
Abstract
Objective:
To explore the effect of home skin temperature management in winter on the complications of expander and skin expansion efficiency in ear reconstruction patients.
Methods:
A total of 58 patients were involved and divided into control group and experimental group according to the different postoperative nursing methods. The control group was given routine nursing, and the experimental group received additional home hot compress guidance. At the end of expansion, complications, Visual Analog Scale (VAS) score, expansion time, and satisfaction score were used to evaluate the effect of the intervention.
Results:
Compared with the control group, the experimental group had a significantly-lower wound-related complications rate (7.14% vs 28.57%), lower VAS score (2.68 ± 1.19 vs 4.32 ± 1.02), and shorter expansion time (82.36 ± 8.69 vs 89.79 ± 9.87 days). Patient satisfaction was significantly higher in the experimental group (92.86% vs 67.86%), P < .05.
Conclusions:
During skin soft tissue expansion, home skin temperature management through hot compress can effectively reduce the incidence of complications, improve the expansion efficiency, reduce the pain of patients, and ultimately improve the overall satisfaction of patients.
Skin tissue expansion has been widely used in the repair of skin defects and congenital deformities. 1 Among them, the expansion technique plays a crucial role in ear reconstruction. 2 During the tissue expansion process, the mechanical tension exerted by the expander on the normal skin continuously leads to the regeneration of the skin, and the regenerated skin is similar to the adjacent skin in terms of color, texture, and luster. 3 This is the fundamental principle of skin expansion. However, during skin expansion, various complications such as pain, hematoma, infection, and expander leakage may occur, bringing secondary harm to patients. 4 Therefore, how to reduce the complications during the skin expansion period has always been the focus of researchers.
It is worth noting that the main characteristic of skin expansion is the continuous damage and re-healing of the local skin, and new skin is obtained in this process. 5 Interventions targeting skin healing may have an impact on the expansion outcome. A study has found that an early-wound temperature lower than the core body temperature will impede collagen deposition and reduce the activity of fibroblasts, thus delaying the healing process. 6 Moreover, the expanders for ear reconstruction are mostly implanted behind the ear, and the skin is often exposed during the expansion process, so the skin temperature is easily affected by environmental changes and fluctuates violently, especially in cold winter weather. In addition, the inflated expander also blocks the heat conduction from the deep tissue to the skin. Therefore, in winter, the temperature of the expanded postauricular skin is significantly lower than the core body temperature due to exposure to cold environments and the expander blocking heat conduction from deep tissues.
In conclusion, the research group intends to explore the effect of skin temperature management in winter on the complications of expanders and the expansion efficiency in ear reconstruction through a randomized controlled study.
Patients and Methods
Patients
A total of 56 patients who underwent complete expansion method ear reconstruction in our department during the winter of 2022 to 2023 were selected as the research subjects. Inclusion criteria were as follows: (1) age >6 years old; (2) meeting the diagnosis of congenital ear deformity; (3) undergoing complete expansion method ear reconstruction; (4) undergoing surgery in winter; and (5) informed consent of the patient or family members. Exclusion criteria were as follows: (1) accompanied by facial organ dysfunction; (2) local skin infection; (3) dysfunction of important organs such as heart, liver, brain, lung and kidney; and (4) autoimmune diseases. The enrolled patients were divided into a control group (n = 28) and a study group (n = 28) according to the different postoperative nursing methods, which were carried out during the expansion and water injection period after the implantation of the expander. This study was approved by the Hospital’s Ethics Committee (Approval No.: KY20212102).
Methods
Surgical and Water Injection Protocols
After anesthesia, the patient’s scalp was cut layer by layer to the galea aponeurotica according to the pre-designed range and surgical incision. The dissection was carried out in the deep layer of the galea aponeurotica, and the predetermined cavity was dissected in the superficial layer of the periosteum along the hairline deep to the periosteum. During the dissection process, attention was paid to protecting the facial nerve and posterior auricular artery. After the cavity was dissected and hemostasis was achieved, an oval or rectangular expander was placed, and the size and shape of the expander were selected according to the patient’s condition. Finally, the drainage tube and valve of the expander were externally fixed, and the wound was sutured. 15 ml of water was injected during the operation.
