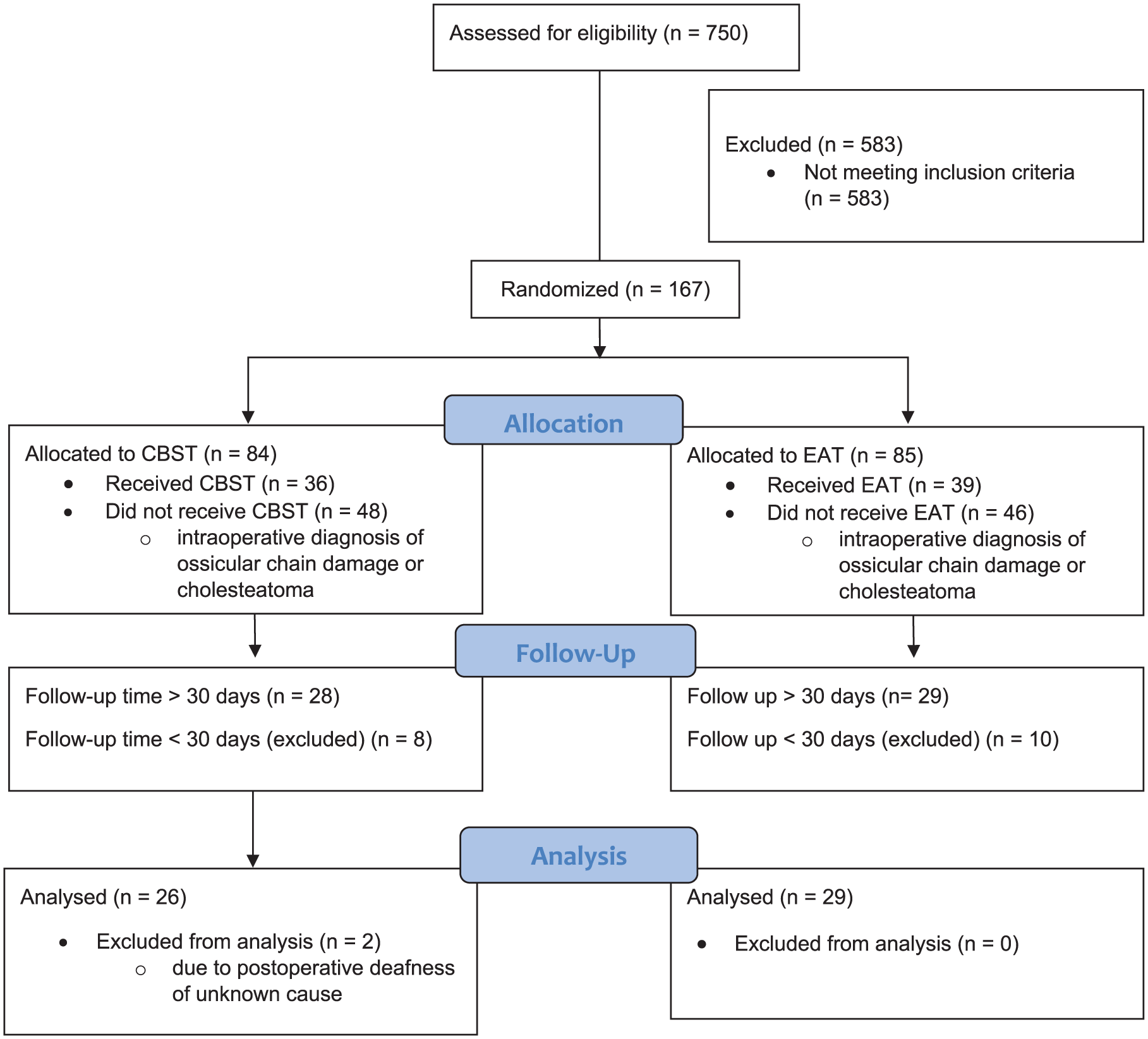
Consort flow diagram.
Within both groups, 95% of the reconstructed TM were closed at last follow-up (EAT: 27 out of 29; CBST: 26 out of 28; P = .488). The causes for failure were proinflammatory meatal fibrosis (n = 1) and reperforation (n = 1) within the EAT group. Regarding reperforation, no predisposing factors are known in the patient’s history. Dislocation of the graft (n = 1) and necrosis of the long process of the incus (n = 1) led to failure in the CBST group.
