
Abstract
Introduction
Vocal cords adduct for phonation and abduct for breathing in healthy people. However, there are a variety of mechanical reasons for vocal cords to malfunction. Bilateral vocal fold paralysis is a common emergent situation in the otolaryngology field, which often demands doctors’ rapid decision making and management.1,2 If the vocal cords are fixed near the midline, the glottic area becomes insufficient to serve as an adequate airway.3,4 Patients usually present with stridor, dyspnea, or other signs of difficulty breathing. 5 When an emergency room encounters a patient with suspected bilateral vocal fold paralysis, they frequently refer the patient to an otolaryngologist for an endoscopic assessment in order to assess the vocal cords’ degree of movement.
Otolaryngologists often face the decision of whether to intervene to maintain the airway through intubation or tracheostomy. 6 However, we lack any objective tool to assist in decision making. A previous study found that the maximum anterior glottic angle (GA) had a moderate capacity to predict the requirement for surgical airway intervention and a strong discriminatory capacity for the diagnosis of bilateral vocal palsy. 7 The previous report regarding similar measurements has been made. A similar objective tool does indeed exist, and we are using a different method here that may corroborate the previously-published results. 7 This tool may be useful for the assessment of other neurological laryngeal conditions and may help guide decision making in laryngeal surgery. This study intends to determine the importance of measuring the GA and area in the treatment of airway maintenance to the detriment of the best decision regarding interventions.
Materials and Methods
We reviewed the cases of bilateral vocal fold paralysis at Shuang Ho Hospital from January 2008 to December 2023. There were 33 cases of bilateral vocal fold paralysis. The research project was approved by the Institutional Review Board of the Taipei Medical University-Shuang Ho Hospital (N201912032). However, due to the limitation of capturing images with a portable fiberscope, only 26 of 33 cases had images uploaded into the picture archiving and communication system that were reviewable. After collecting the images of these 26 patients, we took the ones with the GA of the vocal cords as the end inhalation period. The widest opening of the glottis occurs when one is inhaling. The GA was defined by lines connecting the anterior commissure with each inner surface of the vocal process, as proposed in previous studies.8,9 The GA was got after a series of inhaling pictures. Two