
Abstract
Iatrogenic displacement of third molars is a rare but significant complication of dental extractions, particularly in children where unique anatomic and developmental factors pose additional challenges. This report describes the case of a 12-year-old female who presented with a displaced maxillary third molar crown into the left maxillary sinus following dental extraction. This displacement resulted in acute orbital cellulitis, which was initially managed with oral antibiotic therapy. Endoscopic endonasal retrieval of the foreign body 4 months later was recommended after the initial infection was treated to reduce the risk of recurrent orbital and/or sinonasal infections. Surgical planning incorporated intraoperative navigation with existing cone beam computed tomography to minimize radiation exposure. The procedure was successful with no perioperative complications. This case highlights the importance of prompt recognition, careful surgical planning, and utilization of minimally invasive approaches to optimize outcomes while minimizing craniofacial morbidity in pediatric patients.
Introduction
Third molars, colloquially known as wisdom teeth due to their late eruption, are the most frequently targeted teeth for extraction. 1 Classic indications for dental extraction include impaction or infection, particularly in young adults. Despite it being a routine dental procedure performed on approximately 5 million Americans each year, third molar extraction is not devoid of complications. 2 Pain, edema, infection, and self-limited bleeding are relatively common and benign complications of wisdom tooth extraction. 3 However, severe complications such as nerve injury, oronasal fistulae, mandibular fractures, and tooth displacement are also possible adverse events. 4 It is crucial for clinicians to recognize and manage these complications promptly to minimize the risk of long-term morbidity and ensure optimal patient outcomes. Iatrogenic tooth displacement into adjacent anatomical spaces, including the lateral pharyngeal space, infratemporal fossa, maxillary sinus, and buccal space, can lead to infection if not treated or addressed in a timely manner. Although such cases have been reported, these descriptions have been limited to the adult population.5 -8 Specifically, pediatric patients present unique challenges due to reduced craniofacial dimensions and developing dentition, which necessitate careful planning and unique technical considerations. 9 This work describes a step-by-step endoscopic endonasal approach for the retrieval of a displaced maxillary third molar crown in a prepubescent patient.
Case Presentation
A 12-year-old female underwent wisdom tooth extraction due to impacted third molars. During dental extraction, the oral surgeon observed displacement of the left molar crown. Panorex imaging intraoperatively revealed that the tooth was displaced within the ipsilateral maxillary sinus, and multiple attempts at transoral removal were unsuccessful. Three days afterwards, she developed an acute episode of orbital cellulitis, which was initially managed with a course of outpatient oral antibiotic therapy. The patient’s past medical history was notable for seasonal allergies and recurrent sinusitis. After the patient worsened 2 weeks later, the patient was referred to Otolaryngology and started on intravenous antibiotics, which treated her appropriately. Nasal endoscopy was performed, which revealed no acute sinonasal infection but was notable for bilateral concha bullosa, inferior turbinate hypertrophy, and adenoid hypertrophy. Functional endoscopic sinus surgery was recommended 4 months post-dental extraction after improvement from the initial infection not only for foreign body removal but also to address chronic nasal obstruction. Cone beam computed tomography (CT) imaging at this time revealed a calcified foreign body in the left maxillary sinus and post-obstructive inflammatory changes within the ethmoid labyrinth (Figure 1).
