
Abstract
A bronchogenic cyst (BC) is a rare congenital cystic lesion, especially when located in the suprahyoid region of the anterior cervical front. We report a case of a male child who was misdiagnosed with a thyroglossal duct cyst due to the clinical presentation of a mass located near the anterior midline of the neck, in the region above the hyoid bone, which moved up and down with swallowing, characteristics consistent with a thyroglossal duct cyst. We excised the lesion under general anesthesia. Histopathological analysis revealed cartilage tissue, pseudostratified columnar epithelium of the cyst wall with cilia and mucous glands, finally diagnosing it as BC. BC should be considered in the differential diagnosis of neck masses.
Introduction
A bronchogenic cyst (BC) is a congenital cystic mass resulting from abnormal development of the respiratory system, caused by aberrant budding of the foregut on days 26 to 40 of embryonic development. First reported by Meyer in 1859, it is also known as a bronchial cyst.1,2 According to existing reports, BCs are classified into mediastinal type in about 75% of cases, intrapulmonary type in about 25%, and ectopic type in less than 1% based on the site of onset, particularly in cases occurring in the anterior cervical suprahyoid region. 3 Because BC rarely occurs outside the chest, it is not usually considered a differential diagnosis for a cystic mass in the neck of a neonate. 4 Here, we describe a case of a bronchogenic-derived cyst in the upper anterior cervical hyoid bone, clinically similar to a thyroglossal duct cyst.
Case Presentation
A 5-year-old male patient presented to the hospital with a painless neck mass that had been gradually enlarging over more than 6 months. The mass moved up and down with swallowing. Routine laboratory tests, including complete blood count, electrolytes, and urinalysis, were within the normal range, and there were no endocrine or metabolic abnormalities. The patient had no history of recurrent upper respiratory tract infections, dyspnea, or dysphagia. On examination, a soft, painless mass of about 5.0 × 3.5 cm was found above the hyoid bone, and the skin was free of fistulas. A chest X-ray showed no abnormalities in the mediastinum and intrapulmonary areas. An ultrasound scan of the neck revealed a hypoechoic cystic mass of 5.0 × 3.5 cm on the hyoid bone. An MRI T2 scan confirmed a hyperintense mass on the hyoid bone (Figure 1) with a capsule attached to the hyoid bone, leading to a preliminary diagnosis of a thyroglossal duct cyst.
