
Abstract
Keywords
Introduction
Conventional inferior meatal antrostomy (IMA) was first suggested circa 1887 and was a common procedural approach to various maxillary diseases. 1 It provides good insights and excellent access to the maxillary sinus in a safe and relatively easy manner. 2 However, it does not improve the natural and physiological drainage of the sinus and can lead to disruption of the mucocilliary transport of the mucus. 3 It was abandoned after Messerklinger introduced the concept of the natural ostium. 4 This discovery was the shifting point for sinus surgery, when the endoscopic era began in the 1980s.
Because endoscopic middle meatal antrostomy (MMA) is considered a minimally invasive and functional procedure, it is currently the main approach and the standard of care in addressing various maxillary sinus pathologies. 5 The aim of such a procedure is to optimize ventilation and drainage of the sinus and to provide access to address the underlying disease without disturbing the mucocilliary flow. 3
However, endoscopic MMA frequently offers only limited exposure of the full range of the maxillary sinus. Hidden niches, such as the alveolar, zygomatic, and prelacrimal recesses, serve as distinguishing features of the individual maxillary sinus anatomy. 1,6 In these difficult-to-access locations, endoscopic MMA alone would not allow for sufficient access and could increase the risk of leaving residual disease.
Therefore, for anatomically challenging maxillary lesions, a combined approach using endoscopic inferior and middle meatal antrostomies has been suggested. This combined approach would yield both intraoperative and postoperative benefits. 7 However, this approach is known to increase the risk of recirculation, a phenomenon in which mucus recirculates between adjacent openings back into the maxillary sinus. It can lead to the recurrence of the disease and/or persistent postnasal drip. 8
In this paper, we introduce our modified technique of inferior antrostomy as a submucosal temporary inferior maxillary antrostomy (STIMA). In cases in which a combined approach is required, it would improve intraoperative visualization and accessibility to various locations of the maxillary sinus and reduce the occurrence of the known complications of conventional inferior maxillary antrostomy, such as recirculation phenomenon, persistent postnasal drip, and injury to the nasolacrimal duct (NLD).
Objectives
To describe our new modification of the conventional inferior maxillary antrostomy, STIMA.
To compare the degree of visualization between the MMA and our new modification (STIMA).
To compare the ease of accessibility between the MMA and our new modification (STIMA).
To assess the integrity of the flap and its adequacy in closing the inferior maxillary antrostomy.
Methodology
This was a descriptive cadaveric study. It was performed at the experimental animal laboratory of the Faculty of Medicine at an academic teaching hospital. The study was approved by the institutional review board.
Study Specimen
The study was performed on 4 fresh frozen human cadavers. Eight maxillary sinuses were used to achieve the study objectives.
The maxillary sinus was divided into 5 areas: roof, posterior wall, prelacrimal recess, zygomatic recess, and alveolar recess.
For Visualization
For the degree of visualization, 3 different rigid sinonasal endoscopes were used. The endoscopes (Karl Storz, Tuttlingen, Germany) were 4 mm × 17 mm, in size with 0, 30, and 70-degree views. Each area of the maxillary sinus was assessed by the 3 different scopes, once through the MMA and once through the IMA. The degree of visualization was classified and scored as completely visualized (1 point), partially visualized (1/2 point), or non-visualized (0 point).
For Accessibility
For ease of accessibility, straight, and curved rigid suction tubes were used. The straight suction tube (FERGUSON Suction Tube) had a cut-off hole, 10 Fr., and a working length of 11 cm. The curved suction cannula (V. EICKEN Antrum Cannula, LUER-Lock), had a long curved outer diameter of 3 mm and a length of 15 cm. Each area of the maxillary sinus was assessed by the 2 different suction tubes, once through the MMA and once through the IMA. Ease of accessibility was classified and scored as completely accessible (1 point), partially accessible (1/2 point), or non-accessible (0 point).
Surgical Technique
Middle Meatal Antrostomy
The vertical and horizontal parts of the uncinate process were completely removed using the retrograde swinging-door technique to ensure visualization of the natural ostium and the creation of a very wide antrostomy. An antrostomy was extended posteriorly to the level of the posterior maxillary wall.
This was performed using a combination of maxillary probes, back-biting forceps, ethmoid forceps, and microdebrider shaver blades.
Submucosal Temporary Inferior Maxillary Antrostomy
An initial incision was made on the lateral wall, just anterior and inferior to the face of inferior turbinate. This was then extended medially toward the septum and extended posteriorly at the junction between the nasal septum and the nasal floor over the hard palate. A submucosal flap was raised from the nasal floor and the lateral wall of the inferior meatus. The distal end of the NLD near Hanser’s valve were secured, as they were raised with the flap. An inferior maxillary antrostomy was created by removing the bony wall and the corresponding maxillary mucosa. This was performed using the J-curette, curved suction, back-biting forceps, ethmoid forceps, and different microdebrider blades. After the end of the study, the flap was redraped to cover and close the inferior maxillary antrostomy. The flap was assessed for its integrity and adequacy of closure (Figure 1).