The EAT group presented a preoperative hearing threshold of 37.6 ± 18.6 dB, which did not change significantly postoperatively (38.5 ± 21.3 dB, P = .380, Cohen’s d = .057). Within the CBST group, the initial hearing threshold was 35.4 ± 11.70 dB before and 30.4 ± 13.3 dB (P = .028, Cohen’s d = 0.458) after surgery (Figures 3 and 4).
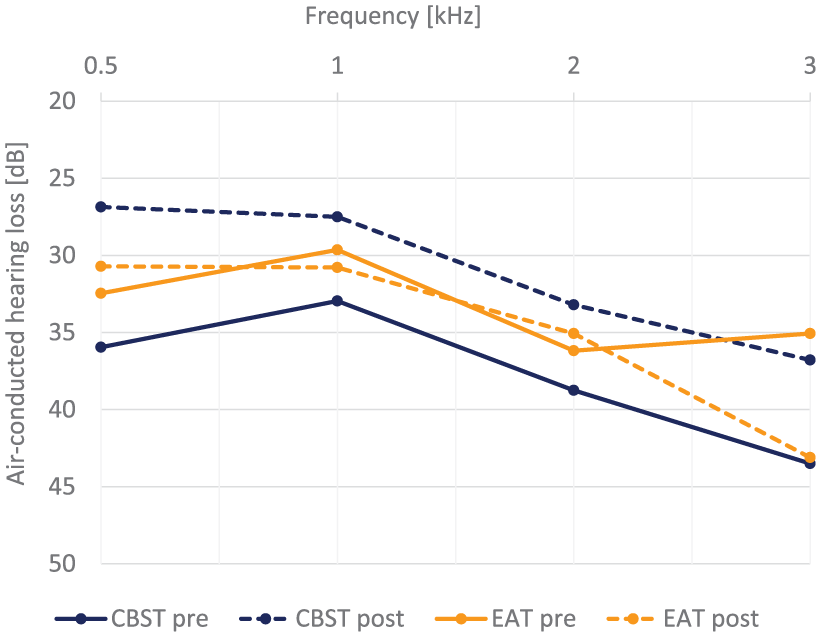
Pre- and postoperative levels of air-conducted hearing loss.
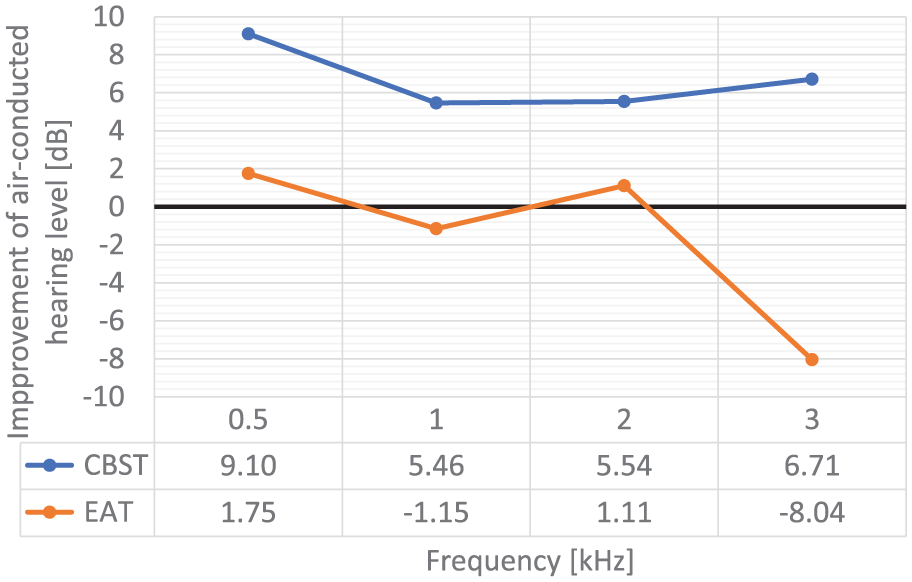
Improvement of air-conducted hearing loss.
