
Abstract
A rare disease called localized tonsillar amyloidosis can cause serious problems with airway patency in severe cases. This was the case with an elderly man who experienced difficulty breathing and swallowing due to enlarged palatine tonsils. The physical and imaging findings suggested tonsillolithiasis, and the patient underwent bilateral tonsillectomy. The diagnosis of amyloidosis was confirmed with histopathological examination using Congo red staining. Surgical intervention and careful follow-up care can be effective in these cases, which generally have a good prognosis.
Introduction
Localized amyloidosis is a rare type of amyloidosis that can be treated with surgery and has a better outlook than systemic amyloidosis. While localized amyloidosis is not uncommon, it is very rare for amyloid deposits to occur only in the bilateral palatine tonsils and they may be mistaken for tonsillolithiasis. Proper examination and tissue biopsy are necessary for accurate diagnosis. 1 To our knowledge, only two cases of localized tonsillar amyloidosis have been reported.2,3 In this report, we present a case of palatine tonsillar amyloidosis and compare it with previously published cases.
Case Report
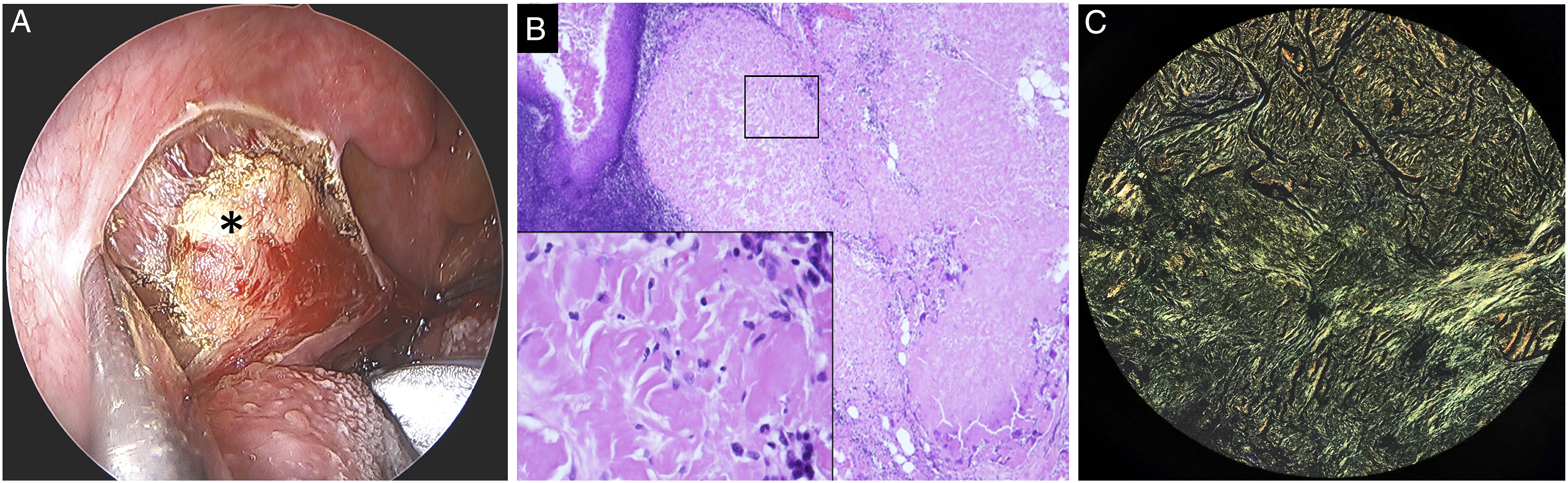
A 77-year-old man complained of feeling like there was something stuck in his throat and slight difficulty swallowing for an extended period of time. Three months prior, these symptoms were worse, particularly difficulty breathing while sleeping. The patient had a history of hypertension and hepatitis C but did not have significant weight loss, night sweats, or fever. On physical examination, multiple local protuberances were found on the bilateral palatine tonsils that contained substances similar to tonsilloliths (Figure 1A). Upon palpation, the texture was slightly firm but not tender. Nasopharyngoscopy showed that the right tonsillar protrusion extended deep into the larynx and was slightly in contact with the epiglottis (Figure 1B). Computed tomography revealed bilateral tonsillar hypertrophy with multiple opaque spots (Figure 1C). The patient underwent a bilateral tonsillectomy, and after the tonsil mucosa was surgically removed, an intact, opalescent, firm substance was found (Figure 2A). Histopathological examination with hematoxylin and eosin staining showed that the typical subepithelial lymphoid tissue was replaced by copious amorphous eosinophilic deposits (Figure 2B), and Congo red staining demonstrated apple-green birefringence under polarized light (Figure 2C). Systemic