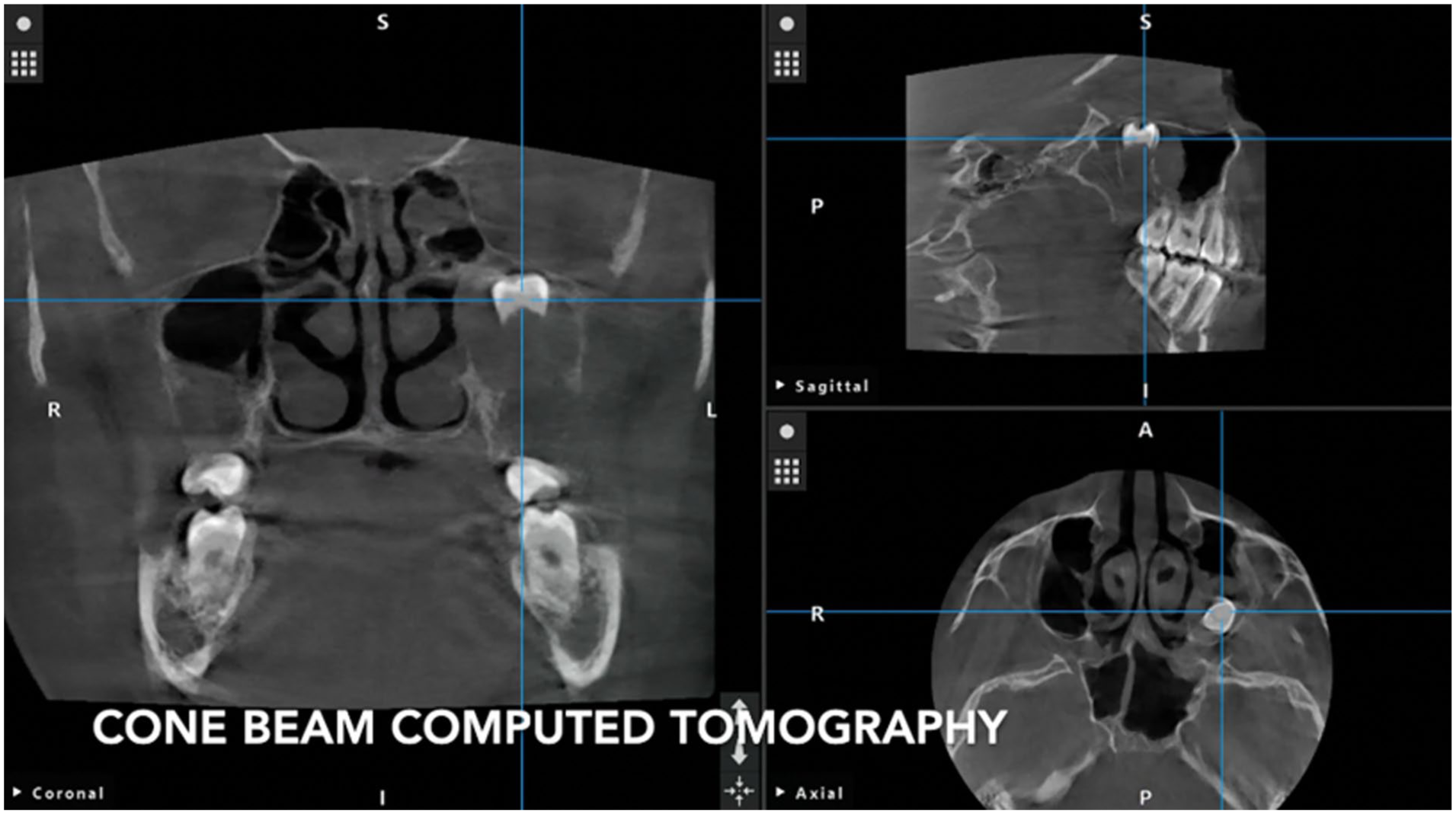
Tri-planar cone beam computed tomography imaging reveals a calcified foreign body in the left maxillary sinus (Stryker ENT Navigation System).
Surgical Technique
The procedure was performed under general anesthesia. Stryker ENT navigation system (Stryker Corportion, Kalamazoo, MI, USA) was utilized for image guidance during the surgery. A 4 mm 0° endoscope was used to examine the left and right sinonasal cavities. 1% lidocaine with 1:100 000 epinephrine was injected into the left uncinate process, and bilateral inferior and middle turbinates.
A 15-blade was used to make a stab incision along the face of the concha bullosa on the left side. The left concha bullosa was resected using straight thru-cut forceps and a microdebrider. An uncinectomy was carried out using backbiting forceps. The posterior fontanelle of the maxillary sinus was resected using straight thru-cut forceps to create a mega antrostomy. After achieving adequate exposure, a 4 mm 70° endoscope was used to examine the left maxillary sinus where a foreign body was evident along the posterior maxillary wall (Figure 2).