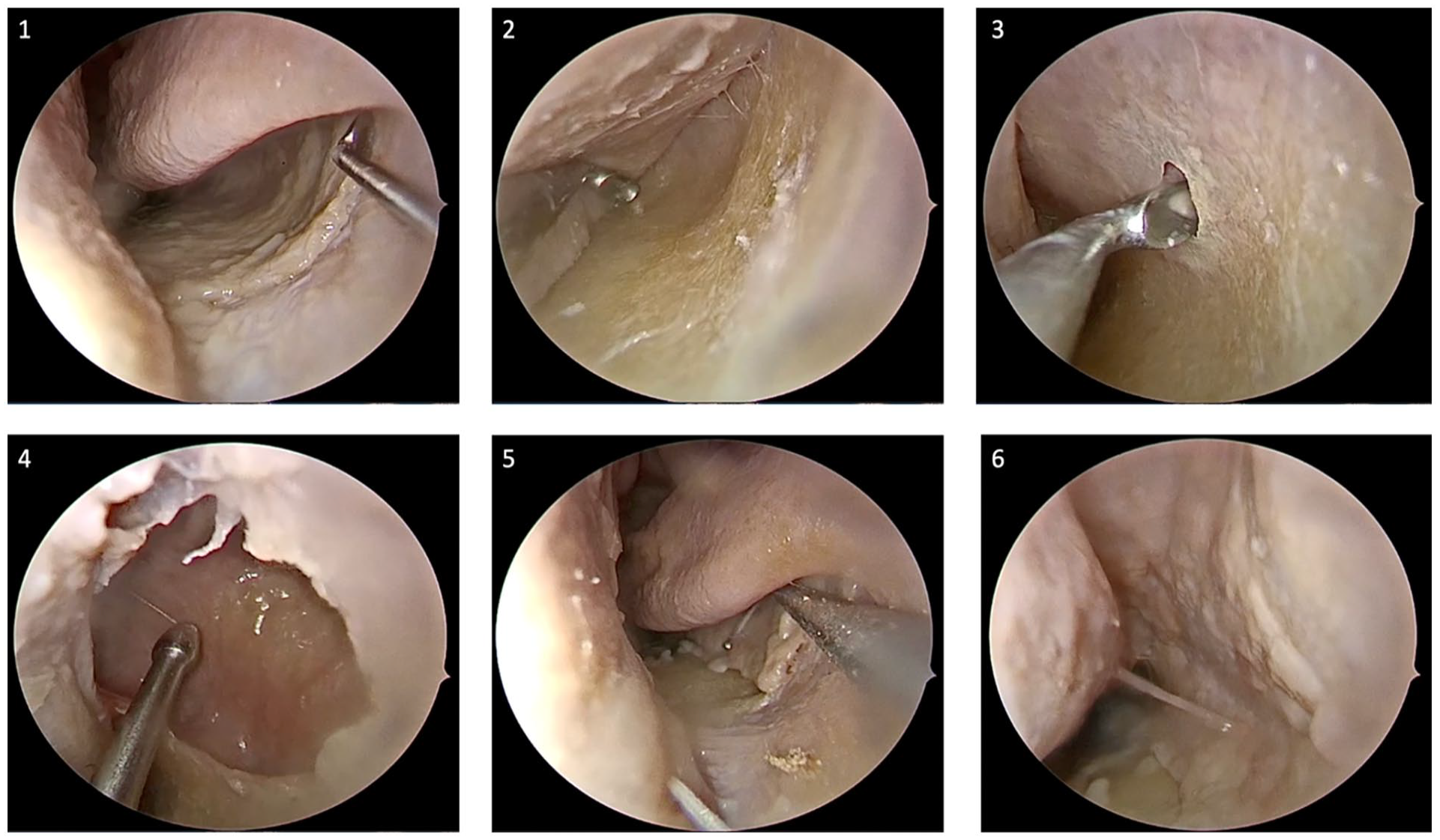
STIMA technique: (1) Site of incision. (2) Submucoasal flap. (3) Submucosal antrostomy. (4) After widening the submucosal antrostomy. (5) After draping the mucosa. (6) End of procedure.
Statistical Analysis
IBM SPSS® Version 23 (IBM Corp., Armonk, NY, USA) was used for the statistical analyses. Categorical and nominal data were summarized as counts and percentages, while continuous data were summarized as means and standard deviations. A paired sample t-test was used to establish the relationships between the 2 groups. Lastly, conventional P-values of <.05 were used to reject the null hypothesis.
Results
The proposed modification of the IMA was performed on 4 cadaveric cephalic specimens. All the eight sides were utilized to achieve the study objectives.
Regarding the degree of visualization, our study demonstrated the superiority of STIMA over MMA, especially in the hidden niches of the maxillary sinus. The difference in the visualization scores of these niches using just the 0-degree rigid endoscope was statistically significant. Using the 30-degree rigid endoscope improved the visualization of these areas; however, it was still better through the STIMA (P-value was significant, <.05). With the 70-degree rigid endoscope, the visualization of the zygomatic recess and roof was complete through the MMA on all 8 sides (Figures 2 and 3). However, the visualization of the prelacrimal and alveolar recesses were better through the STIMA (P-value was significant, <.05) (see Tables 1 –3).