If there were no complications 5 to 7 days after the implantation of the expander, water injection expansion could be started. The protocol was a slow expansion of 1 ml/day, and the expansion cycle was about 3 months, with a total injection volume of 110 to 120 ml.
Intervention Measures
Control Group: The patients in the control group received routine nursing during the expansion period, including the following: (1) strict aseptic operation was required during the injection of the expander to avoid exogenous infection; (2) guiding the patient to carry out off-hospital nursing operations such as cleaning and disinfection; (3) guiding the patient to monitor the discomfort symptoms by himself/herself outside of the hospital and report to the doctor in time; and (4) conducting psychological intervention to reduce the patient’s mental health problems.
Experimental Group: On the basis of the intervention measures of the control group, the patients and their families were instructed to conduct home skin temperature management. A hot towel at about 40 °C (35 °C-42 °C) was applied for hot compresses on the expanded skin behind the ear, 3 to 5 times a day, 30 to 60 minutes each time. When the patient entered the outdoor environment, hats and other clothing were used to maintain the temperature of the expanded skin behind the ear and avoid abrupt temperature changes in skin.
Observation Indicator
Primary Observation Indicator: Follow-up personnel were arranged to collect the occurrence of complications of the expander in patients during the water injection expansion period, such as hematoma, infection, expander leakage, and abnormal blood supply of the skin flap.
Secondary Observation Indicators: (1) the pain degree of the patient during the expansion process was evaluated using the Visual Analog Scale (VAS) at the end of the expansion; (2) the expansion time of the patient was collected to reflect the expansion efficiency; and (3) the overall satisfaction degree of the patient with the expansion process (very satisfied, satisfied, dissatisfied) was collected at the end of the expansion.
Statistical Methods
The GraphPad Prism 8.0 (GraphPad Software) was used to analyze the experimental data in this study. Measurement data were expressed as (
Results
General Information of Patients
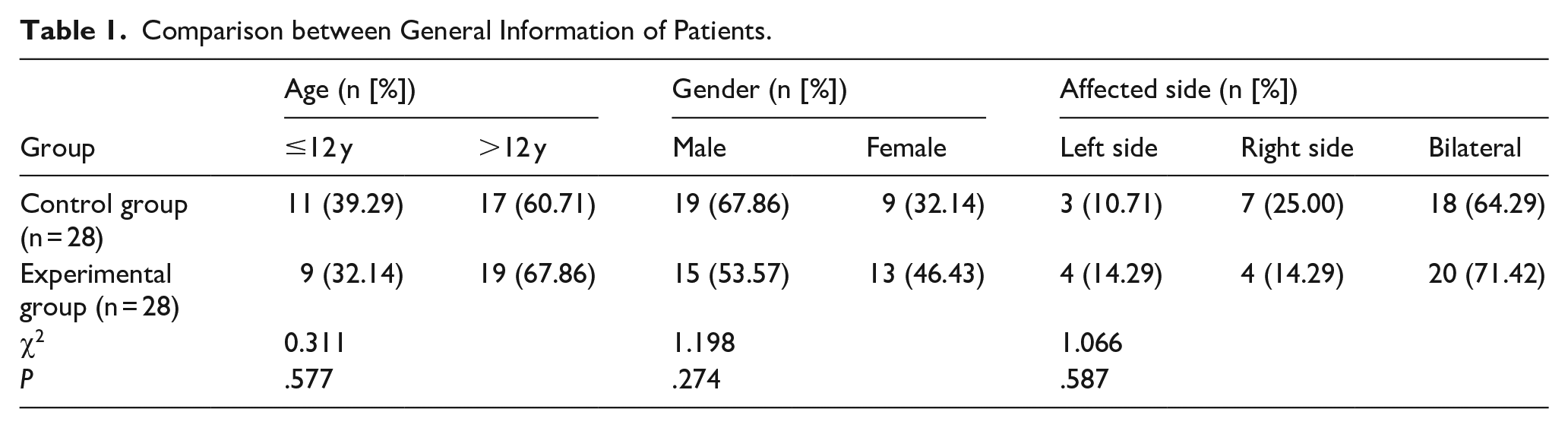
There was no significant difference in age, gender, BMI, and affected side between the control group and the experimental group, and the 2 groups of patients were comparable, P > .05 (Table 1).