disease was ruled out, and the final diagnosis was localized amyloidosis of the bilateral palatine tonsils. The patient’s symptoms significantly improved after surgery, and there was no recurrence after 3 years of follow-up. Bilateral tonsil protrusions. A. bilateral tonsil protrusions containing tonsillolith-like appearance (star mark). B. Nasopharyngoscopy showing the right tonsillar protrusion deep to the epiglottis (star mark). C. Computed tomography revealing the protrusions containing opaque materials (star mark). Amyloid depositions. A. Macroscopic view of intratonsillar amyloidosis (star mark). B. Amorphous and eosinophilic infiltrate replacing subepithelial lymphoid tissue on hematoxylin and eosin stain (×40 and ×400). C. Apple-green birefringence on Congo red stain (×100).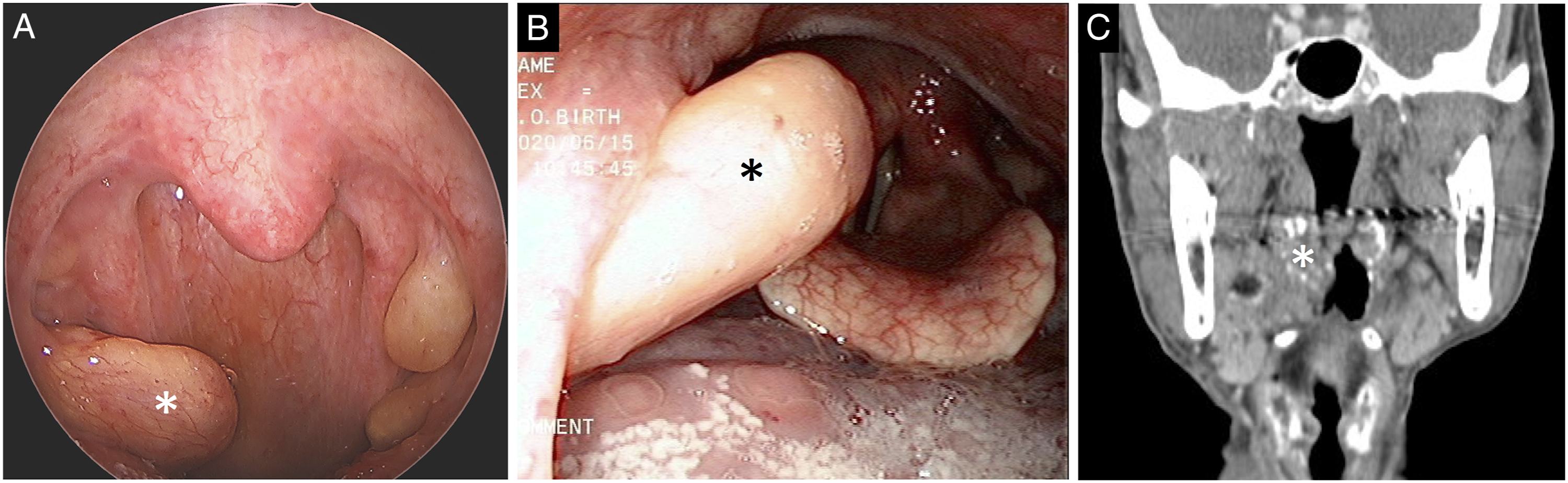
Discussion
Amyloidosis is a rare disorder that causes the formation of fibrillary protein deposits in various organs throughout the body. It is typically diagnosed through histopathological examination, during which the aggregates can display apple-green birefringence under polarized light with Congo red staining. 1 There are two main types of amyloidosis: systemic and localized. It also has four subtypes: light-chain amyloidosis (AL), reactive amyloid A amyloidosis, hemodialysis-associated β2-microglobulin amyloidosis, and hereditary transthyretin-related amyloidosis.1,4,5 Localized amyloidosis can affect organs such as the brain, endocrine system, thyroid, heart, or kidneys. 1 The prevalence of amyloidosis has been increasing in the United States and European Union in recent years, with an estimated incidence ranging from 3 to 12 per million persons per year. 2
Although amyloidosis is a rare disease, the head and neck region is known to be a common site for amyloid deposits, accounting for about 19% of reported amyloidosis cases. 4 Localized head and neck amyloidosis most commonly affects the larynx and thyroid (60%), followed by the trachea (9%), orbit (4%), and nasopharynx (3%). 3 Localized amyloidosis is usually associated with the AL type of protein produced by plasma cells. 5 Initial diagnostic tests, including lymphadenopathy evaluation, radiographic imaging, blood smear analysis, and bone marrow and abdominal fat biopsy, can help rule out underlying conditions such as lymphoma, multiple myeloma, and systemic amyloidosis. After a thorough evaluation, localized amyloidosis can be managed with surgical excision and follow-up care. 5
Primary localized amyloidosis of palatine tonsils.