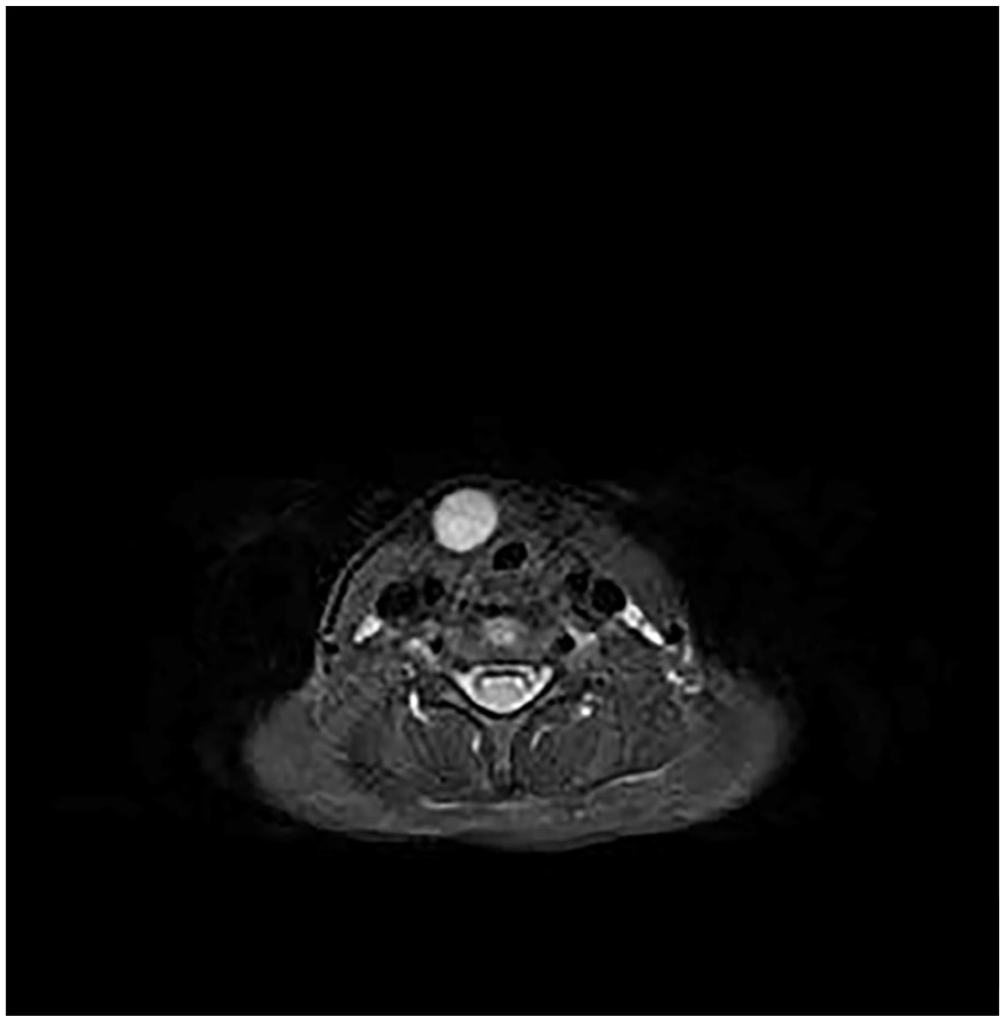
MRI T2 scan shows a round hyperintense signal.
Under general anesthesia, the lump was surgically removed through a horizontal incision in the neck above the hyoid bone. The lump was found under the platysma muscle, and no fistula or catheter was detected. Because the mass was attached to the body of the hyoid bone, it had to be removed along with the middle part of the hyoid bone. The mass was also attached to the cartilage of the anterior tracheal wall (Figure 2). The cyst was 0.1 cm thick, grayish-white, and tough in texture, containing a yellowish mucinous material upon dissection (Figure 3). Histopathology showed cyst fragments lined with pseudostratified columnar epithelium, displaying many cilia and mucus cells (Figure 4), leading to the diagnosis of a bronchial cyst. The patient has been followed for 2 years with no signs of recurrence.
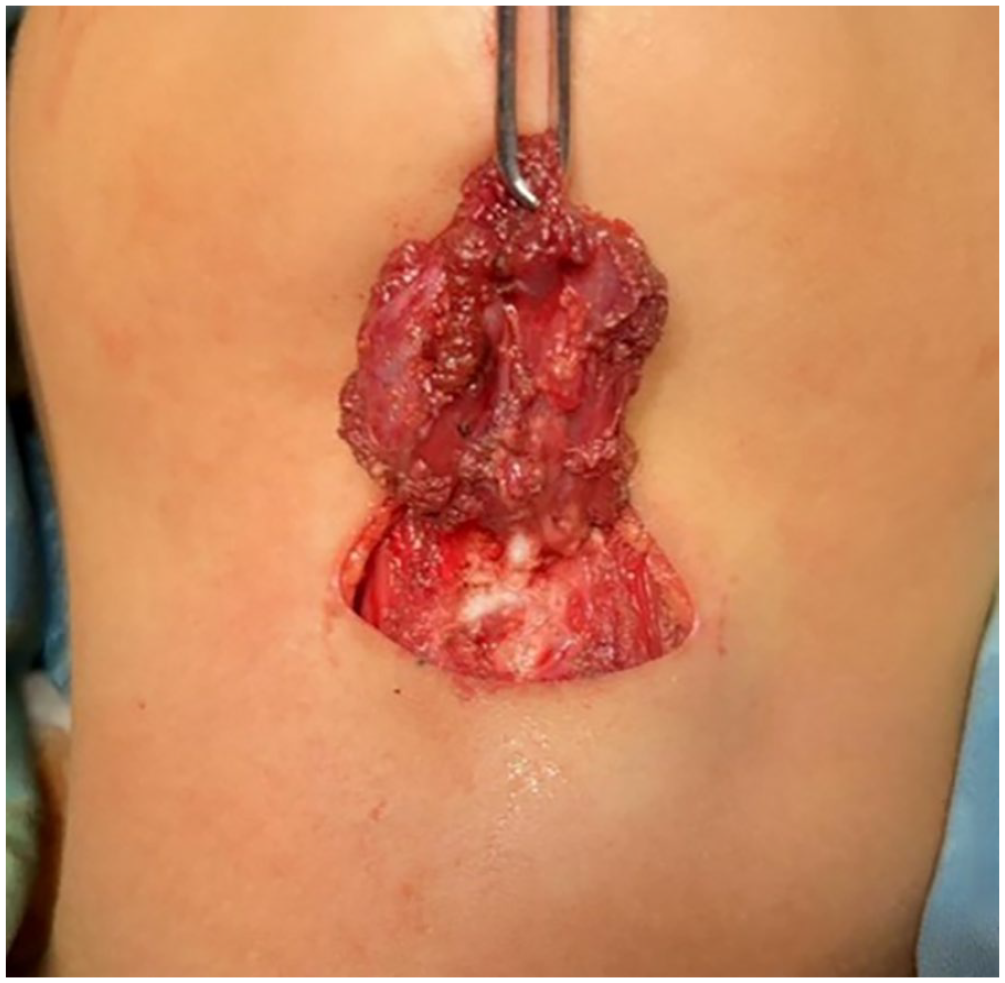
Mass connected to the anterior tracheal wall via cartilage.

Cyst containing yellowish mucinous material.
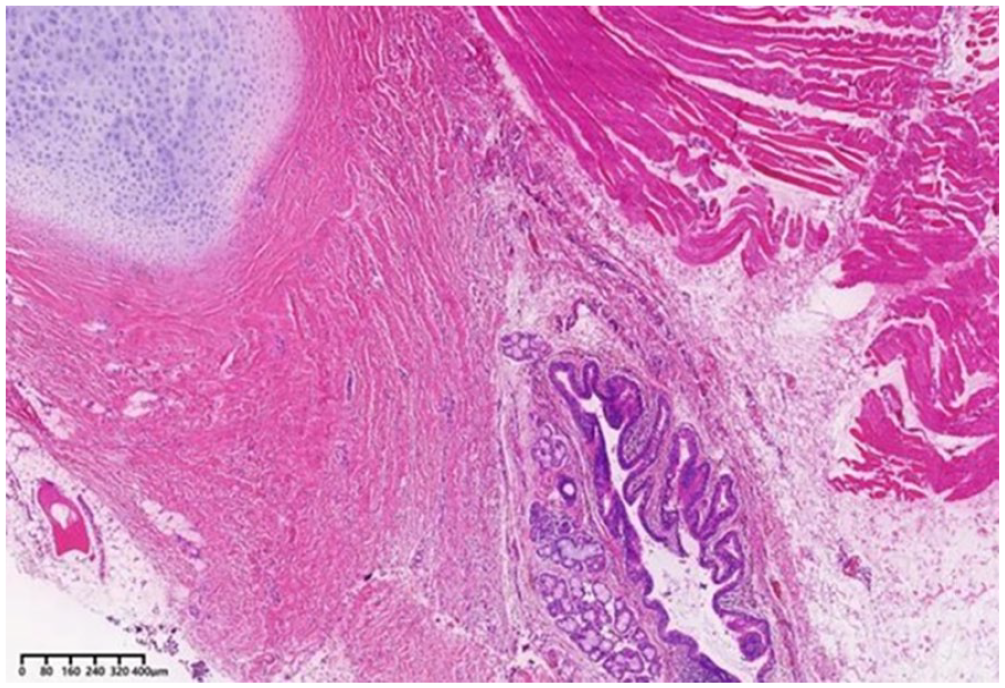
Cartilage tissue and pseudostratified columnar epithelium with cilia and mucus cells were observed (H&E ×40).
