
Abstract
Objectives:
This study aimed to analyze the effects of intraoperative neuromonitoring (IONM) on the prevalence of vocal cord palsy (VCP) in thyroid surgery.
Methods:
Data from 493 patients (839 nerves at risk [NAR]) who underwent thyroid surgery between July 2014 and May 2016 were retrospectively evaluated. The patients were divided into 2 groups: Group 1 (G1) consisted of patients who underwent surgery without IONM, whereas group 2 (G2) consisted of patients who underwent surgery with IONM. The surgical techniques were identical, and experienced surgeons performed the procedures in both groups. Intraoperative neuromonitoring was performed in compliance with the International Neural Monitoring Guidelines.
Results:
In total, 211 patients (170 female, 41 male) with 360 NAR were included in G1, and 282 patients (220 female, 62 male) with 479 NAR were included in G2. The number of VCP per NAR in G1 and G2 was 33 (9.2%) and 27 (5.6%), respectively (P = .005). The number of transient VCP per NAR in G1 and G2 was 27 (7.5%) and 23 (4.8%; P = .230), respectively. The number of permanent VCP per NAR in G1 and G2 was 6 (1.7%) and 4 (0.8%; P = .341), respectively. Bilateral VCP was detected in 4 (2.7%) patients in G1, whereas there was no patient with bilateral VCP in G2 (P = .033).
Conclusions:
Intraoperative neuromonitoring may decrease the incidence of total VCP and prevent the development of bilateral VCP, which has unfavorable results for both patients and health-care professionals.
Introduction
Thyroidectomy, a widely performed surgical procedure in endocrine surgery, has been used in the treatment of benign and malignant thyroid pathologies for almost 100 years since the establishment of the surgical technique by Theodore Kocher (1841-1917). 1 Despite this, recurrent laryngeal nerve palsy (RLNP) is still considered the most significant and severe complication of thyroid surgery. 2 Identification and complete visualization of the recurrent laryngeal nerve (RLN) is the gold standard for preserving it intraoperatively. Despite careful identification and anatomically complete visualization of the RLN, postoperative RLNP still occurs in some cases. 3
The symptoms and clinical manifestations of vocal cord palsy (VCP) vary. Symptoms of breathy dysphonia, dysphagia, and liquid aspiration in unilateral RLNP generally cause mild discomfort and are more tolerable, whereas bilateral RLNP is a life-threatening condition resulting in a tracheostomy during the early postoperative period. 3
Another aspect of RLNP is the significant difference in health-care charges between patients with and without VCP. Patients with VCP or third-party payers generally have higher health-care costs than those without VCP, and this significant difference is unrelated to other patient factors such as malignancy, obesity, and thyroid gland weight. 4
Jeannon et al 5 searched MEDLINE and published a meta-analysis of 27 studies that included >25 000 patients who underwent thyroid surgery. The rates of transient and permanent VCP were 9.8% (1.4%-38.4%) and 2.3% (0%-18.6%), respectively. Another meta-analysis 6 of 40 articles with 30 922 patients estimated the incidence of bilateral RLNP in patients who underwent total thyroidectomy with and without intraoperative neuromonitoring (IONM). They reported that bilateral VCP had a lower incidence in the IONM group than in the non-IONM group (2.43% [1.55%-3.5%] vs 5.18% [2.53%-8.7%]).
To decrease the incidence of transient and permanent RLNP, IONM has been accepted as a risk-reducing tool. 7 Although IONM has been used in endocrine surgery for >40 years, its role during thyroid surgery remains controversial, as no consensus exists on its role in reducing RLNP incidence. 8,9 This study aimed to analyze the effects of IONM, especially in reducing the incidence of VCP, by comparing the results of thyroidectomies performed with or without IONM.