doctors measured the angles independently and then averaged the 2 (Figure 1). An Apple protractor app was applied to measure the angles. The interrater reliability is good between the 2 doctors. The GA measurement from the 2 doctors was almost the same. The categorical outcome variables were used as dependent variables and the continuous covariates. An air flow meter is not available during a routine check for patient at the ER or outpatient department. The air flow per cubic meter was not taken into account for the statistics in this study.
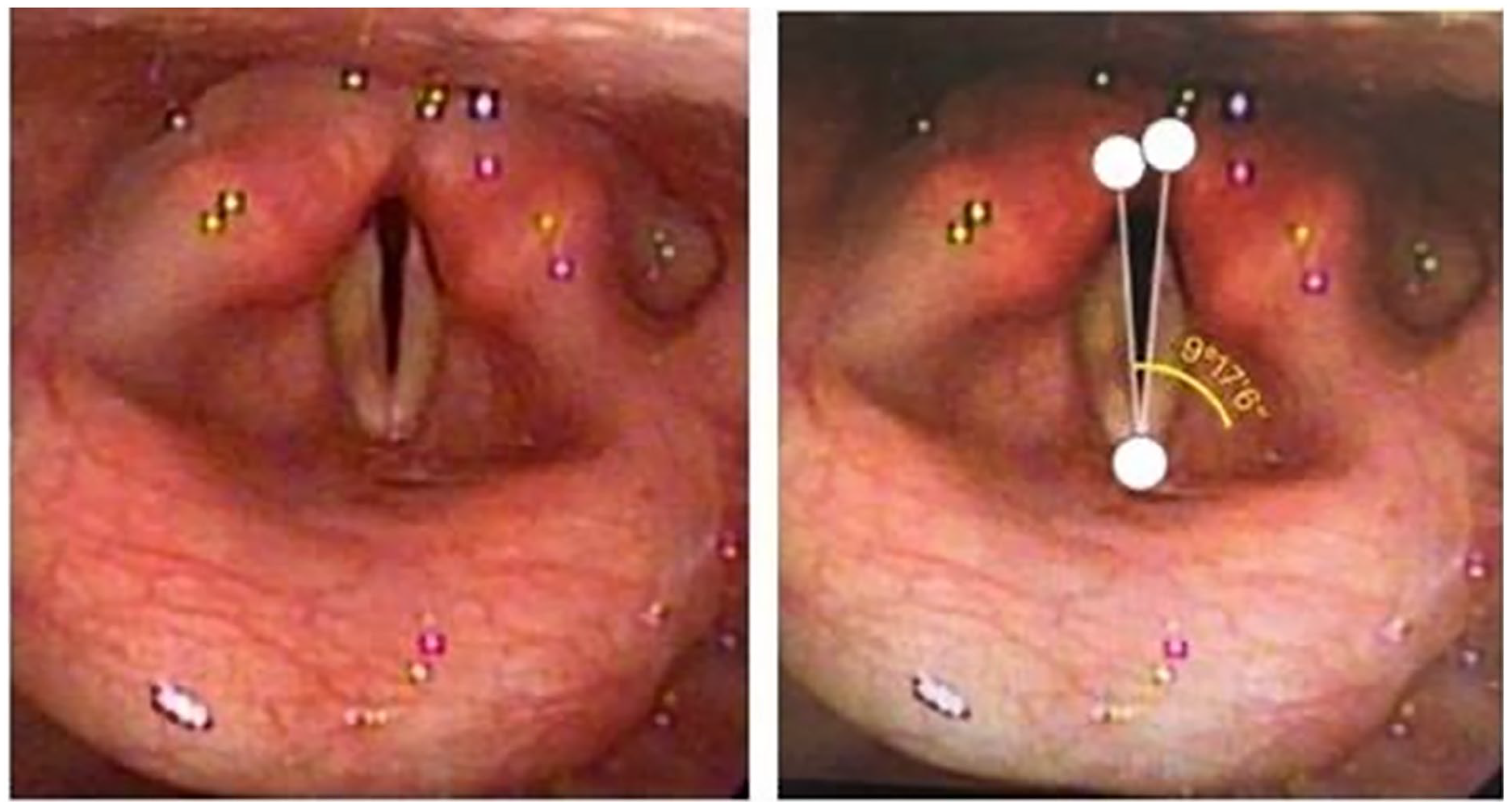
A scope view of bilateral vocal fold paralysis post total thyroidectomy (left). The measurement of glottic angle was standardized from the anterior commissure to the medial side of each vocal process (right).
Glottic area was also calculated with the equation of ½ × (average vocal cord length according to gender in Taiwanese data [10])2 × sine (angle). The glottis area of bilateral vocal palsy is almost an isosceles triangle. Medical records were reviewed, and any procedures to maintain a secure airway including intubation and tracheostomy were documented. During an emergency, trying to get the real length of the cords is impractical. So, we used average values of Taiwan’s population to calculate the glottis area.
The Microsoft Excel® and SPSS® (Version 24.0 for Windows; SPSS Inc, Chicago, IL, USA) programs were used for statistical analysis. The receiver operating characteristic (ROC) curve of GA and area was made. 7 The demographic data of patients were analyzed with average and standard deviation. The GA, glottic area, and need for intervention were calculated and statistically analyzed with logistic regression. Among the 26 patients, 17 had intubation/tracheostomy due to respiratory failure and belonged to the intervention group. The rest was a nonintervention group. A P value less than .05 was regarded as statistically significant.
Result
Among the retrospective study of 26 patients, 17 had intubation/tracheostomy due to respiratory failure. Nine of them kept stable vital signs without invasive airway management (Table 1). We checked the average age between the intervention and nonintervention groups. The mean age was 63.2 ± 11.1 years, 60.7 ± 6.5 years in the intervention group, and 68.1 ± 16.1 years in the nonintervention group. No significant difference between the age distributions of the 2 groups was noted (Table 2).
The Character of Each Case and the Favored Etiology of Bilateral Vocal Paralysis.

Abbreviations: CCRT, concurrent chemotherapy and radiotherapy; F, female; M, male; SqCC, squamous cell carcinoma.