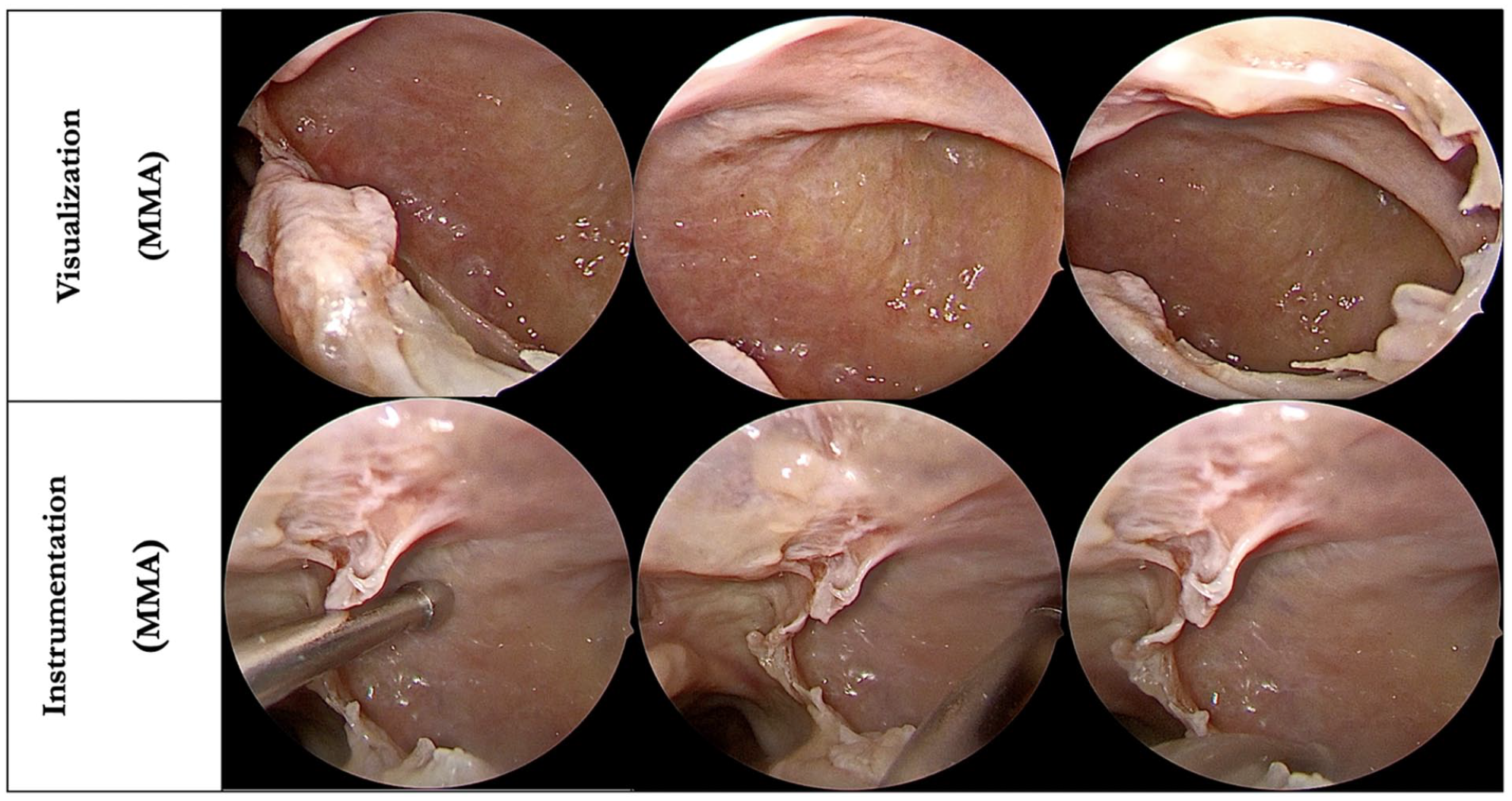
Demonstrating visualization and instrumentation through middle meatal antrostomy.
