
Abstract
Orbital floor implants are commonly used to repair fractures, but complications such as infection, diplopia, or implant misplacement may develop. We describe a 68 year-old male presenting with chronic orbital pain and purulent discharge many years after undergoing repair of an orbital floor fracture with a titanium and porous polyethylene implant. Imaging and surgical findings demonstrated a malpositioned orbital floor implant in the maxillary sinus with resultant chronic infection and complete bony encapsulation of the implant – a previously-unreported phenomenon. The implant was retrieved using a combined transconjunctival, endoscopic, and Caldwell-Luc trans-antral approach. We propose that chronic low-grade inflammation and mechanical stress induced by the implant misplacement are likely causes of the observed unusual osteogenesis. Other factors including titanium surface characteristics, immune signaling, and systemic determinants have been associated with pathologic osteogenesis and can provide a broader context for this unusual finding. This case emphasizes the potential for undesirable osteogenesis in the orbit and the importance of keeping such rare complications in the differential. It also emphasizes the need for multi-approach surgical technique and multidisciplinary planning in treating complex implant-related infections and revisions.
Introduction
Orbital fractures are frequently seen after facial trauma and often involve the orbital floor and medial wall. When severe, they may displace the globe and cause loss of vision. 1 In most cases, surgical intervention is indicated in order to repair the damaged orbit and prevent potential long-term complications. However, the surgery may cause its own set of complications such as diplopia (in up to 42%), enophthalmos (in up to 27%), ectropion, and hypesthesia. 2 Infectious complications such as orbital cellulitis or abscess, estimated in smaller studies at <2%, are less common but can cause significant morbidity.3,4 Identified risk factors for infection include preexisting sinus disease or behaviors that increase sinus pressure, such as vigorous nose blowing. 5
Various materials have been utilized for reconstructing the orbital floor,6,7 such as autologous bone grafts that are biocompatible but require a secondary donor site and surgery 8 ; porous polyethylene (Medpor), which is easy to shape and supports tissue ingrowth but with a small risk of infection and extrusion 9 ; and polydioxanone, a resorbable material that is ideal for temporary stabilization of small defects. 10 Titanium mesh is one of the most commonly-used implants because of its strength, biocompatibility, ease of intraoperative manipulation, radiopacity, and overall stability. Its favorable mechanical properties and compatibility with surrounding tissues have made it a dependable option in orbital reconstruction. 4 Composite titanium and porous polyethylene orbital implants have become popular as well.
Despite all these advantages, complications associated with titanium implants have been well-documented. A long-term study has reported higher rates of postoperative diplopia and reoperation associated with titanium mesh. 11 Additional reports have described soft tissue reactions to titanium, including implant fibrosis, 12 soft tissue incorporation in the orbit and midface, 13 and orbital adherence syndrome, which may cause motility restriction and eyelid retraction. 14 One case also described a postoperative orbital abscess following repair with a titanium implant in a patient with prior sinusitis and orbital cellulitis, which resolved after implant removal. 15 However, none of these reports discuss osseous encapsulation of the implant, particularly in the paranasal sinuses.
To our knowledge, no such prior reports have described a pathologic osseous encapsulation of an orbital floor implant. We present the first case description of a chronically-infected orbital floor hybrid titanium-porous polyethylene implant that migrated into the maxillary sinus and became completely embedded in a newly-formed bone.
Case Presentation
This patient is a 68 year-old male with a past medical history of diabetes, hyperlipidemia, and facial trauma resulting in a left orbital floor fracture. He underwent operative repair at an outside hospital with the placement of a titanium and porous polyethylene implant. Several months after the repair, he developed low-grade and chronic inflammation. Then, he underwent an incision and drainage procedure. No operative or procedural records are available from that time.
Six years after the initial repair, the patient developed left eye pain and purulent drainage concerning for hardware infection and presented to our hospital. He was seen and evaluated in the ophthalmology clinic and subsequently underwent an orbitotomy with incision and drainage of an orbital floor abscess. Given the lack of external incision and lower conjunctival scarring, it was presumed that the previous orbital floor repair was carried out via a transconjunctival approach. Despite the incision, drainage for a week, and multiple courses of oral and intravenous antibiotics, the patient experienced only mild and transient improvement. Due to persistent symptoms, there was significant concern for a chronic implant infection (Figure 1A).