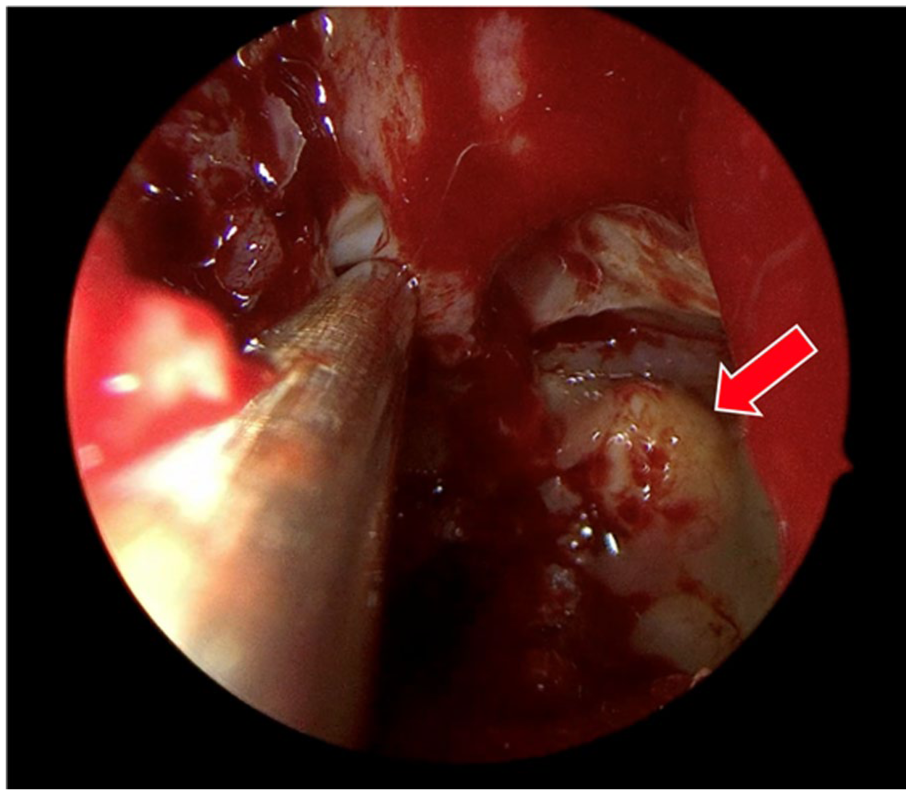
A foreign body (arrow) was identified adhered along the posterior maxillary wall of the left maxillary sinus.
Takahashi forceps were used to carefully remove the foreign body and a Cottle elevator was used to debride osteitic bone along the posterior maxillary wall where the foreign body had been adhered (Figure 3). Finally, bilateral submucous inferior turbinate reduction, transoral microdebrider adenoidectomy, and right concha bullosa resection were performed in a standard manner. The patient did well after surgery and did not experience any perioperative complications.
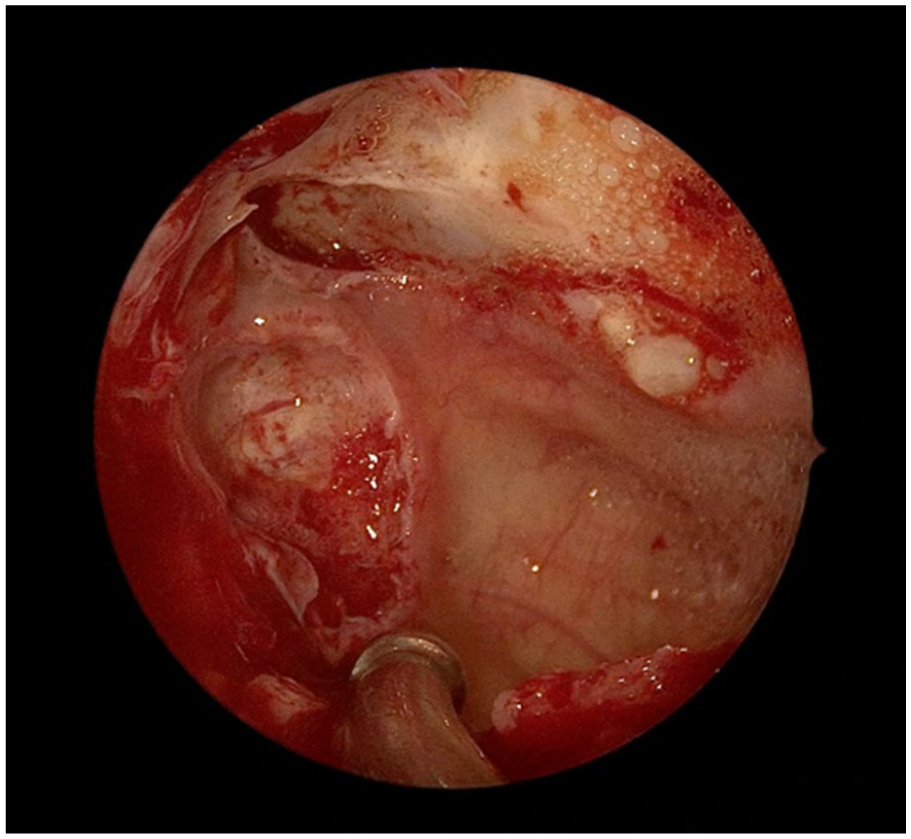
Left posterior maxillary sinus wall following foreign body removal showing bony transformation where the foreign body had been adhered.