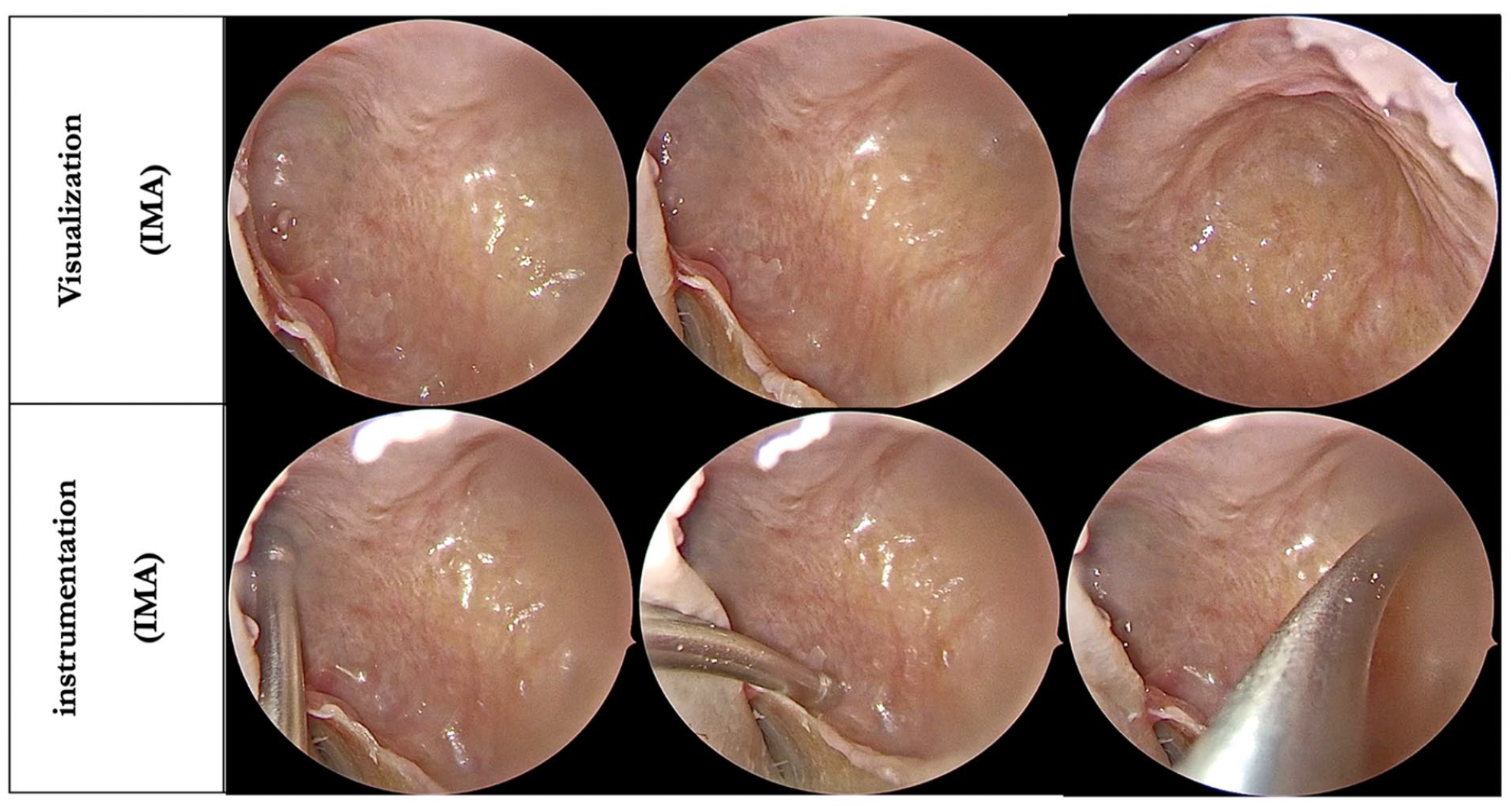
Demonstrating visualization and instrumentation through inferior meatal antrostomy.
Showing Mean Score of Visualization for Each Maxillary Area Using 0-Degree Scope.
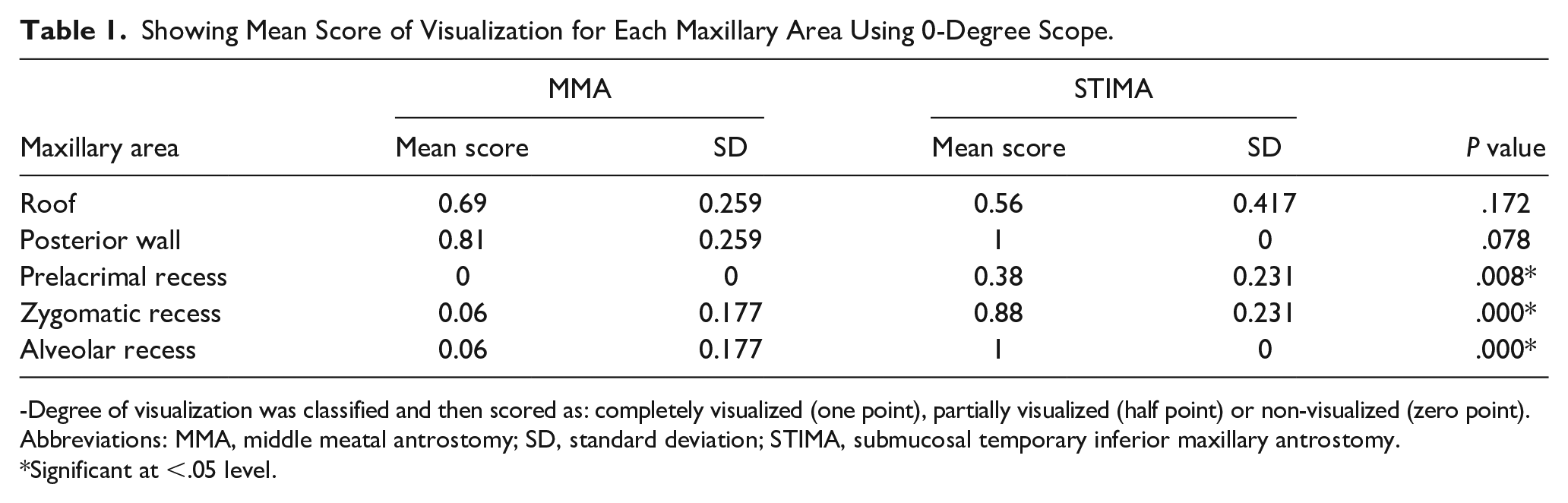
-Degree of visualization was classified and then scored as: completely visualized (one point), partially visualized (half point) or non-visualized (zero point).