Discussion
BC is a congenital abnormality in the development of the respiratory system. The development of the respiratory system begins at the fourth week of the embryo, and between the fourth and sixth weeks of embryonic development, the primitive foregut separates to form the ventral trachea and dorsal esophagus.1,5,6 When the ventral foregut broncholung bud loses its connection with the tracheo-bronchial tree, the lung bud may migrate to an abnormal location. Abnormal budding of the lung can cause partial dysplasia, resulting in bronchial cysts, pulmonary sequestration, and tracheal lobe abnormalities.2,7 Ectopic BC can be observed in the oral cavity, neck, brain, dura, abdominal cavity, and other areas. Cervical bronchial cysts are thought to originate from the ascending migration of abnormal budding, with the trajectory of ascending migration divided into 2 types: deep neck and superficial neck. These cysts are usually not accompanied by other developmental abnormalities. A retrospective study of bronchial cysts of the head and neck by Mattingly et al showed that ectopic BC is more common in the oral cavity and extremely rare in the anterior part of the neck, 8 as demonstrated in this case report. BC lesions appear as unilocular, thin-walled, mucus-filled cysts, usually containing a mixture of water and protein mucus. The cyst may be thin and clear or viscous, with occasional bloody discharge or air.9,10 BC typically appears on CT scan as a round fluid-containing cyst with smooth, sharp, uniform margins, and a wide range of signals on MR T1W1 and a hyperintense T2W1 similar to cerebrospinal fluid. 11 Thick or irregular cyst walls are not typical of bronchial cysts and may indicate necrotizing tumors or lymphadenopathy. If the cyst is infected or has high protein and calcium content, its density may fall within the solid tissue range, increasing diagnostic uncertainty. Mild enhancement of the cyst wall on contrast-enhanced CT scan, which is evident in co-infection, may be helpful for further diagnosis. In addition, MRI and CT scans delineate the size and location of lesions to plan surgery.12,13 The clinical differential diagnosis of bronchial cysts includes thyroglossal duct cysts, branchial cleft cysts, teratomas, and schwannomas, usually differentiated by histopathological examination. 3 In reported cases of bronchial cysts, histopathology showed that the cyst wall epithelium consisted of pseudostratified columnar cells and cilia with mucus-secreting goblet cells, and rarely, a nonciliated cubic, columnar, or stratified squamous epithelium with intramural cartilage. 14 The histopathological findings (Figure 4) in this case were consistent with the typical features of BC described above. Symptomatic disease has been reported in 50% to 75% of patients with BC, and serious complications have been reported in 25% to 37% of patients. Dyspnea may occur when the cyst continues to enlarge and is infected, as BC is located anterior to the mid-cervical trachea in this case. The most common complication of BC is infection, with arrhythmias, pulmonary artery occlusion, severe hemoptysis, cyst rupture, superior vena cava syndrome, and malignant transformation also reported. Cases have clearly indicated left recurrent laryngeal nerve palsy due to mediastinal bronchial cysts. 9
Treatment of patients with BC depends on the patient’s age and symptoms at presentation. Percutaneous aspiration is simple, but because the bronchial epithelium of the cyst lining is still present, it will inevitably lead to cyst recurrence. 7 If symptoms are frequent, serious complications can occur if left untreated,15,16 and the risk of malignancy may increase. 17 Complete surgical resection is the treatment of choice,10,18,19 while conservative (watch and wait) management can be performed in high-risk patients who cannot tolerate surgery. Therefore, BC should be included in the differential diagnosis of patients with neck masses.
Footnotes
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The studies involving human participants were reviewed and approved by the ethics committee of Qingdao Women and Children’s Hospital. The patients/participants provided their written informed consent to participate in this study.