Patients and Methods
After study approval from the institutional review board, the data of patients who underwent thyroid surgery for benign or malignant diseases, between 2014 and 2016, were retrospectively evaluated. The surgical procedures included lobectomy, total thyroidectomy, completion thyroidectomy (removal of the contralateral thyroid lobe in a patient who had previously undergone thyroid lobectomy alone), revision thyroidectomy (removal of remnant/recurrent thyroid tissue in a patient who had undergone thyroid surgery on the ipsilateral side), prophylactic or therapeutic (unilateral or bilateral) central neck dissection with total thyroidectomy, and therapeutic selective lateral compartment neck dissection with total thyroidectomy. Patients who underwent subtotal thyroidectomies were excluded from the study. Moreover, patients with preoperative RLNP, intentional nerve transection for tumor invasion, and RLN failure due to IONM equipment-related technical problems and those who did not undergo preoperative or postoperative vocal cord examinations were excluded. Patients were divided into 2 groups according to intraoperative IONM use: Group 1 (G1) included patients who underwent surgeries without IONM, whereas group 2 (G2) included patients who underwent surgeries with IONM.
Surgical Technique
All surgical procedures were performed under general anesthesia. A standard endotracheal tube without electromyography (EMG) electrodes was used during intubation in G1 patients, whereas the NIM 3.0 standard reinforced EMG endotracheal tube (Medtronic Xomed, Jacksonville, Florida) was used in G2 patients. No neuromuscular blocking agent (rocuronium) was applied, except for low-dose neuromuscular blockade during anesthesia induction in G2.
The surgical techniques were identical, and experienced surgeons performed the procedures in both groups. An anterior approach between the strap muscles was used for primary thyroidectomy, whereas a lateral approach between the strap and sternocleidomastoid muscles was used in patients who underwent reoperations. The initial side of surgery was decided according to malignancy localization and/or side of the dominant lobe or nodule. In some patients, especially those with short necks, huge goiters, or substernal goiters, the strap muscles were transected from one-third of the cranial part of the sternothyroid and sternohyoid (or only from the sternothyroid) muscles with the help of energy devices to provide better exposure. The vagal nerve on the operative side was identified and stimulated directly by dissection of the carotid sheath between the middle and lower thyroid poles. The RLN was usually identified in the mid-polar level, around the inferior thyroid artery. Once the RLN was identified, the thyroid gland was carefully dissected from the anterior and medial surfaces of the RLN until laryngeal entry under the cricopharyngeus muscle.
Intraoperative Neuromonitoring Technique
The standard IONM equipment, induction, maintenance anesthesia, tube positioning, EMG definitions, and data interpretation complied with the International Neural Monitoring Guidelines. 10 A sterile, single-use monopolar stimulator probe (Medtronic Xomed) was used for nerve stimulation, with current amplitude between 1 and 2 mA.
Intraoperative neuromonitoring was applied as a 4-step procedure (V1, R1, R2, and V2), according to the International Neural Monitoring Guidelines. 10 The nervus vagus was identified and stimulated before RLN identification to verify IONM system function, and the EMG wave obtained from the vocal cords was saved as V1. The RLN was identified at the tracheoesophageal groove, and if the RLN could not be identified during dissection, the stimulator probe was used for identification. The EMG wave obtained from the RLN, when the RLN was first detected and stimulated, was saved as R1. After thyroid lobectomy, the RLN was restimulated from its most proximal portion, and the obtained waves were saved as R2. The nervus vagus was stimulated after complete hemostasis of the operative side, and the obtained waves were saved as V2.
After completion of the 4-stage EMG wave assessment, the results were evaluated according to the IONM study group guideline. Electromyography waves ≥100 μV from the vocal cord, due to nervus vagus or RLN stimulation, were defined as a positive EMG response. At completion of surgery, EMG amplitude <100 μV or complete signal loss was defined as signal loss.
The preoperative diagnoses were grouped as nodular goiter (NG; toxic or nontoxic), Graves’ disease, recurrent NG, malignant, and recurrent malignant. The malignant group comprised patients whose fine-needle aspiration biopsies showed malignancy or suspected malignancy.
Patients were also classified based on the risk of intraoperative nerve injury. Patients with multinodular goiter (MNG) without retrosternal extension were assigned to the low-risk group, whereas patients who underwent thyroidectomy with or without central neck dissection due to malignancy, those with Graves’ disease, or those with retrosternal or recurrent goiters were classified in the high-risk group.