Abbreviations: MMA, middle meatal antrostomy; SD, standard deviation; STIMA, submucosal temporary inferior maxillary antrostomy.
Significant at <.05 level.
Showing Mean Score of Visualization for Each Maxillary Area Using 30-Degree Scope.
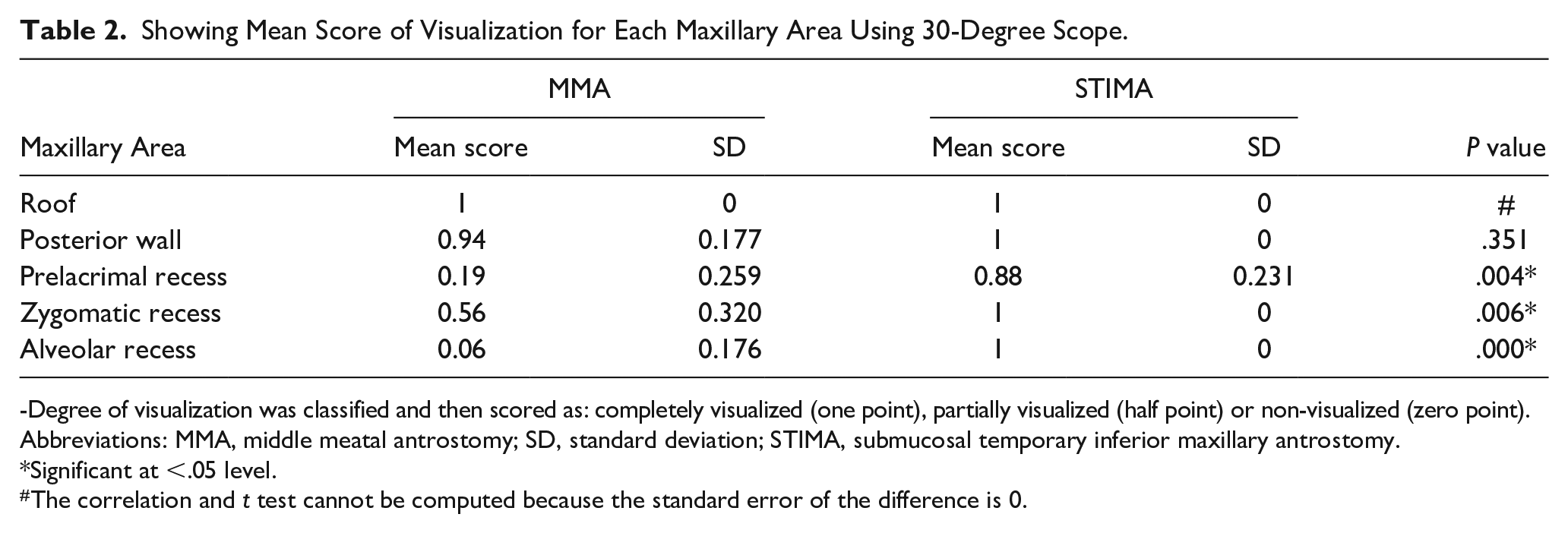
-Degree of visualization was classified and then scored as: completely visualized (one point), partially visualized (half point) or non-visualized (zero point).
Abbreviations: MMA, middle meatal antrostomy; SD, standard deviation; STIMA, submucosal temporary inferior maxillary antrostomy.
Significant at <.05 level.
The correlation and t test cannot be computed because the standard error of the difference is 0.
Showing Mean Score of Visualization for Each Maxillary Area Using 70-Degree Scope.