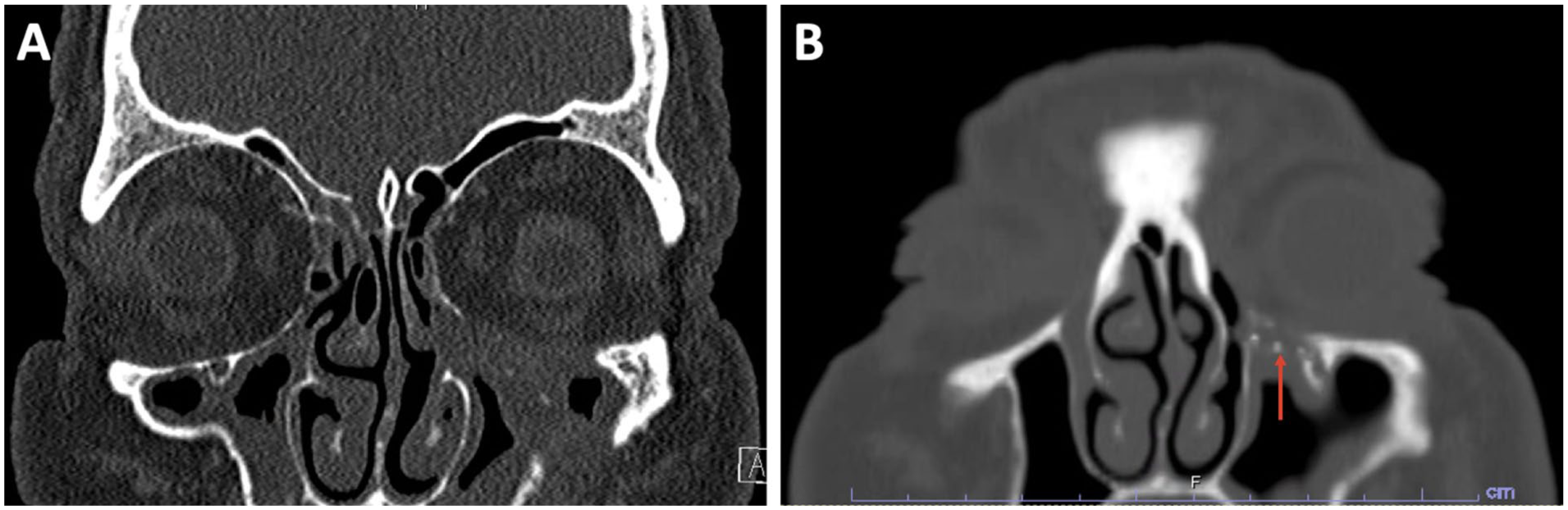
Coronal CT sinus image with left orbital floor implant (A) and after attempted transconjunctival implant retrieval (B). (A) This scan shows exposed orbital floor implant extending into the left maxillary sinus, with associated mucosal thickening and sinus opacification concerning for chronic infection or abscess formation. (B) The scan shows a thin bony layer overlying the left orbital floor implant (indicated by red arrow), which prevented successful retrieval via the transconjunctival approach.
On review of imaging, the medial portion of the implant was noted to not wrap onto the medial orbital wall but rather hang in the superior maxillary sinus. The ophthalmology team then attempted implant removal through a repeat transconjunctival approach. However, upon elevation of the periorbita of the orbital rim and floor, there was no implant noted but only smooth bone (Figure 1B). Consequently, the patient was referred to the otolaryngology – head and neck surgery (OHNS) clinic for further evaluation and consideration of alternative surgical approaches for implant removal.
Approximately 7 months later, the OHNS team brought the patient to the operating room for an attempted implant retrieval. A left-sided endoscopic maxillary mega-antrostomy was performed, which allowed for the visualization of the medial portion of the plate. However, the implant could not be mobilized or fully visualized due to scar and bony overgrowth on the inferior aspect of the implant, suggesting osteogenesis. A concurrent trans-conjunctival approach by ophthalmology was performed, and endoscopic manipulation of the implant allowed a portion of the plate to be seen through a thin fracture line of the new bone that covered the orbital implant. Upon endoscopic incision of the scar tissue along the medial aspect of the orbital floor implant, chronic inflammation and purulent drainage were observed, consistent with a chronically-infected implant.
A left Caldwell-Luc approach was then performed through which the anterior inferior lip on the plate was able to be seen. The thin sheen of bone that had grown along the entire underside of the implant was better appreciated, and the anterior portion was partially removed with Kerrison rongeurs. Through a mixture of elevation and dissection via the trans-nasal endoscopic, transconjunctival, and trans-antral approaches, the implant was able to be successfully retrieved (Figure 2). It was noted to be a composite titanium and polyethylene orbital floor plate; the polyethylene, however, was very smooth and not porous. The patient tolerated the procedure well and was monitored overnight.