Comparison between General Information of Patients.
Occurrence of Complications
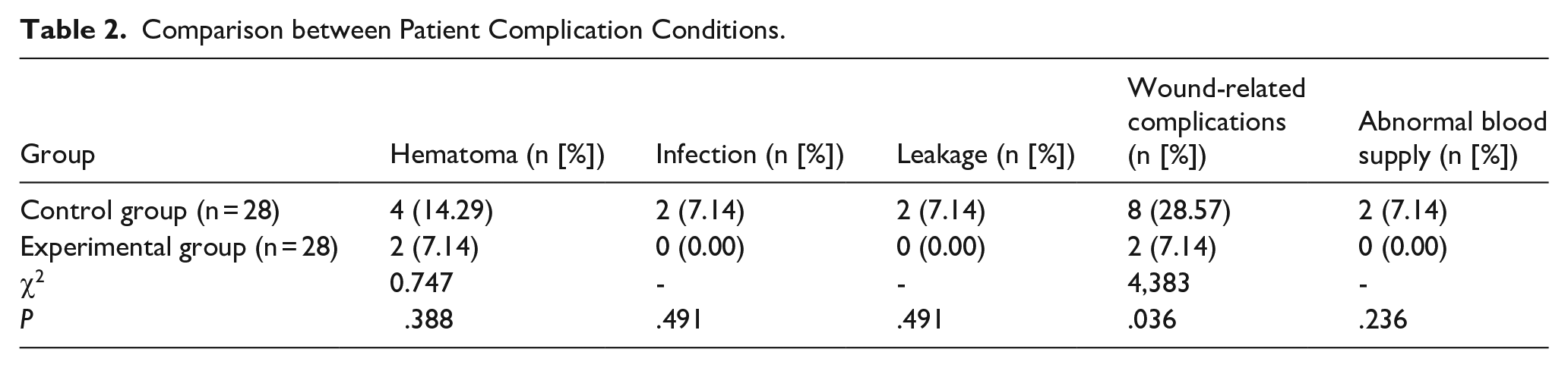
The experimental group had a significantly-lower wound-related complications (hematoma, infection, leakage) rate compared with the control group, P < .05. However, no significant differences were found in hematoma, infection, expander leakage, or abnormal blood supply between groups, P > .05. Meanwhile, the total complication rate in the experimental group was significantly lower than that in the control group, P < .05 (Table 2). In addition, among the 10 patients who developed wound-related complications, 1 (5.56% of 18 unilateral patients) was a unilateral patient and 9 (23.68% of 38 bilateral patients) were bilateral patients, P = .142.
Comparison between Patient Complication Conditions.
Pain Score and Expansion Time
The experimental group exhibited a significantly-lower VAS pain score and shorter expansion time than the control group, P < .05 for both (Table 3).
Comparison between Patient Pain Score and Expansion Time.