Age of Intervention and Nonintervention Groups.
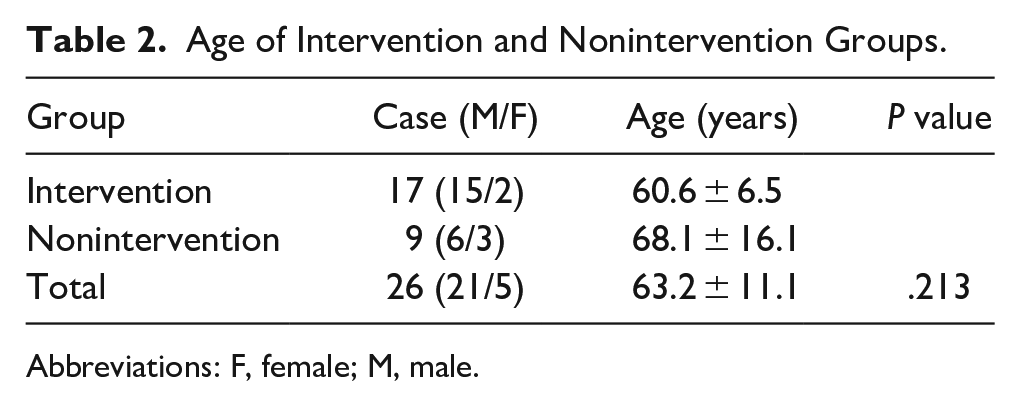
Abbreviations: F, female; M, male.
The average GA was 10.3 ± 7.3°. The intervention group (N = 17) had an average GA of 7.1° ± 3.7°. The nonintervention group (N = 9) had an average GA of 16.3° ± 8.9°. The average glottic area was 18.7 ± 10.2 mm2, with 4.2 ± 7.5 mm2 in the intervention group and 27.2 ± 9.4 mm2 in the nonintervention group (Table 3).
The glottic angle and area of group intervention and non-intervention groups.

OR : odds ratio
As we applied logistic regression comparing the relationships between the GA and area with the outcome of intervention, both groups showed statistical significance. Each 1° increase in GA reduced intervention risk 0.263 times. And each 1 mm2 gain in glottic area decreased the intervention rate 0.776 times. The ROC curve of the GA and area is shown in Figure 2. The area under the curve (AUC) was 0.97 for GA and 0.90 for glottic area, which both represent outstanding discrimination. As for need for intervention, the best cutoff point of the GA was set at 12.2 degrees and the best cutoff point of the glottic area was set at 25.2 mm2 (Tables 1 and 4; Figure 3).
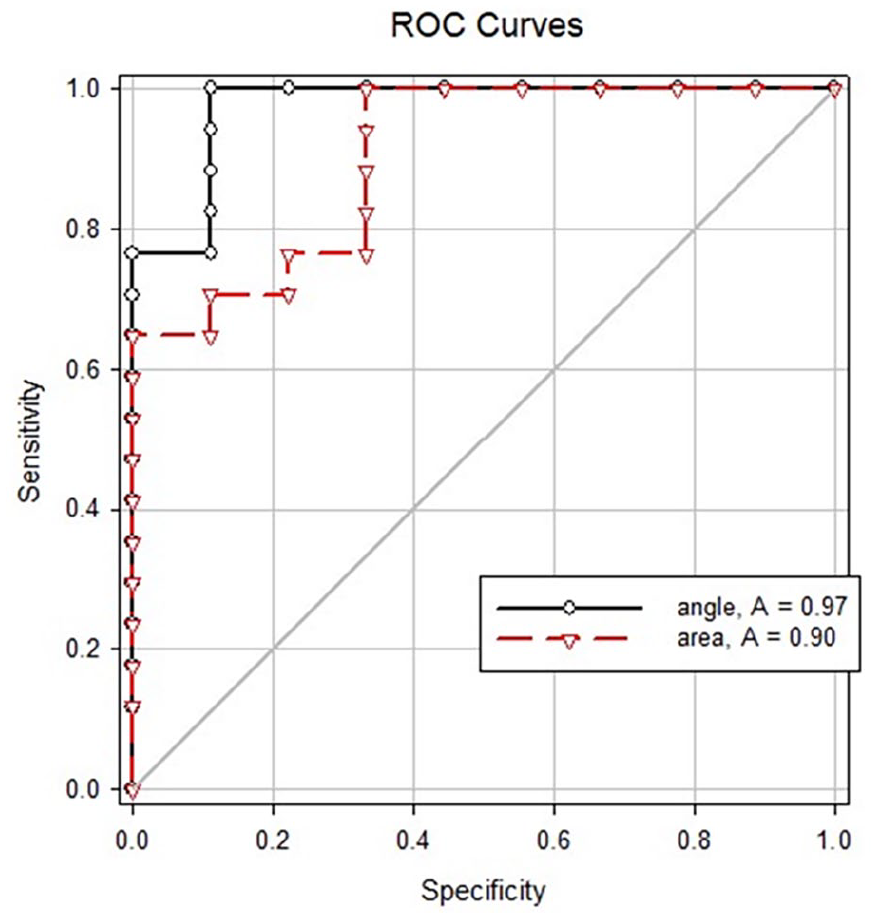
ROC curve of glottic angle and area. The AUC was 0.97 for glottic angle and 0.90 for glottic area.