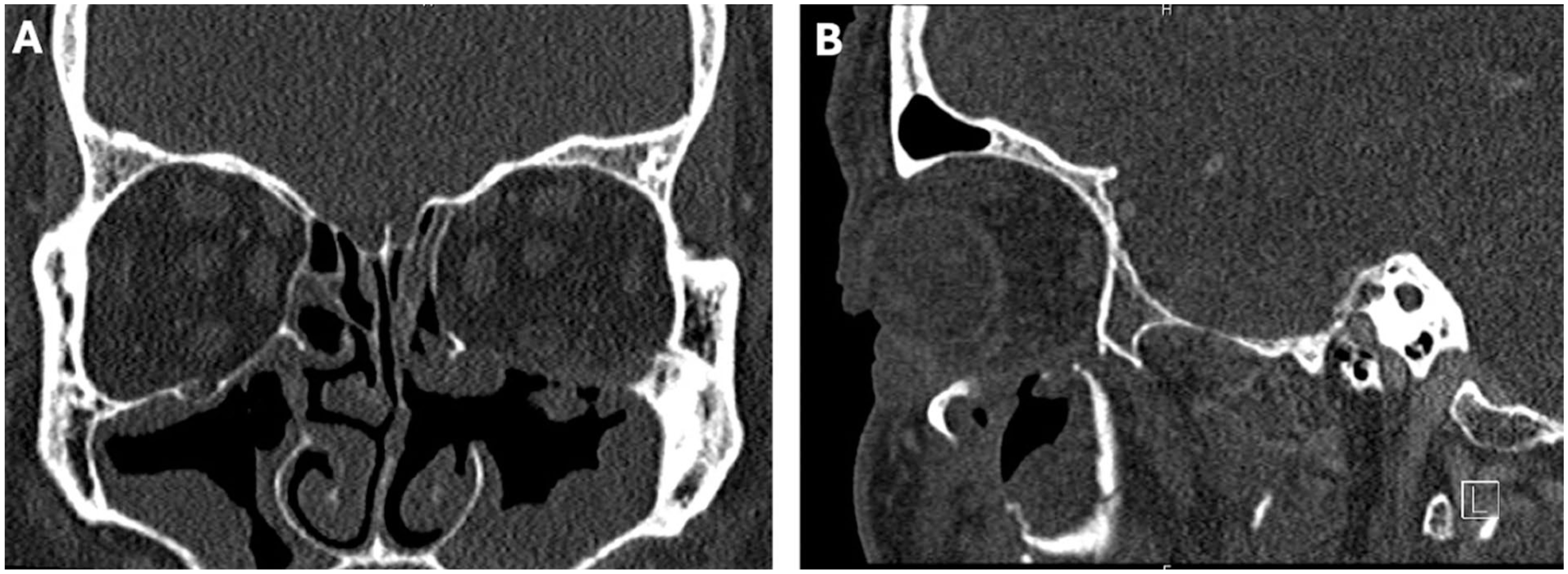
Postoperative coronal (A) and sagittal (B) CT sinus images. (A) Coronal view demonstrates absence of the previously-visible orbital floor implant and reduced maxillary sinus opacification. (B) Sagittal image reveals the Caldwell-Luc antrostomy into the maxillary sinus and resolution of the bony overgrowth previously obstructing the implant. Both views show marked improvement in surrounding inflammation compared with preoperative imaging.
At the patient’s 1 month follow-up, he reported improvement in eye pain and swelling and resolution of the purulent discharge although he endorsed some diplopia, worse with lateral gaze. At his 3 month follow-up, he endorsed resolution of his chronic infection but was continuing care with ophthalmology for his diplopia and vision change.
Discussion
Although postoperative complications for orbital floor implants are well described, complete osteogenesis around an implant is extremely rare. To the best of our knowledge, this is the first case reported in the literature of complete bony encapsulation of a composite titanium-porous polyethylene orbital implant.
While osteogenesis is not an expected outcome from orbital fracture repairs, titanium implants intentionally constructed to osseointegrate are available for the facial skeleton, such as zygomatic/orbital titanium implants for orbit and midface reconstruction, 16 dental implants for dental rehabilitation, and bone anchored hearing aid implants. These implants utilize different techniques, such as sandblasting, to encourage osseointegration between the implant surface and the surrounding bone. Excessive bony overgrowth, in addition to the intended osseointegration, however, has been described in 2 patients in a series of 165 patients who underwent bone anchored hearing aid implantation and required surgical re-exploration at the abutment site. 17 This excessive bone formation was more likely a pathological response at the bone-implant interface beyond the intended osseointegration and therefore suggests that abnormal osteogenesis can arise even when not designed to promote new bone formation.