Intraoperatively, when the EMG signal was lost from the nervus vagus and/or RLN, surgery was discontinued, and the contralateral thyroid lobe was excised in a second surgery to prevent bilateral VCP. This surgery was referred to as “staged thyroidectomy,” and patients who underwent this surgery were also evaluated.
Postoperative Evaluation
All patients underwent vocal cord examination by an experienced laryngologist. Serial laryngoscopic examinations were performed for patients with VCP on postoperative days 15 and 30, and every month thereafter until the sixth postoperative month. Recurrent laryngeal nerve palsy was classified as permanent or temporary and unilateral or bilateral. If there was no evidence of recovery after 6 months, the VCP was considered permanent. No financial association exists between the authors and companies whose IONM and/or related products were used during this study.
Statistical Analyses
Vocal cord palsy incidence was calculated based on the number of nerves at risk (NAR). Using the SPSS software, the differences between continuous and categorical variables were assessed with the Mann-Whitney U and Fisher exact tests and χ2 test, respectively. P values ≤.05 were considered significant.
Results
There were 211 patients (170 women, 41 men) with 360 NAR in G1 and 282 patients (220 women, 62 men) with 479 NAR in G2. The demographic patient characteristics were similar between the groups (Table 1). There was a significant difference in preoperative diagnosis between the groups (P = .030). Recurrent goiter was more frequent in G2 (5, 3%) than in G1 (0, 9%). There were 62 (29.4%) and 85 (30%) unilateral and 149 (70.6%) and 198 (70%) bilateral interventions in G1 and G2, respectively. Although the number of patients with central neck dissection was significantly higher in G2 (0.28% vs 10.44%, P < .001), no significant difference was found in low- or high-risk surgeries.
Demographic Characteristics of Patients, Type and Side of Surgical Procedures, and Number of Patients According to Each Risk Group.a
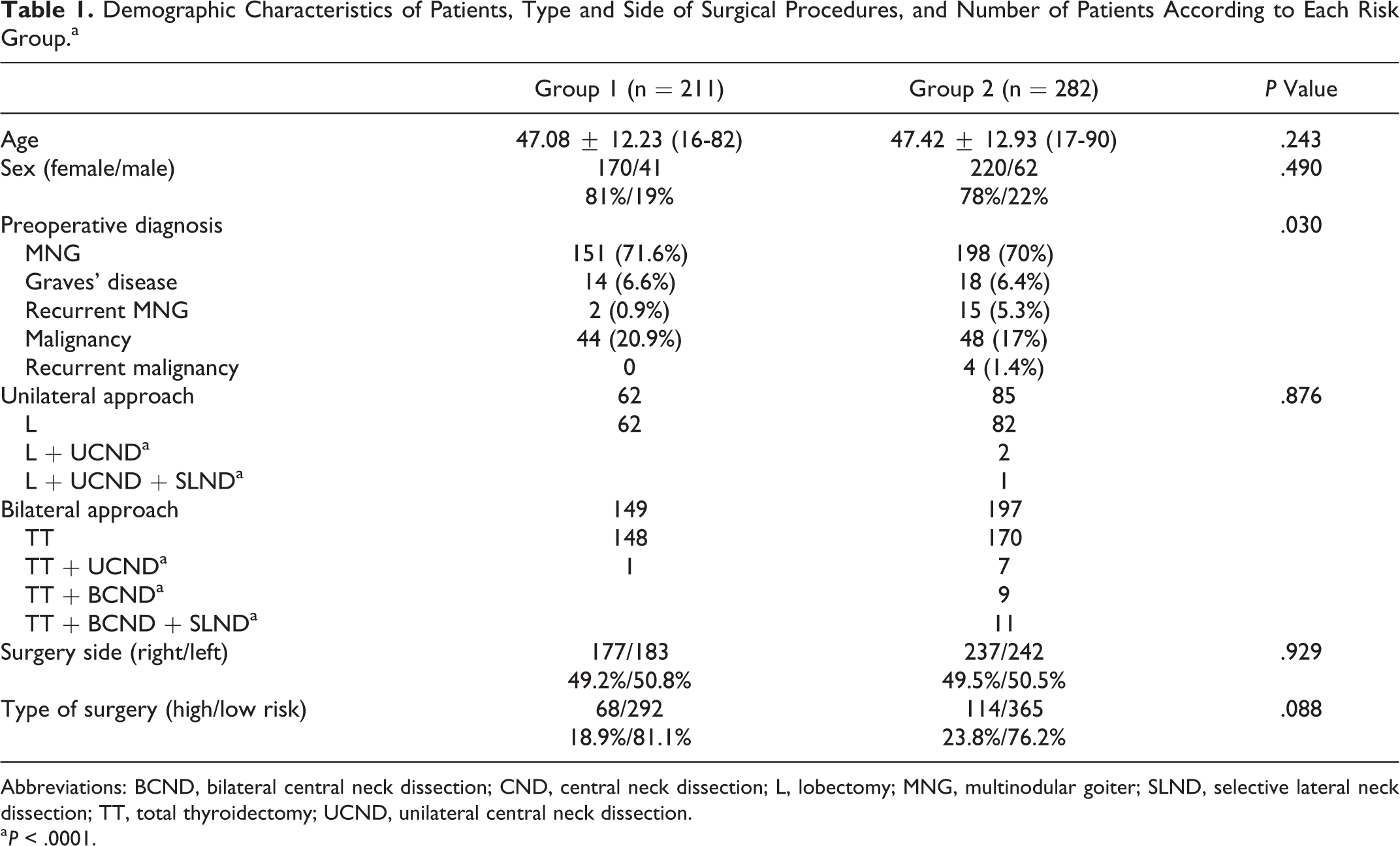
Abbreviations: BCND, bilateral central neck dissection; CND, central neck dissection; L, lobectomy; MNG, multinodular goiter; SLND, selective lateral neck dissection; TT, total thyroidectomy; UCND, unilateral central neck dissection.
a P < .0001.
The VCP per NAR rates in G1 and G2 was 33 (9.2%) and 27 (5.6%), respectively (P = .05). The number of total VCPs was significantly lower in G2 (P = .05). Bilateral VCP was detected in 4 (2.7%) patients in G1, whereas no VCP was detected in G2 (P = .033). The number of permanent and temporary VCPs was higher in G1, but without significance (Table 2).
Numbers and Rates of Nerves at Risk in the Groups.
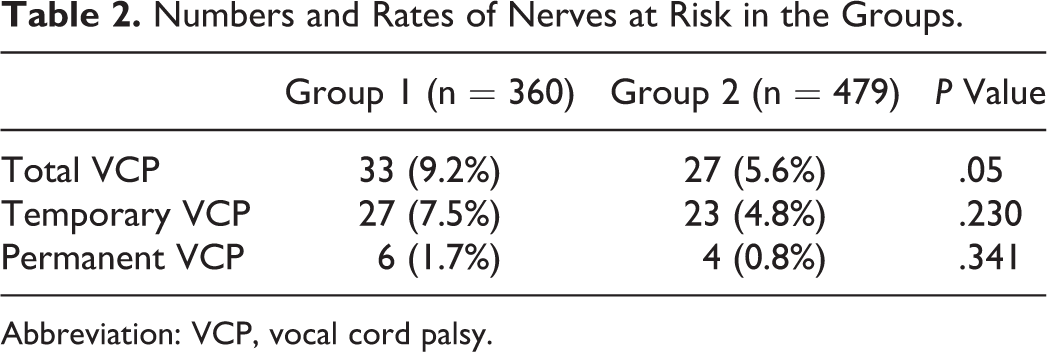
Abbreviation: VCP, vocal cord palsy.