AUC and the Cutoff Point of Glottic Angle and Area.
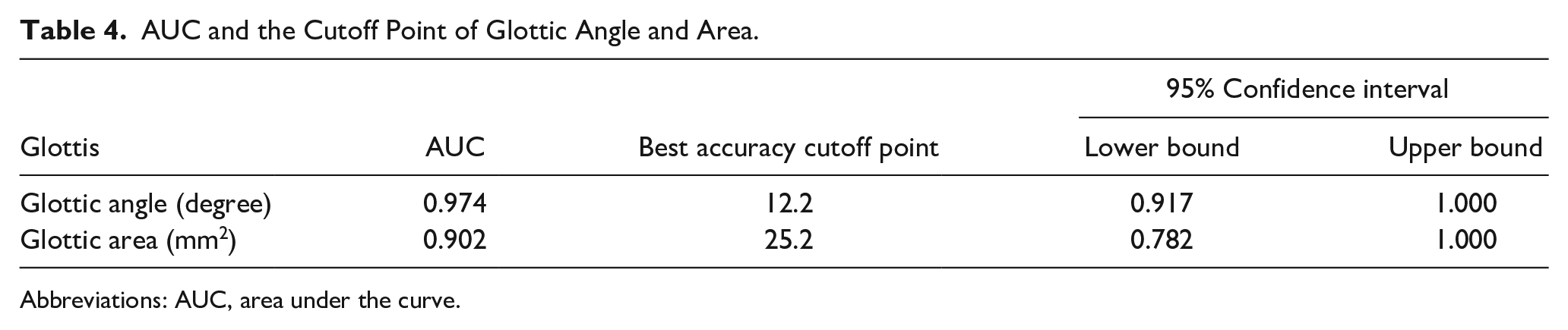
Abbreviations: AUC, area under the curve.