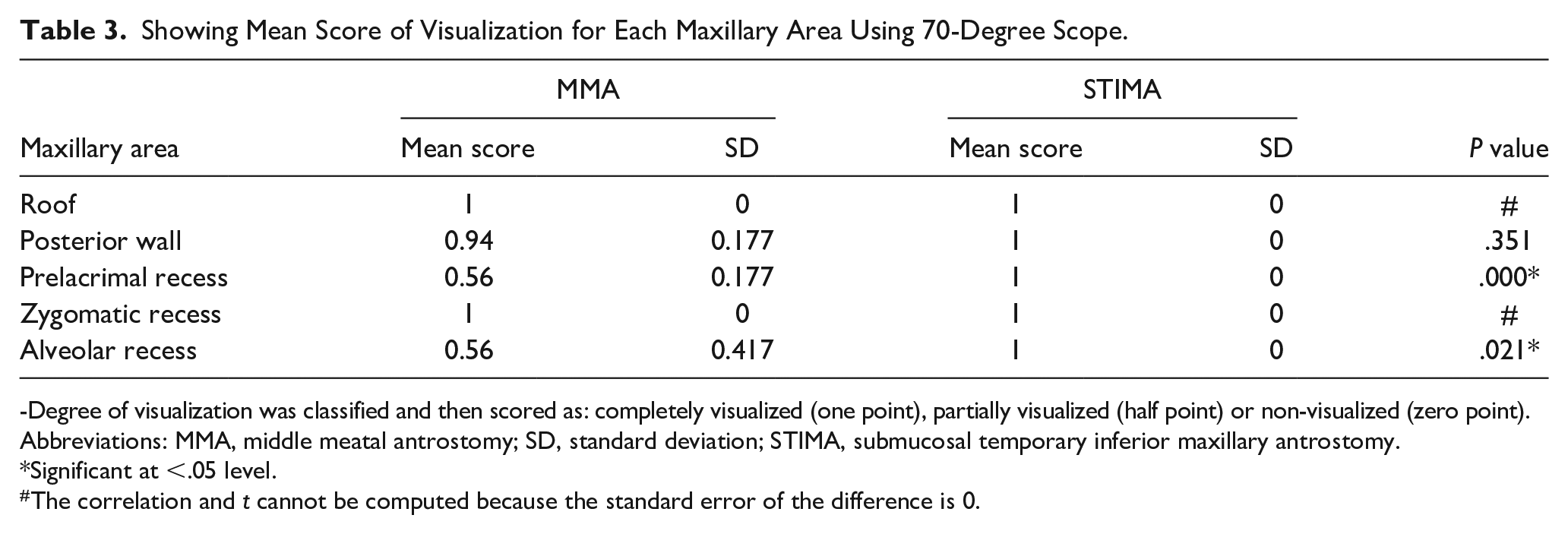
-Degree of visualization was classified and then scored as: completely visualized (one point), partially visualized (half point) or non-visualized (zero point).
Abbreviations: MMA, middle meatal antrostomy; SD, standard deviation; STIMA, submucosal temporary inferior maxillary antrostomy.
Significant at <.05 level.
The correlation and t cannot be computed because the standard error of the difference is 0.
When we evaluated the ease of instrumentation using the straight suction, the roof was better accessed through the MMA. Access to the prelacrimal recess was limited through both approaches. However, access to the posterior wall, the alveolar recess, and the zygomatic recess was better through the STIMA (P-value was significant, <.05). Using the curved suction cannula, the roof and the posterior wall were completely accessible through both approaches on all 8 sides. However, in the difficult-to-access locations, such as the prelacrimal recess, alveolar recess, and zygomatic recess, access through the MMA was very limited (Figures 2 and 3). In contrast, these locations were completely accessible on all 8 sides through our proposed STIMA (P-value was significant, <.05) (see Tables 4 and 5)
Showing Mean Score of Accessibility for Each Maxillary Area with Straight Suction.
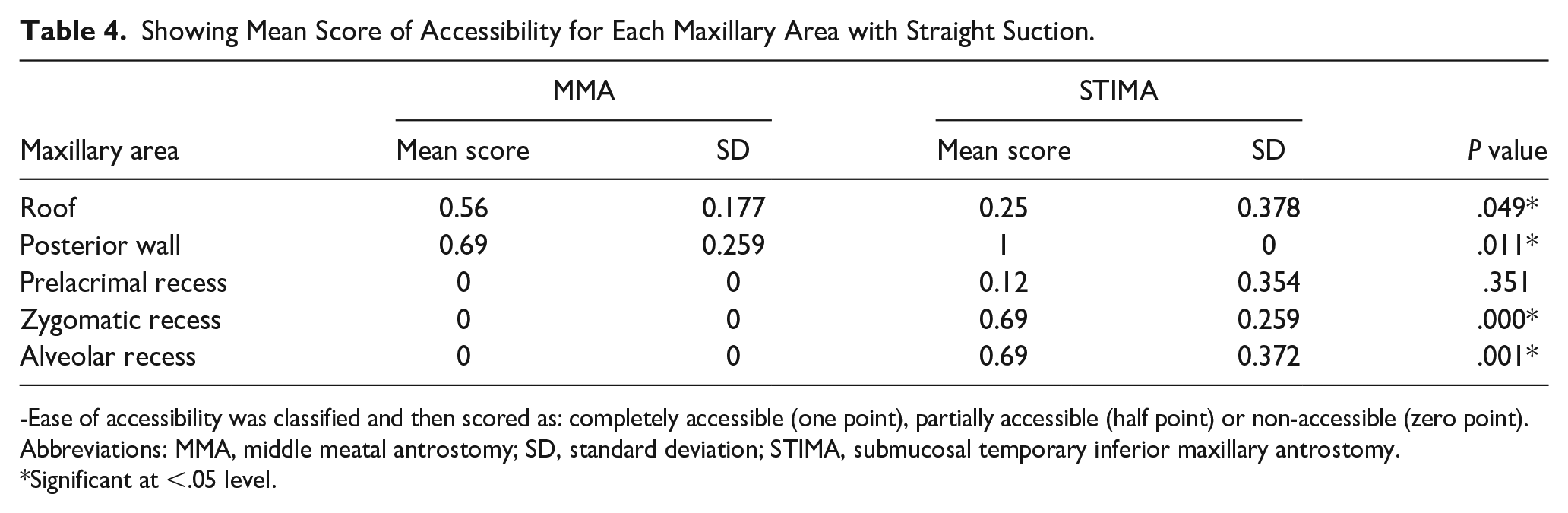
-Ease of accessibility was classified and then scored as: completely accessible (one point), partially accessible (half point) or non-accessible (zero point).