During total thyroidectomy in 1 G1 patient, the RLN was mistakenly bound at its entry to the larynx, which was assumed to be vascular tissue. The RLN was released carefully, the operation completed, and the contralateral side treated with staged thyroidectomy. Nine patients in G2 who underwent bilateral surgery were also treated with staged thyroidectomies due to EMG signal loss. Postoperative VCPs were detected in all 10 patients. Staged thyroidectomies were significantly more frequent in G2 (P = .049).
Bilateral VCP was detected in 4 patients in G1, significantly higher than that in G2 (2.7% vs 0%, P = .033; Table 3). The VCPs of these patients were temporary, and no tracheostomies were performed due to sufficient aperture (2-3 mm) between vocal folds. These patients were followed in the intensive care unit (ICU) on the first postoperative day. On the second postoperative day, they were extubated and received nasal oxygen in the ICU. They had an average hospital stay of 8 to 10 days and managed their respiration without extra effort; oxygen saturation levels were normal upon discharge. The vocal fold functions normalized within 1 to 4 months postoperation.
Numbers and Rates of Bilateral VCP in the Groups.
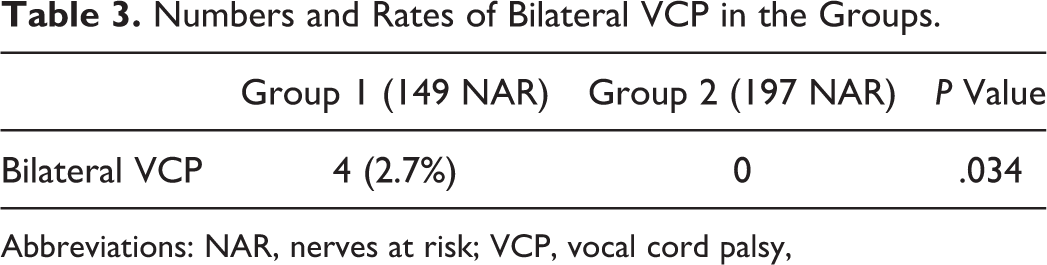
Abbreviations: NAR, nerves at risk; VCP, vocal cord palsy,
When the surgeries were grouped as low risk (Table 4) or high risk (Table 5), the number of total, temporary, and permanent VCPs was higher in G1 than in G2, without statistical significance.
Numbers and Rates of Nerves at Risk During Normal-Risk Thyroid Surgeries.
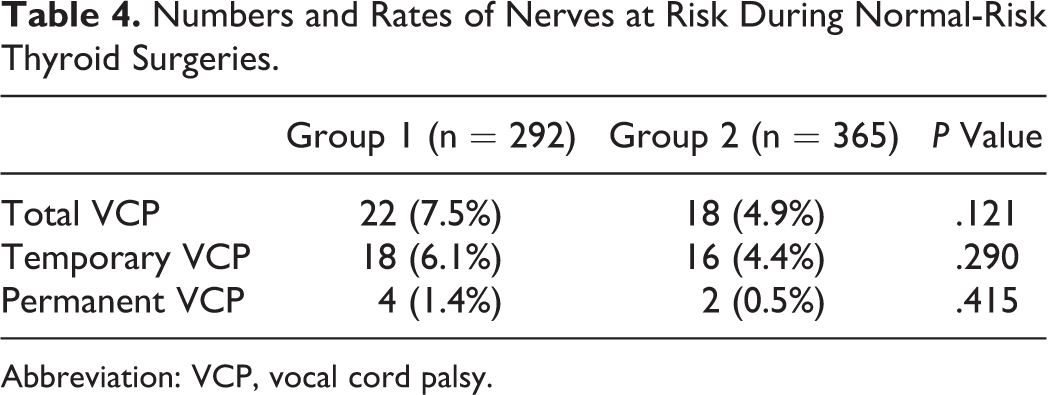
Abbreviation: VCP, vocal cord palsy.
Numbers and Rates of Nerves at Risk During High-Risk Thyroid Surgeries.