Given the positioning of the implant on our original computerized tomography scan, the assumption was that the implant was likely inadequately propped onto the medial orbital wall and was floating in the maxillary sinus after which it became chronically infected and ultimately became fully encapsulated with new bone. This unusual outcome points to a prolonged and atypical biological response, likely shaped by a combination of several factors.
One proposed contributor is osteogenic immune activation, an integral aspect of successful osseointegration. After implantation, M1 macrophages induce inflammation, then progresses to the phase with M2 macrophages and regulatory T-cells that decrease inflammation and facilitates bone formation.18,19 However, this process can be disrupted by chronic infection or biofilm formation, which usually lead to persistent activation of M1 macrophages and pro-inflammatory cytokines, and eventually bone resorption. 20 In rare cases, however, chronic low-level immune activation can stimulate a paradoxical response where the body tries to isolate the implant with bone. The term “foreign body equilibrium” has been used to describe this phenomenon, where bone forms as part of a chronic but controlled defense mechanism to encapsulate the implants. 21
In our case, the orbital floor implant was likely placed abnormally into the maxillary sinus during the initial surgery, leaving it exposed to sinus mucosa and flora chronically. Radiographic and operative findings demonstrated a poorly-fixed titanium mesh to the medial orbital wall that was past the sinus cavity (Figure 1A). This orientation may have led to chronic mucosal contact, low-grade irritation, and ongoing infection evidenced by his orbital abscesses and purulent drainage. These factors combined may have induced an immune response characterized by prolonged M2 macrophage activity and, as described above, a slow bone-forming process. Interestingly, there was a study that reported osteogenesis along the sinus walls in patients with zygomatic implants that traversed chronically-inflamed maxillary sinuses. 22 Unlike this study, however, our patient’s implant became fully encased in bone, indicating a more exaggerated response, perhaps due to longstanding duration and the body’s attempt to wall off the foreign substance.
Additionally, mechanical factors could be associated with this immune response. Mechanotransduction is the process by which mechanical stress is transmitted throughout bone, where osteocytes sense strain and induce activation of osteoblasts to form new bone. 23 In this case, the inferior mispositioning of the orbital implant into the maxillary sinus and the lack of fixation to the medial orbital wall may have allowed for recurrent micromovements and low-level stress to the adjacent tissues. The continued effects of these forces may have led to persistent irritation and chronic immune response, resulting in a microenvironment that favored osteogenesis.
Other such factors for an atypical implant osteogenesis, though less likely to have contributed significantly in our patient’s case, are worth discussing as well. As suggested by Thyparampil et al, transient intraocular pressure (IOP) elevations following orbital floor repair can impose mechanical stress, and in theory, promote bone formation. 24 However, our patient’s IOP was not increased at the time of presentation or even after surgery. Moreover, even though most orbital implants are not surface-engineered specifically for osseointegration, titanium in general possesses properties such as surface roughness and hydrophilicity that can modulate the immune response and favor bone healing. 25 While it might not be the main driver of osteogenesis in our case, these properties could have contributed to the more global inflammatory context. What is interesting, however, is that the osteogenesis involved both the titanium and the polyethylene surfaces of the implant. While porous polyethylene typically allows for fibrous ingrowth of tissue, our implant’s polyethylene surface was found to be very smooth with no ingrowth of tissue, only bony encapsulation.
Finally, certain systemic medications have been reported to stimulate osteoblastic activity or to suppress bone resorption, such as teriparatide, simvastatin, vitamin D, via calcium regulation and Wnt/β-catenin signaling. 26 However, at the time of presentation, our patient was not on any medications that are proven to have a major impact on bone metabolism. Overall, these general factors are important to consider when analyzing unusual implant behavior such as ours.
In addition to the unusual pathophysiology, the surgical management in our case was also notable for the unique combination of the transconjunctival, endoscopic, and Caldwell-Luc approaches to access the implant from various angles. There has been one other reported study that used a subciliary and Caldwell-Luc approach for orbital floor fractures, 27 but none that used our technique. Our method can possibly be indicated for challenging and unexpected surgical complications such as our patient. The case demonstrates that multiple approaches may be necessary to use to manage complex orbital implant complications.
Conclusion
In this article, we report a rare case of delayed osteogenesis of a displaced titanium-porous polyethylene orbital floor implant. This case underscores the importance of recognizing atypical tissue reactions, such as an unintentional osseous encapsulation seen in our case, as a differential diagnosis in the setting of late complications following an orbital fracture repair. Definitive management required a combined transconjunctival, trans-antral (Caldwell-Luc), and transnasal approach, emphasizing the role of multidisciplinary and adaptive surgical planning in complex revision cases.
Footnotes
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases or case series.
Consent to Participate
Written informed consent was obtained from the patient to participate.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.