Abbreviations: MMA, middle meatal antrostomy; SD, standard deviation; STIMA, submucosal temporary inferior maxillary antrostomy.
Significant at <.05 level.
Showing Mean Score of Accessibility for Each Maxillary Area with Curve Suction.
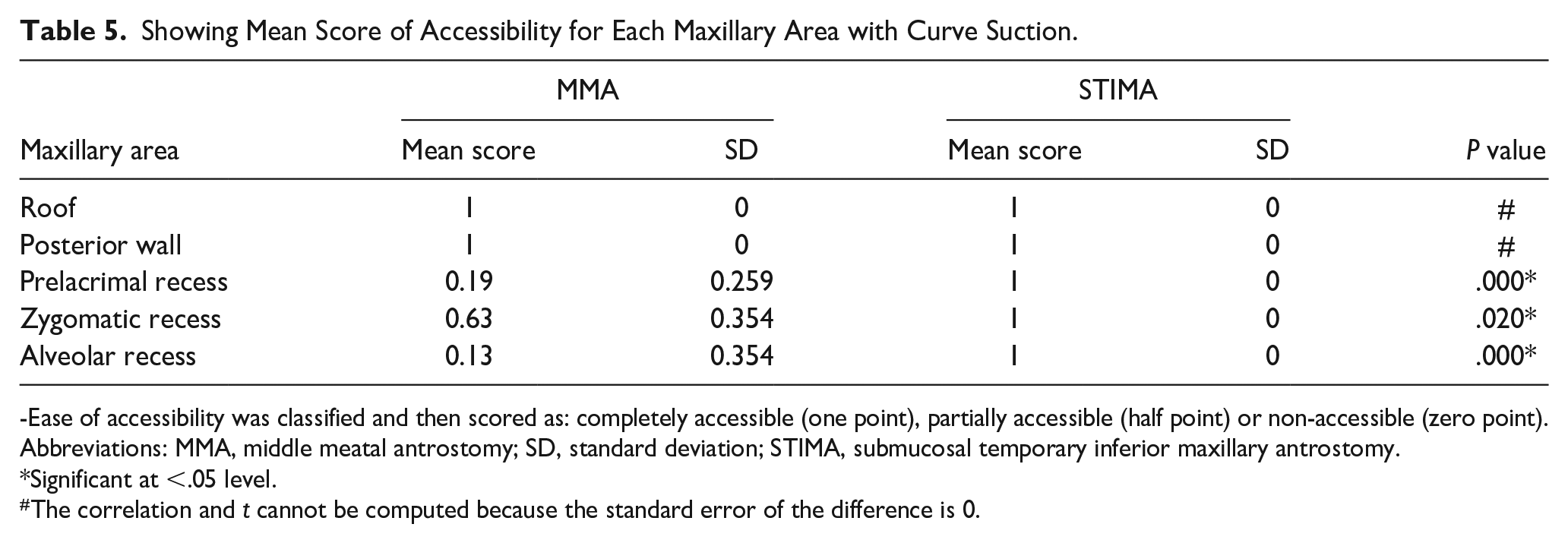
-Ease of accessibility was classified and then scored as: completely accessible (one point), partially accessible (half point) or non-accessible (zero point).
Abbreviations: MMA, middle meatal antrostomy; SD, standard deviation; STIMA, submucosal temporary inferior maxillary antrostomy.
Significant at <.05 level.
The correlation and t cannot be computed because the standard error of the difference is 0.
We did not encounter any direct orbital injury or injury to the NLD in our specimens, either through MMA or through the STIMA. We encountered small tears in the mucosal flap on 2 sides (25%). Nevertheless, the flap was sufficient to close the antrostomy site in a complete and relaxed manner on all 8 sides.