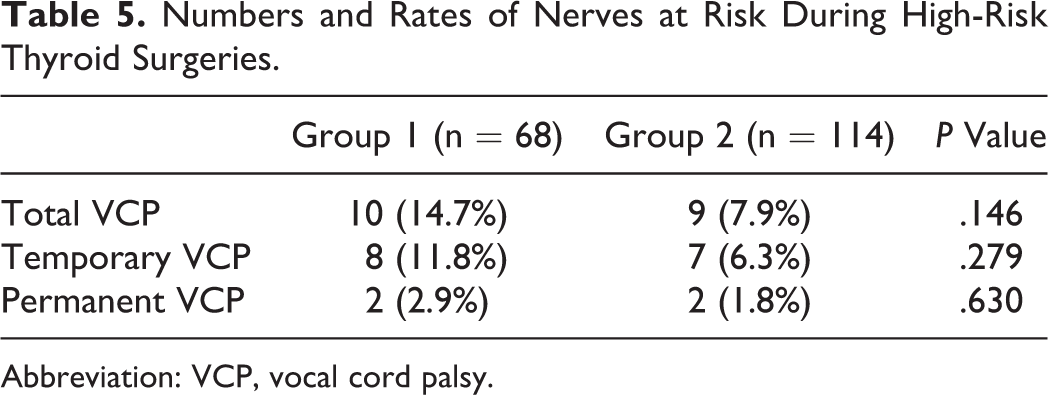
Abbreviation: VCP, vocal cord palsy.
Discussion
Recurrent laryngeal nerve identification is the gold standard for nerve protection. According to experienced endocrine surgeons, in 6.8% to 11.5% of thyroidectomies, the RLN cannot be identified. This increases to 42% to 66% in patients with recurrent disease. 11 Intraoperative neuromonitoring facilitates RLN identification, and with this, almost every nerve can be identified. 12 After RLN identification, IONM facilitates nerve mapping and allows a more secure dissection. 13
The preservation and identification of RLN anatomic integrity do not ensure proper functioning postoperatively. Although only 15% of nerve injuries can be detected physically, 100% of RLN injuries can be identified with IONM intraoperatively. 14,15
Although IONM contributes to the identification, mapping, and intraoperative determination of RLN function, its effects on VCP remain controversial. In our study, the VCP per NAR rates were lower in G2 than in G1 (5.3% vs 9.2%, P = .05). The rates for both transient and temporary VCP per NAR were higher in G2, without statistical significance. This may be due to the low NAR in each group. Although the rate of temporary VCP per NAR in G1 was lower than that in G2 (23 vs 27), at least 1244 NAR for temporary VCP and 1620 NAR for permanent VCP are required for a study power of 80% and to calculate significant differences.
Despite several well-constructed, high-volume studies with different results, it is commonly accepted that IONM reduces RLN injuries. A study on >4000 patients with MNG in Germany claimed that IONM significantly reduces the temporary VCP ratio from 2.1% to 1.4% and permanent VCP from 0.8% to 0.4% (P < .05 for each group). 16 In contrast, a multi-institutional study in Germany with >16 000 patients and 30 000 nerves concluded that the effects of IONM on RLN injuries were not significant between groups with or without IONM, except in patients with immunogenic goiter. 2 A randomized prospective clinical study 17 reported that IONM significantly decreased transient VCP (P = .011, 1.9% lower than that with visualization alone; the prevalences of RLN injury, transient RLN paresis, and permanent RLN palsy were 2.3% [P = .007], 1.9% [P = .011], and 0.4% [P = .368] lower, respectively, than that with visualization alone) in high-risk patients treated with and without additional monitoring, especially patients who underwent high-risk thyroidectomies (2.6% vs 6.3%, P = .003; 3.7% lower overall RLN morbidity [P = .005] and 2.9% lower transient RLN morbidity [P = .011]). In the same study, the permanent VCP rate was lower in G2 than in G1, without statistical significance due to an insufficient sample size. According to a multivariable analysis of patients in the Scandinavian Quality registry for Thyroid, Parathyroid, and Adrenal Surgery, IONM was not associated with low early VCP rates but was associated with low permanent VCP rates (OR, 0.43, 0.19-0.93). 18
In high-volume centers, permanent and temporary VCPs are complications with low prevalence. Due to this rareness, the sample size for obtaining significant differences between groups is generally insufficient in the current literature. 17 To confirm such results, high-quality, multicenter, prospective, randomized, and well-categorized studies with sufficient patient populations are needed. However, planning a multicenter randomized study is difficult. Although some meta-analyses attempt to overcome this, their heterogeneity limits their power. Some meta-analyses have found that IONM has no significant effect on VCP, 4,19 whereas others have found that it reduces the transient VCP rate. 20,21 A recent meta-analysis of 3 randomized controlled and 31 nonrandomized studies with >59 000 NAR found that IONM decreased the permanent and temporary VCP rates, and the results were robust enough to reveal the significance of this observation. 22 Although IONM use as a standard technique during total thyroidectomy remains controversial, the selective use of IONM during high-risk thyroidectomies, such as reoperations and thyroidectomy for malignancy, thyrotoxicosis, or retrosternal goiter, is recommended. 23