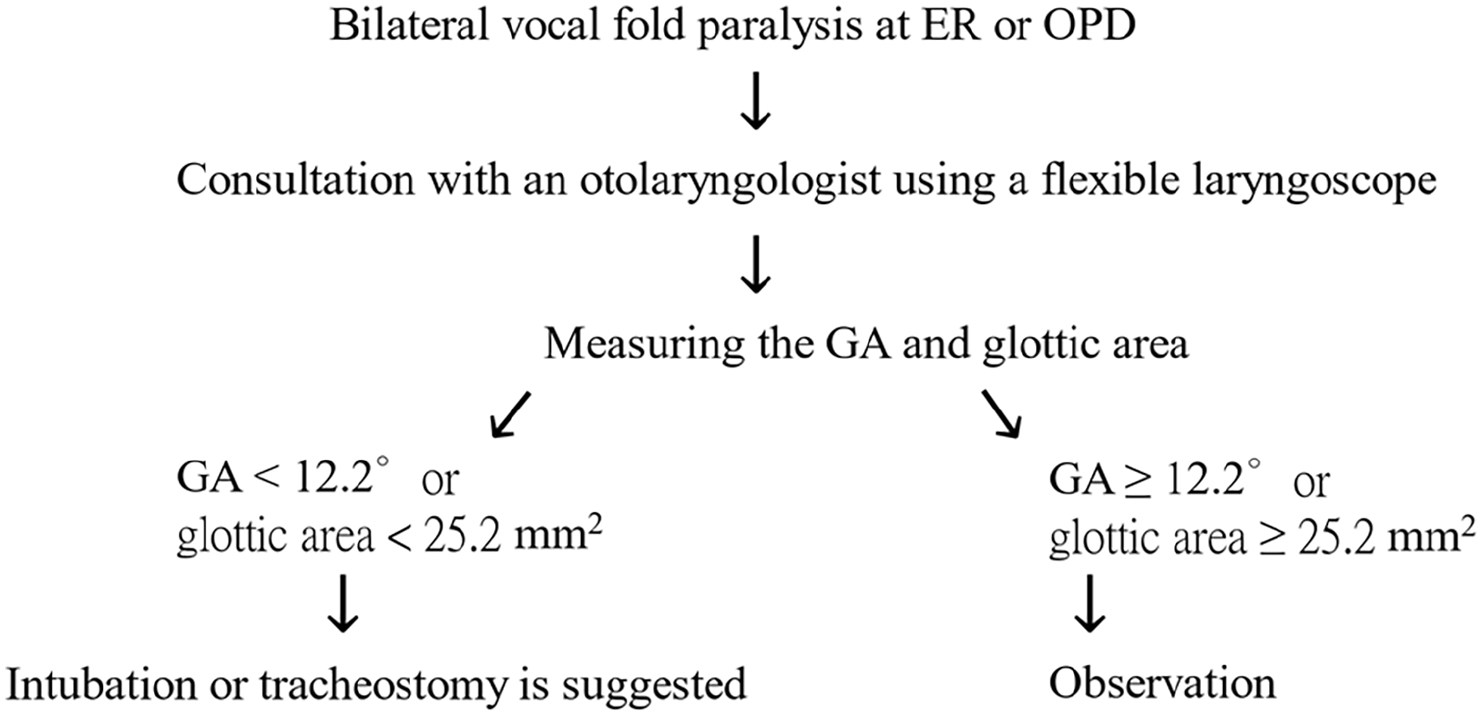
Flow diagram for a bilateral vocal fold paralysis patient.
Discussion
Bilateral vocal fold paralysis might show hoarseness, breathy voice, easy choking, dyspnea, or stridor. 4 In acute life-threatening situations, the patient should be intubated or undergo a tracheostomy to reestablish a patent airway. 4 A tracheotomy can also be avoided by other methods, such as arytenoidectomy or chordectomy. 4 For its reversibility, the suture laterofixation technique is also an alternative in selected patients. 5 In a vertical view of any angle, the degree of the angle is the same as to its original measurement. The scopic images of GA that results are similar to what we would see if we held the object away from us and viewed it along the direction of the vertical view. The measured GA degree is just the same as the original GA presenting. In this study, we suggest GA and area might be an effective factor when considering whether an invasive airway intervention is needed. According to the results of this study, emergent airway intervention, including intubation or tracheostomy, was required when GA < 12.2° or GA < 25.2 mm2. The decision to pursue surgical surgery in patients with bilateral vocal palsy is difficult to make because there are few objective measurements available. At the moment, visual estimations from videolaryngoscopy recordings during phonation are used to measure the position of the vocal folds. 10 Low-resolution descriptors are used to convey the folds' relative positions. The precise usefulness of additional instruments, such as imaging methods and stroboscopy, beyond laryngoscopy is still debatable because there are little data to support any 1 modality. 11 Although laryngeal electromyography’s invasiveness and unclear timing of testing in connection with symptom onset restrict its usefulness as a quantitative, trustworthy clinical tool, it may be helpful in forecasting functional outcomes in patients with vocal fold immobility. 12 Glottic opening is frequently not properly measured, and body plethysmography and spirometry are infrequently used as objective respiratory tests. Some studies have shown that there is little agreement among professionals when reviewing laryngoscopic examinations and that there is little interrater reliability, which suggests that diagnoses based on laryngoscopic findings are still vulnerable to interpretation.9,13 Our findings are intriguing in that they point to a solid capacity to predict which individuals will need operational airway intervention. Regardless of the cause, this study may be useful in advising patients with bilateral vocal palsy. It should be noted that patients who required surgical intervention showed statistically-smaller GA and glottic area, which may help aid decision making. The decision to pursue operational intervention is undoubtedly influenced by a wide range of additional criteria, such as other anatomic anomalies, the speed of residual vocal movement, patient comorbidities, the severity and duration of symptoms, and treatment objectives. However, we think that objective glottic measures can help otolaryngologists who are considering surgical intervention for bilateral vocal palsy or tracking vocal fold motion over time make decisions.