Discussion
In the pre-endoscopic era, the Caldwell-Luc procedure and IMA were the main approaches to address various maxillary sinus pathologies. 9 They were relatively safe and easy procedures that could be performed using a headlight. They provide wide and direct access to different aspects of the maxillary sinus. The use of a microscope can also provide excellent magnification and illumination during the Caldwell-Luc procedure, which would help in proper dissection and ablation of various pathologies, such as inverted papillomas and juvenile nasopharyngeal angiofibromas. 8 However, these procedures are not without potential complications. The Caldwell-Luc procedure could lead to temporary facial edema, bony thickening, and injury to the infra-orbital nerve and/or dental root injury with temporary or permanent sequelae. 9,10 Inferior maxillary antrostomy also has known complications, such as injury to the NLD, dental root injury, and injury to the greater palatine canal and its contents. Moreover, it could disturb the mucocilliary flow with resultant mucus recirculation, which could lead to recurrence of the disease and/or persistent postnasal drip. 3,8
Later, these procedures were gradually abandoned, especially at the beginning of the endoscopic era, when the concept of the natural and physiological mucocilliary flow was understood and adopted. 4 The procedures were replaced by endoscopic MMA, as this addresses the natural maxillary ostium to preserve mucus transport. Although endoscopic MMA has some known complications, such as orbital injury, injury to the NLD and/or recirculation phenomenon, it is still considered a functional and less invasive procedure and is currently the main approach and the standard of care for the majority of maxillary sinus pathologies. 11,12
Although the MMA is considered a safe and functional procedure, it does not provide full access to the maxillary sinus. Occasionally, this could limit accessibility in eradicating some pathologies, particularly when they are located in difficult-to-access locations, such as the anterior wall, prelacrimal recess, alveolar recess and/or zygomatic recess. 10 Hence, combined approaches are occasionally required, in which the pathology is addressed through MMA in addition to the IMA or Caldwell-Luc procedure. These approaches provide sufficient access for visualization and instrumentation; however, they are still associated with the aforementioned potential complications.
In the literature, few articles described some modifications to decrease the potential complications of permanent IMA. Zhao et al described a modified endoscopic meatal fenestration with a small mucosal flap and a bone window of 10 mm that was closed after clearing the sinuses by repositioning the flap back and placing an absorbable suture. Postoperatively, they reported an intact lateral nasal wall in all of their 32 patients with no disease recurrence, but mucosal edema was observed. 13 Choi et al described a minimal IMA by generating a small mucosal flap and a minimal bone window of 10 mm. They evaluated the closure of the window in their sample of 21 patients, with only 76% of them having complete closure of the endoscopic IMA window. 1 On the other hand, Landsberg et al approached inferior antrostomy differently by penetrating the medial maxillary wall using a 3-mm curved suction cannula about 5 mm posterior to the Hasner’s valve after medializing the inferior turbinate. The hole was then widened to about 8-10 mm using cutting forceps. After clearing the lesions of the maxillary sinus, the inferior turbinate was lateralized to its original position, and no tamponade was used at the antrostomy site. Of the 56 patients who underwent IMA in their group, only eight patients (14%) had closures while 48 patients (86%) had persistent antrostomies ranging between 5 and 6 mm. They also reported small cysts, synechiae, and palatal paresthesias. 10
Moreover, one of the established approaches to the maxillary sinus is the prelacrimal approach. In this approach, the maxillary sinus is accessed through a window that is made anterior to the NLD, after medializing the face of the inferior turbinate and removing bones of the pyriform aperture. It is an excellent approach to the hidden niches of the maxillary sinus but care has to be taken to avoid injuring the NLD and the superior anterior alveolar nerve. 14,15 Our approach might offer access to these niches with less dissection and drilling in selected case, without the need to mobilize the NLD and the face of the inferior turbinate. However, further studies on patients are needed to compare its safety, ease, and efficiency with the prelacrimal approach.
In this paper, we introduce our proposed modification of the conventional IMA. We proposed a larger submucosal flap that would allow for a larger temporary antrostomy. Having a larger inferior antrostomy would offer the surgeon better visualization and accessibility to address certain pathologies that are in difficult-to-access locations in a sufficient manner. We have demonstrated the superiority of the IMA over the MMA in visualizing and accessing certain areas of the maxillary sinus primarly using 0-degree, 30-degree, and 70-degree scopes. These areas include the prelacrimal, alveolar, and zygomatic recesses. The proposed larger mucosal flap did not cause any injury to Hasner’s valve or the NLD, as the initial incision was far anterior to them and they were entirely secured by being elevated safely within the flap. The larger size of the mucosal flap allowed for better mobilization to achieve complete closure of the temporary IMA. This would decrease the chances of the recirculation phenomenon and the recurrence of the disease and/or postnasal drip in the future. Since the proposed flap is relaxed and much larger than the antrostomy, it needs only absorbable dressing and would not need to be sutured at the end of the procedure.
Finally, our work is not without limitations. This study was performed on a limited number of cadaveric specimens and not on living patients. The viability of the flap, which is the cornerstone of the proposed modification, was not addressed as the study was performed on cadavers. This would be affected by the quality and integrity of the elevated flap and the wound status in the postoperative period. More randomized, controlled, and blinded studies are needed to assess the effectiveness of our proposed modification in addressing certain pathologies and the fate of the flap and its adequacy to close the antrostomy. The presence of any postoperative perforation or persistent antrostomy could again lead to mucus recirculation and postnasal drip.
Conclusion
STIMA is a relatively easy and safe modification of conventional IMA. It is a promising technique that provides great access for visualization and instrumentation of all difficult-to-access maxillary sinus locations without the potential complications of conventional IMA. Nevertheless, as this is a cadaveric study performed on a limited number of specimens, more prospective, blinded, and controlled studies on patients are needed to verify its potential risks and benefits.
Footnotes
Disclosures
We declare that this manuscript is original, has never been published, or under consideration for publication elsewhere (in part or in whole).
Conference Presentation
This paper was presented at the IFOS Dubai January 2023.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
IRB approval was obtained from IRB committee.