In this study, although the total (7.9% vs 14.7%), temporary (6.3% vs 11.8%), and permanent (1.8% vs 2.9%) RLNP rates were lower in patients who underwent high-risk thyroidectomies in G1, this difference lacked statistical significance. Although the number of high-risk surgeries was similar in both groups, patients with recurrent goiter (5, 3% vs 0.9%, P = .03) and central neck dissection were significantly higher in G1 (P < .0001). Despite the low number of high-risk surgeries, our preliminary results are compatible with those of previous studies that recommend IONM for such surgeries.
Bilateral VCP is a serious and catastrophic complication of thyroidectomy. There were no patients with bilateral VCP in G2; however, 4 patients had bilateral VCP in G1 (0% vs 2.7%; P = .034). There were 9 patients in G2 whose surgeries progressed to staged thyroidectomies due to signal loss during the surgery. In 1 patient in G1, the surgeon mistakenly ligated the RLN, realized the error, and released it just before cutting. This patient was the only patient who required staged thyroidectomy in G1. The ratio of staged thyroidectomy was significantly higher in G2 (P = .049). With IONM, RLN injury can be detected intraoperatively, even if the nerve is anatomically intact, and the surgery can be performed as staged thyroidectomy to prevent bilateral VCP. In patients whose surgeries do not progress to staged thyroidectomies despite intraoperative signal loss, 17% can develop bilateral VCP postoperatively. 24,25
Early bilateral VCP detection is extremely important. In patients with severe respiratory problems, if an adequate respiratory tract is not achieved by tracheostomy or reintubation, the patients may develop anoxic brain injury and even die. 26 In bilateral VCP, the vocal cords may be in the median or paramedian position. In patients with vocal cords in the paramedian position, airway clearance is often sufficient, and there may not be any obvious complaints about breathing at rest, or the complaints may be mild. Intubation or tracheostomy may be unnecessary for these patients. However, this may lead to delayed diagnosis. 27 In our study, although no patients with bilateral VCP required tracheostomy, the hospitalization duration was significantly longer. This prolonged hospitalization increases the postoperative health-care cost. Moreover, when these patients were discharged, their effort capacity was limited due to respiratory distress, causing loss of work power.
The most important limitation of this study was its retrospective nature and the insufficient number of NARs. However, since IONM has been routinely used in thyroid surgery after this study in our clinic, it is impossible to perform a prospective or retrospective study in which the number of nerves in the IONM group increases. We believe that this study, which included 839 NARs, will contribute to the medical literature.
Therefore, IONM may decrease the incidence of total VCP and prevent bilateral VCP, which has unfavorable results for patients and health-care professionals.
Footnotes
Authors’ Note
Informed consent was obtained from all individuals who participated in the study. K.K., M.U., and A.I. contributed to study concept and design; N.A., E.B., and M.F.C., contributed to acquisition of data; B.C., and K.K. contributed analysis and interpretation of data; K.K., A.I., and M.U. contributed to critical revision of the manuscript for important intellectual content; K.K., A.I., and M.U contributed to study supervision; all authors contributed to drafting of the manuscript; All authors approved the final draft of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.