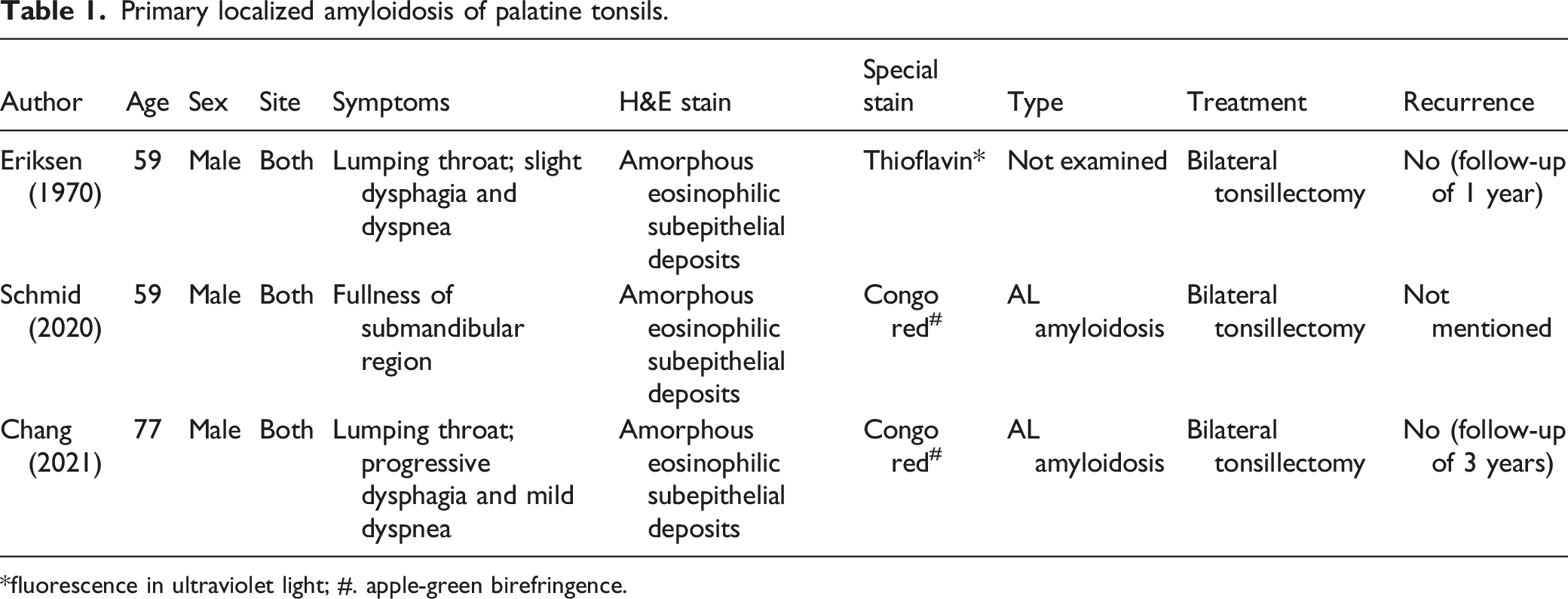
*fluorescence in ultraviolet light; #. apple-green birefringence.
Conclusion
Localized tonsillar amyloidosis typically affects the bilateral tonsils and occurs in older men, causing progressive difficulty swallowing and impaired breathing. Bilateral tonsillectomy with appropriate staining can lead to a definitive diagnosis and a good prognosis. However, more cases and longer follow-up periods are needed to fully understand the epidemiology of this rare disease.
Footnotes
Acknowledgments
The authors would like to thank Dr Liu for her assistance with the pathologic investigation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Institutional Review Board at Chang Gung Memorial Hospital has approved our study, which adheres to the principles outlined in the Declaration of Helsinki. In addition, the hospital’s board has granted an exemption from the requirement to obtain patient informed consent for our study (approval no. 201900520B0).