
Abstract
Objectives:
To examine the frequency in which angled endoscopes are necessary to visualize the true maxillary ostium (TMO) following uncinectomy and prior to maxillary antrostomy. Additionally, to identify preoperative computed tomography (CT) measures that predict need for an angled endoscope to visualize the TMO.
Study Design:
Retrospective study.
Setting:
Tertiary academic hospital.
Patients and Methods:
Patients who underwent endoscopic sinus surgery (ESS) between December of 2017 and August of 2018 were retrospectively identified. Cases were reviewed if they were primary ESS cases for chronic rhinosinusitis without polyposis and if they were at least 18 years of age.
Results:
Sixty-three maxillary antrostomies were reviewed (82.5% were from bilateral cases). Thirty-five cases (55.6%) required an angled endoscope in order to visualize the TMO. Of the preoperative CT measures examined, a smaller sphenoid keel-caudal septum-nasolacrimal duct (SK-CS-NL) angle was significantly associated with need for an angled endoscope intraoperatively to visualize the TMO (17.1° SD ± 3.2 vs 15.0° SD ± 2.9; P = .010).
Conclusion:
Angled endoscopes are likely required in the majority of maxillary antrostomies to visualize the TMO. This is important to recognize in order to prevent iatrogenic recirculation. The SK-CS-NL angle may help to identify cases preoperatively which require an angled endoscope to identify the TMO during surgery.
Keywords
Introduction
Seven to nineteen percent of patients who undergo primary endoscopic sinus surgery (ESS) for chronic rhinosinusitis (CRS) will require revision surgery. 1 –5 Endoscopic sinus surgery failure can occur for a variety of reasons including surgical technique, type and extent of sinus disease, underlying systemic diseases or immunodeficiency, and patient compliance with sinonasal medical therapies. When examining factors related to surgical technique, the following are often cited as reasons for ESS failure: retained cells, scarring or adhesions of the middle meatus, ostium narrowing secondary to scarring or osteoneogenesis, middle turbinate lateralization, incomplete uncinectomy, and failure to incorporate the true maxillary ostium (TMO) into the surgical antrostomy. 1,6
When the TMO is not integrated into the antrostomy, a phenomenon known as “recirculation” occurs whereby mucous is extruded from the TMO only to reenter the sinus slightly downstream through the discontinuous surgical antrostomy, effectively creating a functional obstruction. Maxillary sinus recirculation has been identified in up to 15% of cases at the time of revision surgery. 7 However, removal of the intervening bridge of tissue between the TMO and surgical antrostomy in order to restore physiologic drainage can be easily performed by in-office lysis under local anesthesia, with likely resolution of symptoms caused by recirculation. 8
Visualizing the TMO during surgery is critical in order to prevent recirculation. It cannot be identified without complete uncinectomy and may be challenging to identify as it is situated anterosuperiorly on the medial maxillary wall, lateral and deep to the nasolacrimal convexity. 9 Anecdotally, the TMO often cannot be visualized with a 0° endoscope, necessitating use of an angled endoscope (typically a 30° or 45°; Figure 1). To our knowledge, there is no published study to date that has examined how frequently an angled endoscope is required during ESS to visualize the TMO. Therefore, in this study, we examine: (1) the proportion of maxillary antrostomies performed for CRS without nasal polyposis (CRSsNP) that require an angled endoscope to visualize the TMO following uncinectomy and (2) preoperative computed tomography (CT) measures that may predict need for an angled endoscope to visualize the TMO during surgery.
