
Abstract
A man in his late 60s, with a history of psoriatic arthritis, presented with a 10-year history of hoarseness and exertional dyspnea. Flexible laryngostroboscopy demonstrated bilateral true vocal cord immobility resting in paramedian positions with glottic airway space reduction at ~5 to 10 mm on respiration. A contrast-enhanced computed tomography scan of the neck was performed to assess for a lesion along the course of the recurrent laryngeal nerves (RLNs), and it confirmed the findings of vocal cord immobility, evidenced by enlarged pyriform sinus and laryngeal ventricle, medialization and thickening of the aryepiglottic folds, and anteromedial deviation of the arytenoid cartilage, but no lesions along the RLNs. In the absence of structural, neurologic, or malignant causes, the findings were suggestive of cricoarytenoid joint fixation secondary to psoriatic arthritis. While cricoarytenoid arthritis is associated with other rheumatologic conditions, its association with psoriatic arthritis is exceedingly rare, with only 1 previously documented case. Our case highlights the importance of considering psoriatic arthritis in the workup of bilateral vocal cord immobility, particularly in patients with no other identifiable cause.
Introduction
Vocal cord immobility is characterized by impaired mobility of the true vocal cord(s), secondary to neurologic dysfunction or mechanical fixation. Bilateral vocal cord immobility involves impaired mobility of both true vocal cords and accounts for ~10% to 30% of cases. 1 Patients with bilateral vocal fold immobility present with symptoms including changes in voice, dysphagia, throat discomfort, dyspnea, cough, and aspiration. 2 The most common etiology of both unilateral and bilateral vocal fold immobility is surgical iatrogenic injury, with thyroid and parathyroid surgeries resulting in the majority of cases. Other common causes include neoplastic compression, central neurologic pathology, and idiopathic neuropathies. 1 In this report, we present a unique case of bilateral vocal fold immobility secondary to psoriatic arthritis.
Case Report
A Caucasian man in his late 60s was seen in the ENT clinic with a stable 10-year history of hoarseness and exertional dyspnea. His medical history was significant for psoriatic arthritis with no systemic treatment, as well as chronic pancreatitis and hypercholesterolemia. He had no surgical history. Flexible laryngostroboscopy demonstrated bilateral true vocal cord immobility resting in paramedian positions with glottic airway space reduction at ~5 to 10 mm on respiration. Fibrous tissue at the posterior glottis was also noted (see Figure 1). On phonation, the patient achieved some glottic voicing with some concurrent false vocal fold phonation (plica ventricularis). A contrast-enhanced computed tomography (CE-CT) scan of the neck was performed to assess for a lesion along the course of the recurrent laryngeal nerves (RLNs). CE-CT findings were consistent with vocal cord immobility, demonstrating an enlarged pyriform sinus and laryngeal ventricle, medialization and thickening of the aryepiglottic folds, and anteromedial deviation of the arytenoid cartilage. There was an accompanying fusion of the cricoarytenoid joints bilaterally. There was no evidence of any lesion along the pathway of the RLNs, and no evidence of malignancy or thyroid pathology (see Figure 2).
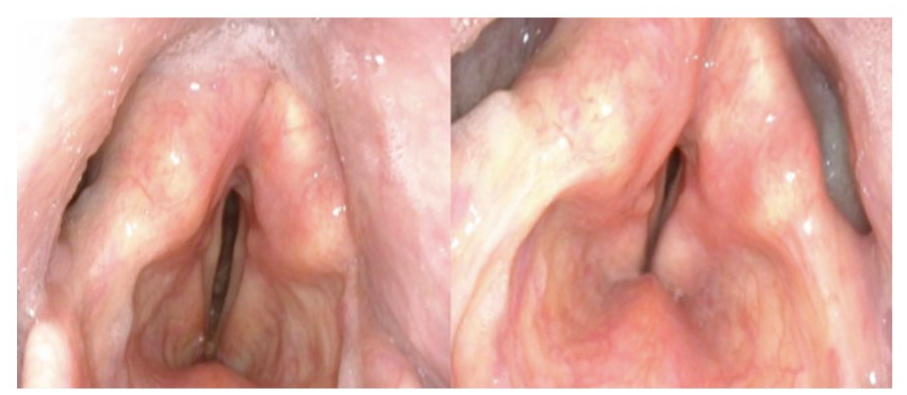
Photos from laryngostroboscopy taken during vocal cord abduction (left) and adduction (right). During abduction, fibrous tissue at the posterior glottis is seen. During adduction/respiration, some glottic closure is seen, but with a posterior glottic gap. Both the true and false vocal cords are being used by the patient for phonation.