Postoperative Outcome
Follow-up nasal endoscopy with in-office nasal debridement 12 months after surgery revealed a patent left maxillary antrostomy and resolution of nasal obstructive symptoms. Pathological analysis of the foreign body was consistent with a molar tooth.
Discussion
This work presents an endoscopic endonasal approach for the retrieval of a displaced maxillary third molar crown in a prepubescent patient. The patient presented with iatrogenic third molar displacement into the maxillary sinus during dental extraction. The patient was successfully managed with a combination of oral antibiotic therapy for acute orbital cellulitis and prompt endoscopic endonasal removal of the foreign body. The patient recovered uneventfully and remained free of complications at her 12-month follow-up visit.
In this case, foreign body removal was recommended to address concerns surrounding the displaced tooth serving as a potential nidus for recurrent sinonasal infections and chronic inflammation. Several studies have described that retained foreign bodies in the paranasal sinuses can serve as a nidus for infection, leading to sinusitis, abscess formation, and potential spread of infection into the surrounding orbital and intracranial compartments.10,11 Additionally, chronic foreign bodies can also lead to persistent inflammation, resulting in mucosal damage and an increased risk of chronic rhinosinusitis. 12 Finally, traumatic teeth displacement can further increase these risks as it may compromise the dental pulp and create pathways for opportunistic bacteria to enter and colonize, leading to abscess formation.13,14
Another unique feature of this case is the patient’s young age. Although third molars tend to fully erupt in young adults at a median age of 20 years, the patient’s prepubescent age, in this case, highlighted various special considerations for adequate management in this age group. 15 First, every effort was made to minimize unnecessary radiation exposure. Novel intraoperative surgical navigation technology allowed utilization of the original dental cone beam CT scan to be used for intraoperative surgical navigation, obviating the need for additional scans and minimizing additional radiation exposure. Second, achieving adequate exposure while minimizing potential craniofacial morbidity dictated approach selection. In this case, a purely endoscopic endonasal approach with the creation of a maxillary mega antrostomy provided adequate visualization while minimizing potential dental sensory disturbances and damage to developing permanent dentition in a prepubescent patient. 16 While the Caldwell-Luc approach can be a valuable tool in the surgeon’s armamentarium for removing antral foreign bodies, its drawbacks, including the risk of infraorbital nerve or nasolacrimal duct injury, make it a less preferred option compared to minimally invasive approaches in children.17 -19 Finally, this work demonstrates how a minimally invasive approach and tailored imaging protocols can optimize outcomes and meet the special surgical, rehabilitative, and developmental needs of children. 9 These basic principles can also be applied to similar cases involving foreign bodies in challenging anatomic locations.
Conclusion
Iatrogenic tooth displacement is a rare but potentially serious complication following wisdom tooth extraction. Prompt recognition and management of this condition is crucial to avoid infectious and inflammatory complications related to chronically retained foreign bodies. This case highlights the importance of adequate approach selection to maximize exposure while minimizing craniofacial morbidity in the pediatric population. Additionally, this case emphasizes the importance of selective imaging studies to minimize radiation exposure in children. Ultimately, prompt diagnosis and intervention employing a minimally invasive approach are paramount in managing this complex condition.
Footnotes
Author Note
This manuscript was presented as a podium presentation at the 2024 Eerie ENT Cases on October 26, 2024.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent Statement
Written informed consent was obtained from the patient and their legal guardian for the publication of this case report.
Author Contributions
All authors (B.A.V.-S., V.B.H., S.C.L., V.A.P.) reviewed the case, contributed to writing and editing the manuscript, and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Submission Statement
This article is original and has not been submitted elsewhere in part or in whole.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.