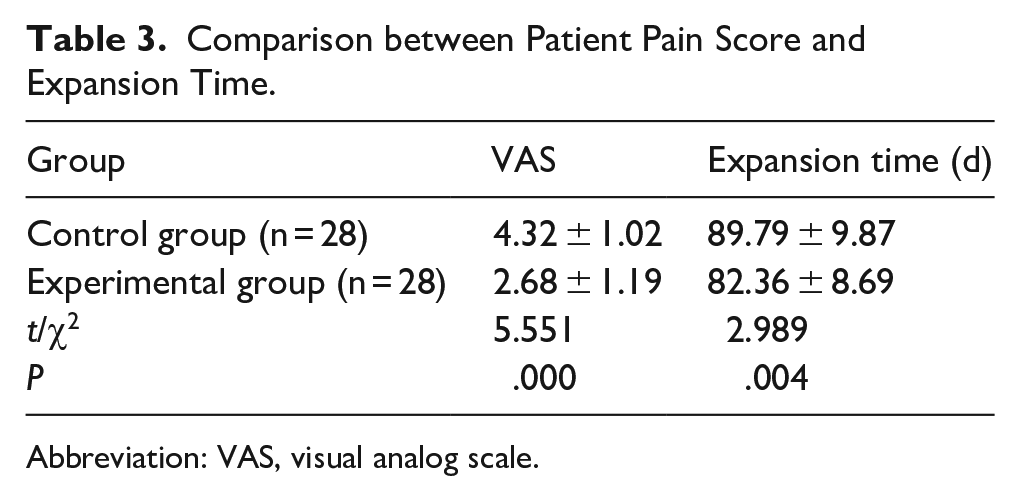
Abbreviation: VAS, visual analog scale.
Patient Satisfaction
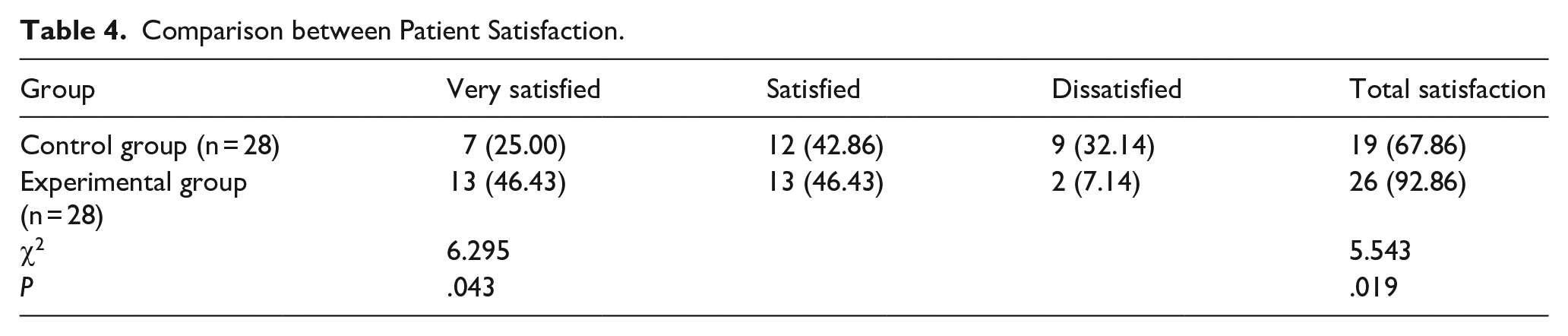
The total satisfaction rate was significantly higher in the experimental group than in the control group, P < .05 (Table 4).
Comparison between Patient Satisfaction.
Discussion
The main feature of skin expansion is the repeated damage and re-healing, and any factor that affects the healing of the injury may affect the outcome of the expansion. 5 It is worth noting that there is a complex sensor system in the skin, which enables it to sense the surrounding environment, such as temperature, humidity, and pressure. 7 However, after the patient undergoes the implantation of the skin expander, the large-scale cavity dissection and the inflated expander may both lead to the impairment of the skin sensory and temperature regulation functions; in particular, the skin temperature in winter will be significantly reduced.