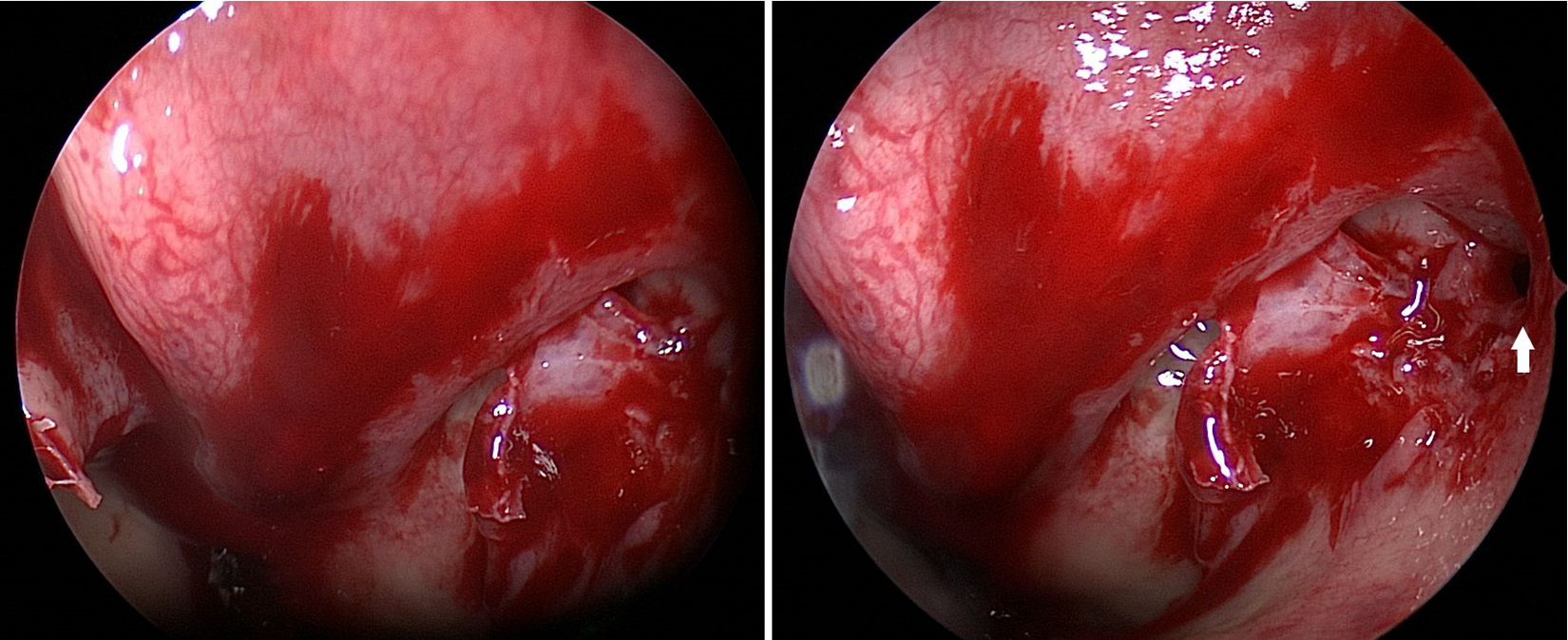
Visualization of the true maxillary ostium (TMO) with both 0° (left) and 30° (right) endoscopes. The arrow denotes the TMO. The TMO in this case could only be visualized with an angled endoscope.
Methods
Institutional review board approval was obtained prior to commencement of this study. Patients who underwent ESS from December 2017 to August of 2018 were retrospectively reviewed if they met the following inclusion criteria: had CRSsNP, underwent primary surgery, and were at least 18 years of age. All patients underwent surgery with one of 2 rhinologists in the Department of Otolaryngology–Head and Neck Surgery at New York University (R.A.L. and S.M.L).
True Maxillary Ostium Identification
After uncinectomy and prior to maxillary antrostomy, close inspection of the TMO was performed. One rhinologist (R.A.L) used a 0° endoscope for initial attempt at visualizing the TMO, while the other rhinologist (S.M.L) used a 30°. If the TMO was not able to be visualized by R.A.L. with a 0° endoscope, further attempt was made with an angled endoscope (first with a 30° or if necessary, a 45°). After visualizing the TMO with a 30° endoscope, S.M.L. attempted visualization with a 0° endoscope. Whether or not an angled endoscope was necessary to visualize the TMO was recorded for each case. Visualization of the TMO was defined as identification of at least the posterior membranous aspect of the ostium.
Preoperative Radiographic Measurements
In consultation with a neuroradiologist (E.Z.) at our institution, 4 preoperative CT measures were devised a priori that were thought to be possibly predictive of difficulty visualizing the TMO with a 0° endoscope during surgery. (1) Lund-Mackay score—an index of mucosal inflammation that can lead to obscuration of the TMO, was calculated for the side (left or right) that the maxillary antrostomy was performed. (2) Piriform aperture width—a narrower nasal corridor will limit positioning of the endoscope laterally and thus visualizing the TMO. This was recorded at its widest width in the coronal plane. (3) Ostium depth—calculated by measuring the distance between a line parallel to the plane of the TMO or medial maxillary wall and a line tangent to the medial aspect of the nasolacrimal duct and parallel to the plane of the TMO or medial maxillary wall. This distance represents how lateral lying or deep the TMO is relative to the convexity of the nasolacrimal duct (Figure 2). (4) Sphenoid keel-caudal septum- nasolacrimal duct (SK-CS-NL) angle—this is the angle between a line drawn from the caudal most aspect of nasal septum to the sphenoid keel (a consistent midline structure) and a line from the caudal septum running tangent to the medial aspect of the nasolacrimal duct (Figure 3). This angle is thought to represent the viewing angle of the nasal corridor when a 0° endoscope is seated at the vestibule. Two of the study’s authors (O.H.A. and M.P.L) independently measured Lund-Mackay score, piriform aperture width, and SK-CS-NL angle, for all subjects. Our study’s neuroradiologist (E.Z.) calculated ostium depth.