The absolute changes of the hearing thresholds showed no significant difference between both groups (CBST: 5.04 ± 11.0 dB vs EAT: 0.9 ± 16.3 dB, P = .129, Cohen’s d = 0.417).
The ABG within the EAT group before and after surgery was 16.2 ± 8.4 and 13.4 ± 9.6 dB, respectively (P = .100, Cohen’s d = 0.316). For the CBST group, the respective values are 17.8 ± 7.0 and 12.0 ± 6.0 dB (P < .001, Cohen’s d = 0.913). The absolute change of the ABG was not significantly different between both groups (EAT: 3.0 ± 9.3 dB vs CBST: 5.5 ± 6.2 dB, P = .244, Cohen’s d = 0.318; Figure 5).
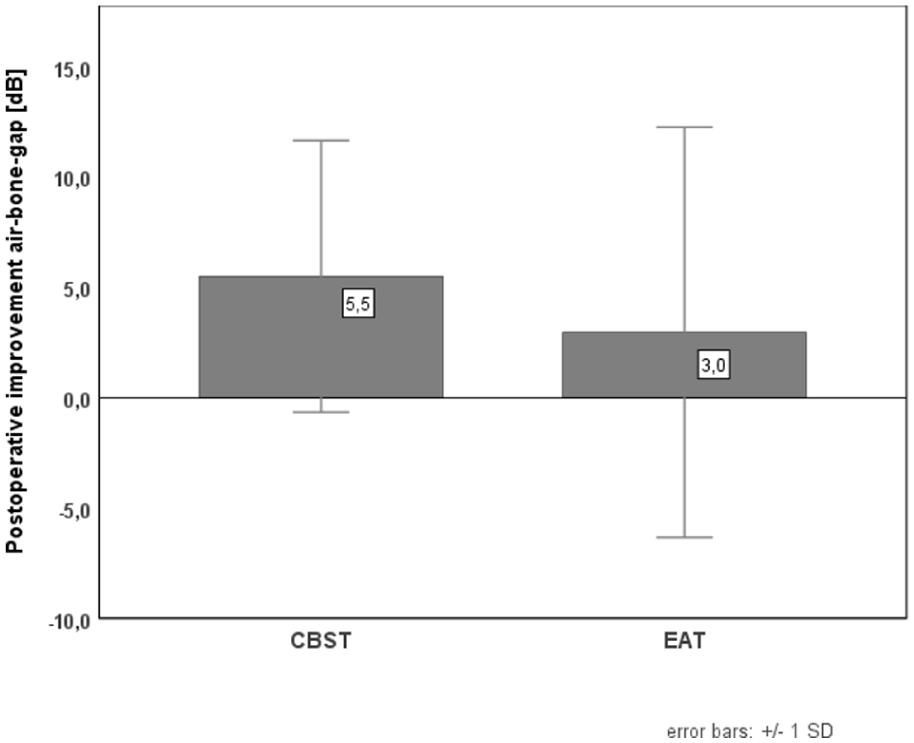
Improvement of the air-bone gap in 4-tone audiometry, separated by the reconstructive method after surgery.
The initial WRS in the EAT group on average was 62.1% ± 37.0 (Md: 75.00% [32.5-90.0]) and 57.1% ± 35.2 (Md: 55.00% [30.0-90.0]) after surgery (P = .254, r = 0.150). In the CBST group, the initial WRS was 63.1% ± 31.7 (Md: 77.5% [38.8-85.0]) and 73.7% ± 28.5 (Md: 77.5% [65.0-100.0]) after surgery (P = .061, r = 0.260). Changes in WRS (%) were significantly higher in the CBST compared to the EAT group (CBST: 10.6% ± 30.4; Md: 10.0% [−6.3 to 25.0]) vs EAT: −5.0% ± 27.7; Md: 0.0% [−17.5 to 10.0], P = .036, r = 0.282; Figure 6).