Current clinical guidelines advocate that the control of pressure, humidity, and microbial population is an important factor in the local intervention of skin injury. However, the control of wound temperature has not been fully integrated into the standard treatment protocol. 8 The interaction between the wound thermal environment and the healing process is a field that lacks sufficient research. Studies have found that mild heat stimulation has a positive effect on wound repair. 9 Temperature plays an important role in the operation of each system in the body, and all cell functions are affected by it,10,11 and so is wound healing. 12 Under physiological conditions, the increase in skin temperature in the inflammatory stage of acute wounds will increase the local dermal blood flow, thus forming an environment conducive to wound healing. 13 On the other hand, in acute surgical wounds, when the temperature of the wound surface is lower than the core body temperature, the healing will also be delayed. 14 A study has shown that 33 °C is the critical threshold temperature for various physiological changes in the wound, and a temperature lower than this threshold will lead to a decrease in the activity of neutrophils, fibroblasts, and keratinocytes. 15 For the wound state with too low temperature, local heat treatment has been proven to enhance capillary blood perfusion and partial pressure of oxygen, increase the activity and collagen deposition of neutrophils, fibroblasts and keratinocytes, and increase the proportion of lymphocytes in the wound site, enhancing the immune response in the microenvironment and thus promoting wound repair. 16 Geng et al designed a self-regulating temperature control device with a temperature control range of 35 °C to 42 °C and applied it to wound treatment. The results showed that through the control of wound temperature, the inflammatory reaction of the wound in the experimental group was reduced and the healing rate was increased by 10%. 17 Therefore, with hot compress at ~40 °C, the experimental group showed a reduction in total complication rate and shorter expansion time than the control group, indicating improved expansion efficiency. However, no significant differences were found in severe complications (eg, infection, leakage).
Notably, the primary discrepancy in complication rates is predominantly observed in total wound-related complications, rather than individual hematoma, infection, and leakage. The hematoma is considered a surgery-related complication within several days after implantation surgery, which is less affected by warm compress. Modern expander technology has indeed reduced severe complications to a low baseline, as evidenced by the absence of statistical differences in hematoma, infection leakage, and blood supply to the skin flap. However, skin hypothermia induced by winter may reduce wound healing efficiency, which results in the increase in total wound-related complication rate observed in this study. Further studies with larger samples are needed to confirm the consistency of these findings. Additionally, we conducted a statistical analysis of patients with wound-related complications and found no significant difference in incidence rates between unilateral and bilateral cases. Theoretically, bilateral patients face greater challenges in home care than unilateral patients, and each ear in bilateral cases should carry a higher risk of complications. However, the actual results showed that there was no statistically-significant difference in the complication risk for each ear, which highlights the importance of additional intervention measures such as skin temperature management from another perspective.
During the late expansion phase, each fluid injection causes the skin flap to be acutely compressed, triggering intense headache. In some cases, the discomfort becomes so severe that it necessitates the withdrawal of fluid from the expander, thereby impeding the expansion process. Clinically, the skin expansion process is relatively long. During this period, the continuously-expanding expander exerts tensile force on the skin or compresses the surrounding nerves, causing the patient to be in a painful state for a long time, which seriously affects the quality of life of the patient. Ying et al found that the use of percutaneous acupoint electrical stimulation with appropriate intensity and frequency can effectively relieve the pain symptoms during skin expansion and improve the patient’s comfort so that they have the confidence to complete the treatment. 18 However, the professionalism of electrical stimulation makes it unable to be used as a daily-home-treatment method, and the popularization rate is not high. Therefore, the research group proposed home skin temperature management. In this study, after convenient hot compress management in the experimental group, the pain score during the expansion process was significantly reduced, and the satisfaction was significantly improved. A good expansion experience also has a positive promoting effect on the patient’s treatment compliance and prognosis.
However, this study also has certain limitations. First, there are relatively-few patients undergoing ear reconstruction in winter, which to some extent affects the reliability of the conclusion. Second, it is still difficult to control the skin temperature through hot compress, and more accurate and even self-adaptive temperature control dressings will be the research direction of the research group in the next step.
Conclusions
During skin soft tissue expansion, home skin temperature management through hot compress can effectively reduce complications, improve expansion efficiency, reduce patient pain, and ultimately improve overall satisfaction.
Footnotes
Consent to Participate
All patients in this study signed a written informed consent form.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author.