Ostium depth.

Sphenoid keel- caudal septum- nasolacrimal duct (SK-CS-NL) angle.
Statistical Analysis
Descriptive statistics were performed for preoperative CT measures. The CT measures were compared between type of endoscope required (angled vs zero degree) by Wilcoxon rank sum test. Additionally, a linear mixed effects model was applied to quantify the associations between type of endoscope required and CT measures by taking the intra-subject correlation between sides (left and right) if bilateral surgery was performed. For inter-rater reliability, the intraclass correlation (ICC) was calculated for each CT measure except ostium depth as this was measured only by our neuroradiologist. An ICC > 0.75 is thought to suggest good inter-rater agreement. All analyses were done with SAS 9.4 (SAS Institute Inc., Cary, NC). A two-sided p-value of <0.05 was considered to be statistically significant.
Results
A total of 63 maxillary antrostomies were examined (Table 1). The majority (82.5%) of antrostomies were from cases performed bilaterally. Most cases (55.6%) required an angled endoscope to successfully identify the TMO. All TMOs in this series were successfully identified and none required greater than a 45° endoscope. Intraclass correlation coefficient measuring inter-rater agreement, was greater than 0.75 for each CT measure (except ostium depth as this was calculated alone by author E.Z.). When examining the relationship between pre-operative CT measures and need for an angled endoscope to visualize the TMO during surgery, only the SK-CS-NL angle was a significant predictor (Table 2). The SK-CS-NL angle was significantly larger on average in cases where a 0° degree endoscope was adequate to visualize the TMO (17.1°; SD: ±3.2 vs 15.0° SD± 2.9; p = 0.010). Ostium depth, piriform aperture width, and Lund-Mackay scores, were not significantly associated with type of endoscope required to visualize the TMO.
Case Information.
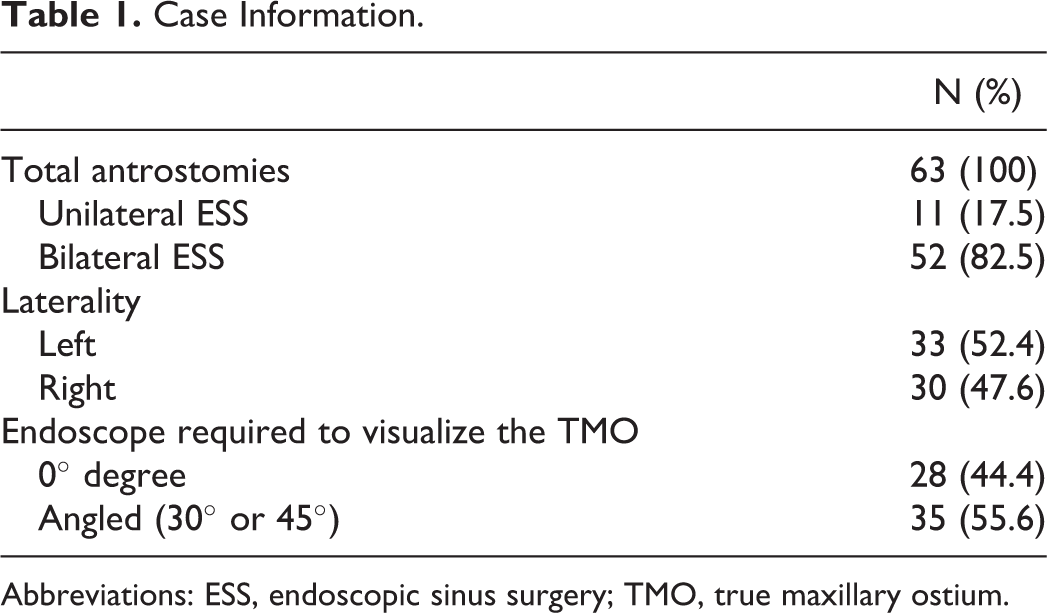
Abbreviations: ESS, endoscopic sinus surgery; TMO, true maxillary ostium.