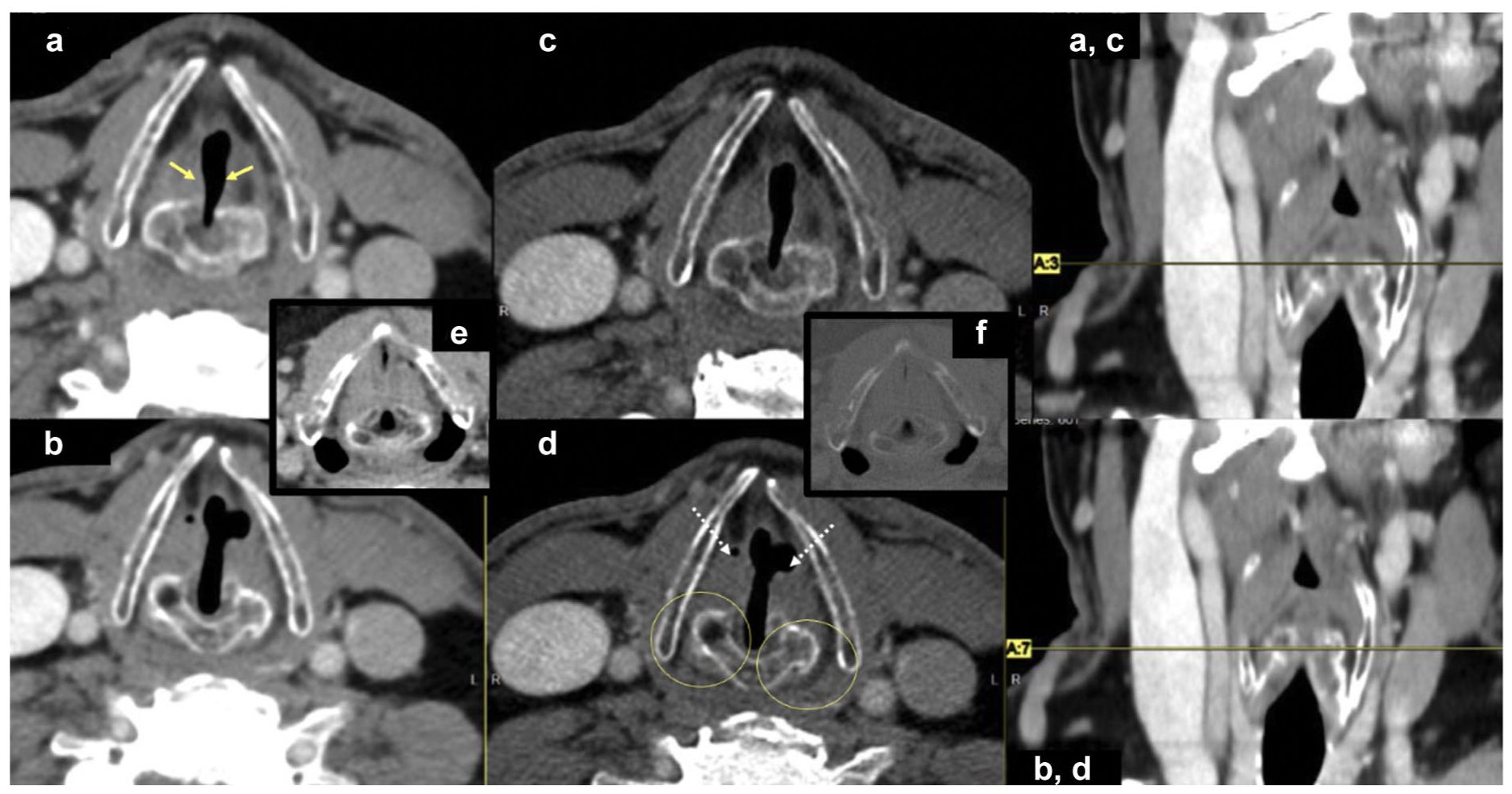
CE-CT images (a, b: soft tissue and c, d: bone window) obtained at the upper (a, c) and lower (b, d) arytenoid cartilage levels, demonstrating characteristic findings of bilateral vocal cord palsy (adduction of true vocal cords (yellow arrows), prominence of the laryngeal ventricles (dashed white arrows), and cricoarytenoid cartilage fusion (yellow circles)). Inserts (e, f) show an age-matched normal control in soft tissue and bone window, respectively. CE-CT, contrast-enhanced computed tomography.