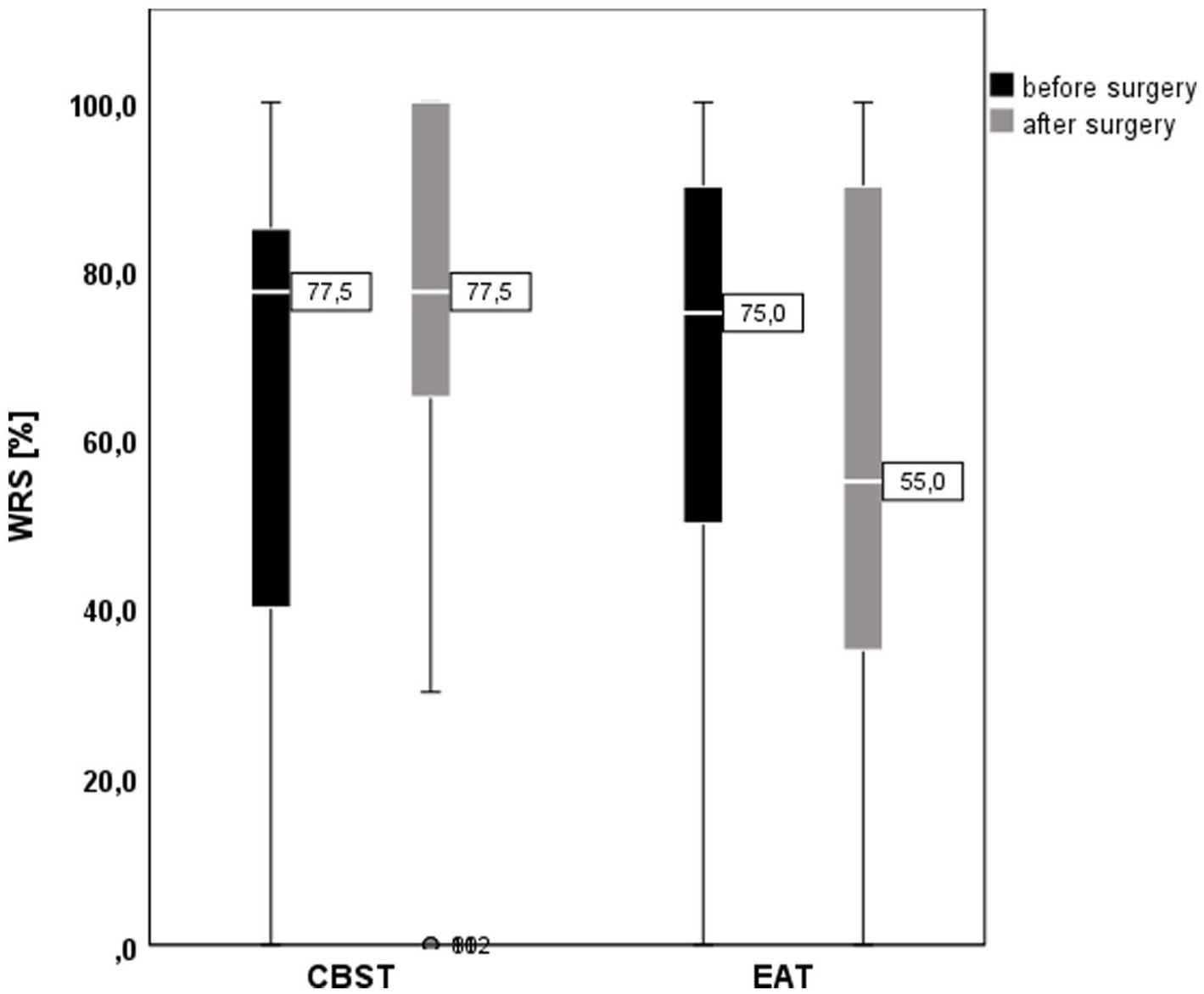
Word recognition score in the Freiburger monosyllabic speech audiometry, separated by reconstructive method.
The mean operation time for EAT was 79.7 ± 24.8 minutes compared to 71.4 ± 19.8 minutes for the CBST (P = .191, Cohen’s d = 0.368).
Discussion
This study shows that the technique of CBST is effective in terms of TM closure and hearing improvement. Improvement of hearing threshold and ABG in tone audiometry, as well as the duration of surgery, do not differ significantly compared to EAT.
Out of the 23 known tympanoplasty techniques, Tos proposed a classification into 6 groups in 2008. 14 According to this classification, CBST and the established techniques used here belong to the group of underlay techniques, in which a graft is placed under the remaining TM. However, the unique characteristic of CBST is that the underlay graft is supported by the spring cartilage.