Preoperative CT Measures as Predictors of Requiring an Angled Endoscope to Visualize the TMO During ESS.a
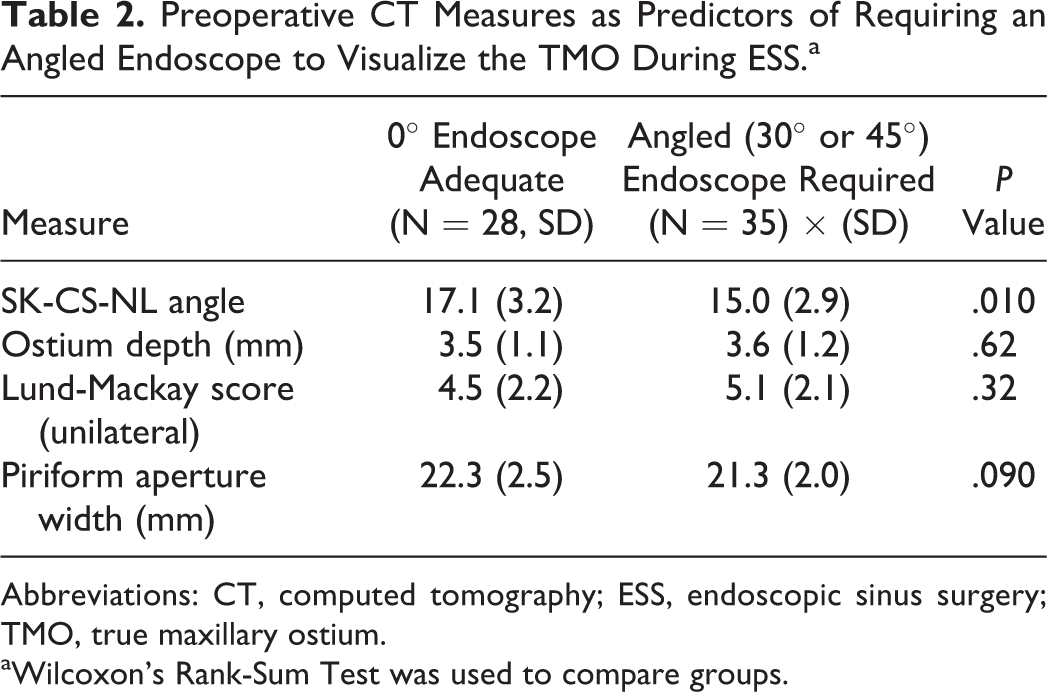
Abbreviations: CT, computed tomography; ESS, endoscopic sinus surgery; TMO, true maxillary ostium.
aWilcoxon’s Rank-Sum Test was used to compare groups.
Discussion
Chronic rhinosinusitis affects approximately 1 in 7 adults and is one of the most common reasons for outpatient physician visits. 10,11 In turn, ESS is increasingly one of the most commonly performed outpatient surgeries in the United States. 11,12 While sinus surgery is successful for most patients, a not insignificant proportion of patients will undergo revision. Maxillary sinus recirculation remains a commonly identified reason for failure during revision surgery. 7,13 Maxillary antrostomy, while seemingly simple, can be difficult to perform properly as there are few landmarks to assist in identification of the maxillary ostium compared to surgery of the sphenoid and ethmoid sinuses where a multitude of landmarks are available (i.e. skull base, lamina papyracea, superior turbinate, maxillary roof, etc.). 14
To our knowledge, this is the first study to examine how frequently an angled endoscope is required to visualize the TMO during maxillary antrostomy. This is important to consider in order to prevent recirculation, a recognized iatrogenic cause of persistent rhinosinusitis. The results of our study suggest that an angled endoscope is likely required in the majority (55.6%) of maxillary antrostomies in order to visualize the TMO. Some practitioners may predominantly rely on a 0° endoscope to perform maxillary antrostomy; however, this could preclude visualization of the TMO and thus incorporation of it into the antrostomy. In this study, we also examined a radiographic measure that we have labeled the SK-CS-NL angle. This measure represents the endoscopic angle of viewing from the vestibule, particularly the lateral limit where visualization beyond and around the nasolacrimal duct is required to visualize the TMO. This angle may be affected by anatomical differences in the septum, width of the nasal cavity, prominence of the nasolacrimal duct, and how lateral lying or deep the TMO is. In cases where an angled endoscope was required to visualize the TMO, this angle was significantly less than when a 0° degree endoscope was adequate (17.1° vs 15.0°; P = .010). However, while statistically significant, the clinical significance of this is uncertain and requires further validation.
There are limitations to this study that warrant discussion. Our small study sample size limits the statistical power and conclusions drawn. Additionally, our study includes cases performed by 2 rhinologists who differ in their surgical technique. This may have led to differences in visualizing the TMO or the threshold in which it was identified. Furthermore, resident physician involvement in this series was not captured but was likely quite variable.
Footnotes
Authors’ Note
Presented as an oral presentation at the American Academy of Otolaryngology- Head and Neck Surgery Foundation (AAO-HNSF) Annual Meeting & OTO Experience on October 8th, 2018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.