On retrospective review of the patient’s prior CT imaging from 8 years prior, which was initially reported as normal, similar findings were seen and were largely unchanged from the present imaging. Clinical examination was otherwise unremarkable, revealing no other identifiable causes. The absence of any nerve lesion or central nervous system pathology, along with the persistence of CT findings without progression, strongly suggests cricoarytenoid joint fixation secondary to psoriatic arthritis.
Surgical intervention was discussed with the patient. Options include a tracheotomy or a laser posterior cordotomy ± partial arytenoidectomy to improve aperture of the glottic airway, but this would potentially come at the expense of some voice quality and increased risk of aspiration during deglutition. Although his breathing does reduce his ability to be physically active, the patient had adapted well to his dyspnea on exertion, which was predictable and stable over many years; a shared decision was reached that his glottic airway was adequate, and no surgical intervention occurred.
Discussion
The cricoarytenoid joint, which connects the arytenoid and cricoid cartilages, is a synovial joint subject to systemic inflammatory processes that affect peripheral joints.3,4 Cricoarytenoid arthritis has previously been associated with rheumatoid arthritis, ankylosing spondylitis, and other autoimmune conditions, including Sjögren’s syndrome, systemic lupus erythematosus, dermatomyositis, juvenile chronic arthritis, and autoimmune hepatitis.5 -7 The pathogenesis of rheumatologic cricoarytenoid joint fixation remains unclear but is presumed to begin with synovitis, leading to cartilage erosion and, in chronic cases, resulting in fibrosis and subsequent ankylosis of the joint. 4
While rheumatoid arthritis is the most common rheumatologic disease associated with laryngeal involvement, psoriatic arthritis can also affect the cricoarytenoid cartilage, although this is extremely rare. 4 On review of the literature, the first documented case of cricoarytenoid joint fixation in psoriatic arthritis was reported in 2021 in the Journal of Rheumatology. This landmark case involved a 71-year-old man with psoriasis vulgaris and joint pain who developed progressive dyspnea, stridor, and hoarseness. Further workup revealed bilateral cricoarytenoid joint fixation, while laboratory testing ruled out rheumatoid arthritis as the cause. 8
Based on the single previously reported case, along with treatment patterns in other rheumatic conditions, management of rheumatologic cricoarytenoid joint fixation may include a combination of both medical and surgical treatment.4,8 Medical options include steroids, biologic disease-modifying antirheumatic drugs, and voice therapy. Surgical treatment is typically pursued concurrently when airway obstruction is present. Tracheostomy is the most effective surgical treatment for severe cases.
Conclusion
Rheumatologic diseases may affect any synovial joint in the body, including the cricoarytenoid joint, but documented cases of psoriatic arthritis association are extremely rare. We present only the second published case, following the 2021 report, which represents the first formal documentation of this association. Healthcare providers should be aware of this potential complication, particularly in psoriatic arthritis patients presenting with voice changes, breathing difficulties, or throat symptoms with no other identifiable cause. Early clinical and radiological recognition and appropriate treatment are crucial, as bilateral cricoarytenoid joint involvement can lead to life-threatening airway obstruction requiring emergency intervention. 9
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Fully informed, voluntary, explicit consent was received from the patient for publication of their case by their healthcare provider. Our institution does not require written consent for the publication of case reports.
Author Contributions
K.T. was involved in methodology, investigation, writing, and visualization. L.M. was involved in the investigation. R.C. was involved in conceptualization, investigation, resources, and reviewing and editing. M.S. was involved in conceptualization, methodology, investigation, reviewing and editing, visualization, supervision, and project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.