The closure rate of 95% achieved with CBST lies in the upper reference range (67%-98.8%). More recent studies show success in a comparable range.12,15 However, comparison of reported results is challenging because the position of the perforation is often not specified more precisely than “central.” Harris et al, 10 a research group that exclusively operated on anterior defects, achieved a closure rate of 84.6% in 2016 in only 13 patients.
Muyshondt and Dirckx describe in their finite element model of the middle ear of the rabbit that even a small prestress on the TM significantly affects the response of the footplate through an effect called prestress stiffening. 16 In addition, Tonndorf and Khanna, in their study of the mechanical properties of the TM using time-averaged holography, have already shown that larger movements typically occur in the area between the manubrium and the annulus, that is, the area of mechanical stabilization by the cartilage spring. 17 Of note, this study used cadaveric TMs. However, both models are based on an intact TM, which was not present in any of our patients. If the natural state of the TM is already severely altered by a perforation, no detrimental effect of the insertion of the C-spring on the mechanical properties of the TM can be observed in this study and in the experimental study by Rupp et al. 12
Funnel et al reported that material loss and alteration lead to a decrease in TM mobility in the finite element model of the cat eardrum. 18 Still, CBST proved to be a feasible and effective reconstruction method in experimental and clinical evaluation.
Limitations and Strength
Several limitations of this study have to be addressed. First, the presented results derive from a relatively short follow-up time. Consequently, no statement can be made regarding long-term hearing outcome and closure rates of CBST. In this regard, the potential obstruction of the airway to the eustachian tube or late graft failure by the spring cartilage may be of special interest in the long term. Second, within the EAT group, deterioration of 30% and more occurred in a total of 5 out of 30 patients, resulting in a meaningful reduction in syllable comprehension. Another limitation of this study is the absence of a predefined sample size calculation, which may affect the interpretation of the results, such as the comparison of ABG improvement between groups. As the study aimed to include all eligible cases within a predefined timeframe rather than achieving a predetermined statistical sample size, it is possible that the study found significant differences that are clinically irrelevant. Lastly, this study was conducted at a single tertiary referral center with 2 experienced surgeons, which may limit the generalizability of the findings.
The strengths of this study were the prospective design with randomization regarding not only the reconstruction technique but also the surgeon. The single-center design prevented non-interpretable results due to different equipment and users. In the future, additional refinements of the proposed surgical technique, that is, variations of the dimension of the grafts used so far, may add to a further improved performance of CBST.
Conclusion
Reconstruction of TM defects affecting the anterior TM and hearing outcomes using CBST is similarly successful compared to EAT. This study excludes any clinically meaningful detrimental effect on hearing because of the bending cartilaginous support of the graft, as known from experimental data on CBST. It can, therefore, be included in the arsenal of tympanoplasty techniques for anterior and subtotal TM perforations.
Footnotes
Ethical Considerations
The study was conducted according to the tenets of the Declaration of Helsinki. To ensure patient privacy and well-being, data processing was performed in accordance with applicable data protection laws and ethical guidelines.
Consent to Participate
All study participants gave written informed consent.
Author Contributions
Substantial contributions: all authors made significant contributions. Concept: Olaf Conrad, Robin Rupp, Antoniu-Oreste Gostian; design: Sarina Müller, Joachim Hornung, Michael Koch; acquisition: Moritz Allner, Matti Sievert, Robin Rupp; analysis: Elisabeth Wimmer, Olaf Conrad, Alexander Heigl; interpretation: Olaf Conrad, Robin Rupp. Antoniu-Oreste Gostian. Critical drafting: all authors drafted the manuscript or critically revised it for important intellectual content. Draft: Olaf Conrad, Robin Rupp, Moritz Allner, Matti Sievert, Elisabeth Wimmer, Alexander Heigl; revision: Olaf Conrad, Robin Rupp, Antoniu-Oreste Gostian, Michael Koch, Sarina Müller, Michael Koch, Joachim Hornung. Final approval: all authors approved the final version of the manuscript for publication. Accountability: all authors agreed to be accountable for all aspects of the work and resolved any questions about its accuracy or integrity.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.