
Abstract
This case report describes a patient with a left ear deformity resulting from a flame burn sustained 20 years ago. The patient underwent an ear reconstruction procedure utilizing an expanded neck flap. The autologous rib cartilage was used as the framework, while an expanded neck flap served as the covering for the framework. The surgery was completed in 3 stages. Initially, tissue expanders were implanted and gradually inflated with water. After sufficient expansion, the expanders were removed, and the scar tissue was excised. Subsequently, the expanded flap was used to cover the defects, and the expanded neck flap was rotated to cover the autogenous costal cartilage framework obtained intraoperatively. Finally, the reconstructed ear was repaired by constructing the cephaloauricular sulcus, removing postauricular scars, and trimming the neck-flap pedicle. After a 1-year follow-up, the wound had healed satisfactorily with only minor complications. The shape of the reconstructed ear appeared realistic, and its function was maintained. Most of the scars were repaired, and the scarred alopecia was significantly improved. In patients with limited availability of the postauricular flap, especially burn patients, using an expanded neck flap can lead to superior outcomes.
Introduction
Ear reconstruction is a challenging procedure in plastic surgery. Classical ear reconstruction surgery is often constrained by the possibility of an insufficient flap in the mastoid region. In this respect, the skin expansion technique, which involves expanding the skin in the mastoid region and then using the expanded skin to reconstruct the auricle, is an effective method for ear reconstruction. Nevertheless, in burn patients, the limited supply of blood and lack of elasticity makes the postauricular skin unsuitable for ear reconstruction. The application of an expanded neck flap for ear reconstruction has remained largely unexplored in the literature. This study reports a successful case of using an expanded neck flap to reconstruct an ear.
Case Report
A 22-year-old female presented with a left-ear deformity caused by a flame burn sustained 20 years ago. The patient’s condition also included scars around the auricle and in the temporoparietal region. The left auricle was partially absent; however, the external auditory canal was undamaged. Upon examination, the temporoparietal skin showed scarred alopecia (Figure 1A and B).
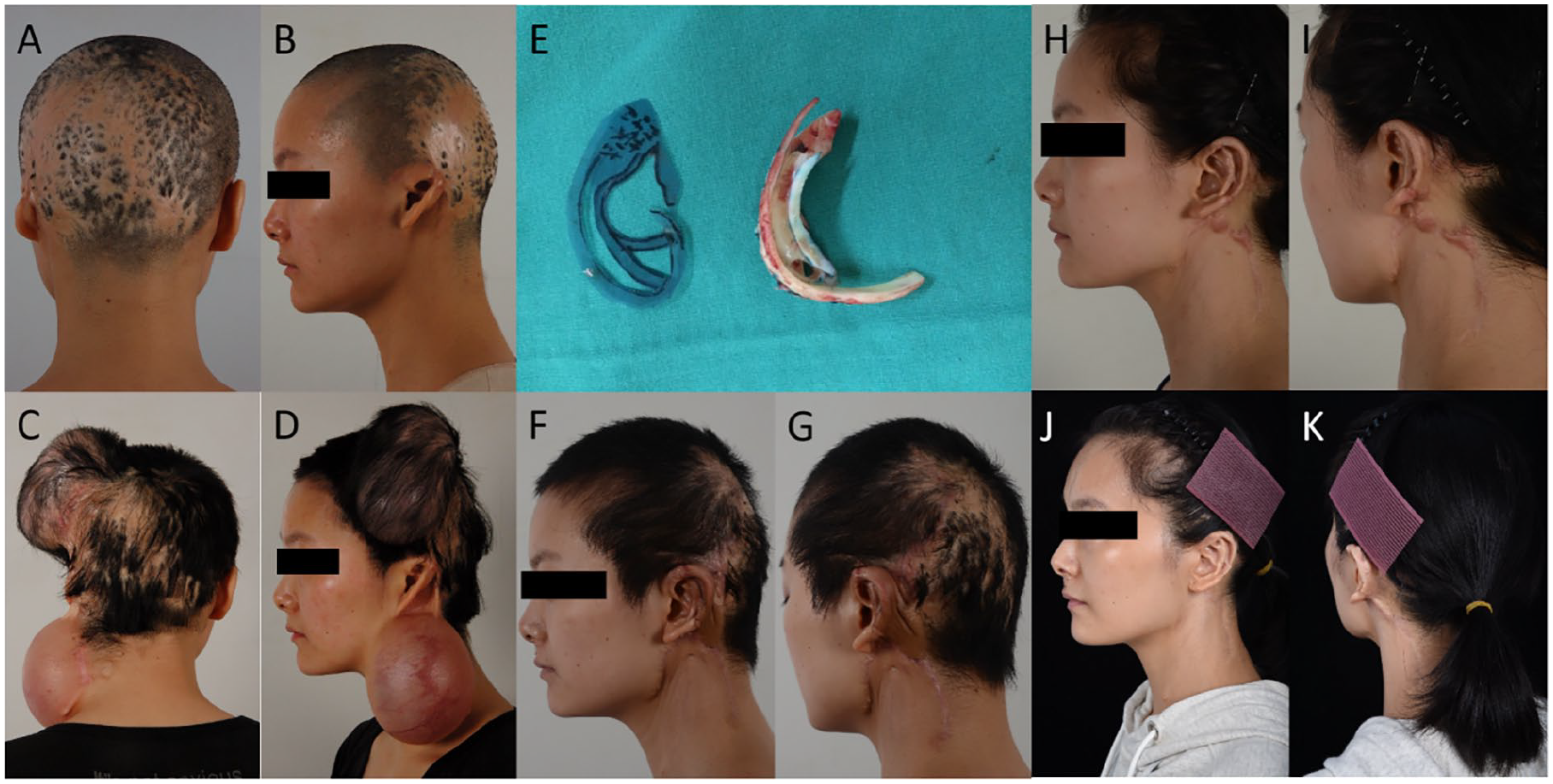
(A and B) Partially absent left auricle with undamaged external auditory canal. Scarred alopecia visible on temporoparietal skin. (C and D) Postexpander implantation. (E) Autogenous costal cartilage framework. (F and G) Post second-stage surgery. (H and I) One-year follow-up after the third-stage procedure. (J and K) Eighth-year follow-up after the third-stage procedure.