Second dimension multi-planar reformatting (2D MPR) is a post-processing technique that is able to create new images from a stack of images in planes other than those of the original stack. 14 We described the use of this method to study normal adult vocal folds during tidal respiration. 14 The average straight length of bilateral vocal folds is greater in men (15.39 ± 2.46 mm) than in women (12.13 ± 2.33 mm) for Taiwanese. The included angle of the bilateral vocal folds was bigger in women (42.90° ± 10.97°) than in men (38.89° ± 10.13°). Men had a greater glottic airway area (165.79° ± 48.87 mm2) than women (107.02 ± 35.18 mm2). Using the average straight length of bilateral vocal folds for males and females, we can calculate the glottic area with the sine (°) equation. As a former study proposed, the minimal glottic area for decannulation should be 38.0 mm2, and the maximal glottic area for maintaining preoperation vocal function should be 50.1 mm2 in adult bilateral vocal cord paralysis with laser aryntenoidectomy. 15 This is compatible with our findings. According to a prior study, 16 the incidence of challenging direct laryngoscopies was substantially correlated with both the glottic height and the upper airway angle. Devore et al. employed the same technique, which included the ROC curve, to identify the predictive parameters in order to determine the actual necessity for understanding how to assess the GA and area measurement. 7 The maximum GA showed a moderate capacity to predict the requirement for operational airway intervention and a strong discriminatory ability for the diagnosis of bilateral vocal fold palsy. 7 Their conclusions are supported by this investigation.
To get a quick decision for a case of bilateral vocal fold paralysis, we can make sure of the diagnosis after obtaining a good view with a laryngoscope. To determine when emergency airway intervention, including intubation or tracheostomy, is needed, we just need a quick and simple method to make a decision. This study shows that measuring the GA and glottic area is needed. We also think it is possible to perform a simultaneous assessment during laryngoscopy, using a video camera and application, without the need for a secondary assessment and photograph in the future.
There are some limitations to our study. The first and most obvious is that it consists of a relatively small number of patients. The retrospective nature of the study makes accurate long-term analysis difficult. A larger prospective study related to this idea is desired. The groups selected in this study were not randomized; there could be a selection bias. Using average values for Taiwan’s population is likely biased. Especially when there are few patients being studied in this paper, the assumption that these few patients represent the average population does not hold up well. A prompt and efficient way to measure the real cord length is needed in the future. The calculation assumes both vocal folds are the same length. With vocal fold paralysis, there can be a change in the length of the vocal folds (foreshortening) making this assumption might deviate from the real situation.
Conclusion
Bilateral vocal fold paralysis causes acute respiratory and phonation problems. This clinical emergency requires timely diagnosis and treatment by an otolaryngologist. Maintaining the airway is the paramount challenge. The question of the timing of invasive airway management still relies on the clinical experience and judgment of physicians.
This article suggests a novel method to evaluate bilateral vocal fold paralysis based on the factors of GA and area. When GA is less than 12.2° or glottic area is smaller than 25.2 mm2, airway intervention such as intubation or tracheostomy is highly likely to be required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Taipei Medical University-Shuang Ho Hospital (110SHHR-05).
Ethical Approval
The research project was approved by the Institutional Review Board of the Taipei Medical University-Shuang Ho Hospital, Taipei, Taiwan, and the number was N201912032, and all experiments were performed in accordance with relevant guidelines and regulations.