The patient underwent the first-stage surgery, which involved the implantation and inflation of tissue expanders. Two kidney-shaped expanders, 1 with a 300-ml volume and the other with a 250-ml volume, were implanted under the left parietal galea aponeurotica and behind the neck, respectively. Owing to the large amount of neck skin required, we completed the overexpansion of the expanders within 3 months by injecting 367 ml of water into the left parietal expander and 470 ml of water into the neck expander (Figure 1C and D). 1 The expanders were then maintained for 3 months. While a short maintenance period can lead to inadequate flap expansion, a long-term maintenance period can cause the neck skin to sag due to gravity, thereby increasing the risk of complications. In this case, a 3-month maintenance period proved to be effective and yielded satisfactory results.
Six months later, the patient underwent the second-stage surgery. After the expanders were removed, the scar tissue was excised, and the defects were repaired with expanded flaps. The expanded neck flap was rotated forward and upward around the occipital hairline to cover the autogenous costal cartilage framework obtained intraoperatively(Figure 1E-G). 2
The third stage of surgery was initiated 6 months after the healing of the second surgery. This procedure involved repairing the reconstructed ear, including constructing the cephaloauricular sulcus, loosening the postauricular scar, and trimming the pedicle of the neck flap.
Results
After a 1-year follow-up, the patient exhibited satisfactory wound healing with negligible complications. The reconstructed ear appeared realistically shaped, and its function was maintained. Most of the scars were repaired, and the scarred alopecia was significantly improved (Figure 1H and I). At the eighth-year follow-up, the reconstructed ear still maintained its shape. In addition, scarring was minimal and the color of the reconstructed ear closely matched that of normal skin, suggesting a favorable aesthetic outcome (Figure 1J and K).
Discussion
Ear reconstruction is an extremely challenging procedure in plastic surgery, with many established surgical methods, such as Brent’s 4-stage method,3,4 Nagata’s 2-stage method, 5 and various 3-stage methods. The 3-stage m ethods can be divided into those using expanders and those using delayed flaps.6,7 Three-stage methods involving expanders include those proposed by Park, 8 Zhuang et al, 9 and Jiang et al. 10 In the present case, the delayed postauricular skin flap method and the expanded postauricular skin method were not suitable due to scars in the auricular and temporal parietal areas. The only skin available in the periauricular region was located on the neck. Consequently, we chose to use the expanded neck skin method.
The key points of the surgical procedure are described below:
Owing to the requirement for a large amount of neck skin, the expanders should be hyperexpanded (e.g., by injecting 470 ml of water into a 250-ml expander) until the flap is thin and the blood vessels are clearly visible. During the expansion process, various complications may arise, such as infection, skin rupture, and obstruction of blood flow. These complications need to be promptly managed using aggressive measures, and surgical intervention can be considered at an early stage if needed. In our study, the expansion process proceeded without incident, and no complications were observed.
A short maintenance period may lead to inadequate flap expansion, while a long maintenance period may cause the neck skin to sag due to gravity, thus increasing the risk of complications. In the case reported in this study, a 3-month maintenance period proved to be effective and yielded satisfactory results. However, the optimal duration of maintenance needs to be determined based on a large number of sample observations.
When rotating the neck flap, it is important to pay attention to the blood supply to prevent excessive distortion of the pedicle or necrosis at the end.
In classical ear reconstruction surgery, the main goals of the third-stage surgery are to reconstruct the tragus, construct the external auditory canal, and repair the reconstructed auricle. However, in this case, it was crucial to manage the twisted pedicle, construct the cephaloauricular sulcus, and loosen the postauricular scar.
Footnotes
Acknowledgements
We are grateful for the patient’s willingness to share her story.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.