
Abstract
Background:
Usually linked with anti-neutrophil cytoplasmic antibodies (ANCA), granulomatosis with polyangiitis (GPA) is an uncommon systemic necrotizing vasculitis. Although GPA sometimes shows multiorgan involvement, the confined phenotype—mostly affecting the upper respiratory tract—can provide major diagnostic and therapeutic difficulties. Though nonsystemic, limited GPA might resemble chronic rhinosinusitis and is at risk for progression or consequences.
Case:
Following COVID-19 immunization and past COVID-19 infection, we describe a case of a 23 year-old girl presenting with persistent nasal obstruction, headache, severe facial pain, crustation, nose bleeding, and anosmia for 1.5 years. Examination revealed bilateral nasal ulceration and crusting; evaluation also indicated mucosal thickening and positive c-ANCA with high proteinase 3 titers. Without granulomatous characteristics, histopathology revealed persistent inflammation and inflammatory nasal polyps. The patient was first managed with methotrexate; therapy was upgraded to rituximab (RTX) due to ongoing symptoms. After RTX induction, the patient achieved clinical remission, with resolution of nasal symptoms and normalization of inflammatory markers. She stayed in remission at the follow-up.
Conclusion:
This case highlights the diagnostic complexity and therapeutic challenges associated with limited GPA, particularly when ear, nose, and throat symptoms predominate without systemic involvement. Key to reaching remission is early rheumatologic referral, interdisciplinary treatment, and rapid escalation to biologic therapy. RTX is a good and well-tolerated choice in refractory restricted GPA; yet more studies are warranted.
Introduction
Granulomatosis with polyangiitis (GPA), formerly known as Wegener’s granulomatosis, is a systemic necrotizing vasculitis primarily affecting small- to medium-sized blood vessels. It is closely associated with anti-neutrophil cytoplasmic antibodies (ANCA), particularly those targeting proteinase 3 (PR3).1,2 While GPA commonly affects the respiratory tract and kidneys, a localized form—limited GPA—predominantly involves the ear, nose, and throat (ENT) without systemic organ involvement. 3 Limited GPA is often misdiagnosed as chronic rhinosinusitis due to its nonspecific symptoms, yet it carries the risk of progression and complications. 4
The etiology of GPA remains unclear but is thought to involve genetic, environmental, and infectious factors. Chronic nasal colonization with Staphylococcus aureus has been linked to disease relapses. 5 Additionally, genome-wide association studies have identified genetic predispositions related to HLA-DP, SERPINA1, and PRTN3 genes. 6 Diagnosis is guided by the 2012 Chapel Hill Consensus Conference criteria, which emphasize necrotizing granulomatous inflammation, ANCA positivity, and clinical presentation.7,8
Limited GPA primarily manifests as nasal crusting, obstruction, and recurrent epistaxis. Unlike systemic GPA, renal and pulmonary involvement is absent, though some cases can transition to a more diffuse disease course.9,10 Treatment typically involves immunosuppressive agents such as methotrexate (MTX) for nonsevere cases, with escalation to biologics like rituximab (RTX) in refractory disease.11,12 Studies, including the RAVE trial, have demonstrated RTX’s efficacy in inducing remission, particularly in relapsing cases. 12
This case report presents a 23 year-old female with limited GPA following COVID-19 infection and vaccination. It highlights the challenges in diagnosing and managing localized disease, the role of ANCA serology in guiding treatment, and the effectiveness of RTX in achieving remission and maintenance.
Case Presentation
We report the case of a 23 year-old medically free female who presented to the rhinology clinic with persistent nasal crustation, obstruction, headache, severe facial pain, and anosmia for 1.5 years. Her symptoms began 1 week after receiving the COVID-19 vaccine, with a preceding history of COVID-19 infection. She also reported recurrent episodes of epistaxis and painful nasal ulcerations with poor wound healing. She had no joint pain or swelling, chest symptoms, or lower limb edema. Nasal examination revealed bilateral nasal crusting with ulceration. There was also an anterior, medium-sized septal perforation. The nasopharynx was clear with no masses. Flexible nasopharyngoscopy demonstrated an unremarkable oropharyngeal area with a patent airway and bilaterally mobile vocal cords, with no masses. Ear examination was unremarkable, with intact tympanic membranes bilaterally. Additionally, neck and eye examinations were also unremarkable. The rest of the physical examinations were unremarkable for systemic involvement. Her laboratory results showed an acceptable white blood cell count (11), positive c-ANCA, and markedly elevated PR3, as well as mild thrombocytosis, mild anemia, elevated Erythrocyte Sedementation Rate (ESR) (27), and C-Reactive Protein (CRP) (14). Screening for Tuberculosis, hepatitis B, and hepatitis C was negative.
Chest X-ray showed no abnormalities, aside from linear vertical opacities deemed artefactual. Lung fields, cardiac silhouette, and mediastinum were otherwise normal. Computorized Tomography (CT) imaging of the paranasal sinuses revealed mucosal thickening in the left maxillary sinus, bilateral nasal cavities, and left inferior turbinate hypertrophy. Both osteomeatal units appeared patent, and no fluid levels were noted (Figure 1). CT of the temporal bone was unremarkable with clear mastoid air cells, normal ossicular chains and inner ear structures, and a high-riding left jugular bulb.

Coronal CT of the paranasal sinuses (PNS) showing mucosal thickening in the left maxillary sinus, bilateral nasal cavities, and left inferior turbinate hypertrophy.
Biopsies were taken from the nasal cavity, demonstrating benign respiratory epithelium undergoing autolysis with underlying chronic inflammation and scattered eosinophils. Additional biopsies were suggestive of inflammatory nasal polyps.
She was referred to rheumatology due to c-ANCA and PR3 results. Given the clinical presentation of recurrent nasal bleeding, crusting, ulceration, and imaging findings without evidence of polyposis or destructive lesions, she was diagnosed with limited GPA.
Initial management included MTX 15 mg weekly and folic acid. During follow-up, despite symptomatic improvement, nasal obstruction persisted, and the nasal mucosa became dry and fibrosed due to the effects of MTX and disease activity. At this stage, the treatment was escalated to RTX therapy. The patient received 3 doses of RTX, completing induction on March 21, 2024, while continuing MTX. During the first RTX infusion, she developed an urticarial rash over the cheeks and ears with nasal congestion, which resolved following IV hydrocortisone and antihistamines. Subsequent RTX infusions were tolerated well under close monitoring.
Follow-up endoscopic evaluation showed synechiae bilaterally between the septum and turbinates, with no signs of ulceration, bleeding, or erosion. Her nasal symptoms improved significantly, with no active epistaxis, no hearing loss, and no constitutional symptoms. Labs showed normalized inflammatory markers, and chest imaging remained stable. Due to vitamin D deficiency, she was started on cholecalciferol and multivitamins. After completion of RTX induction, MTX was discontinued per plan, and she continued to follow-up with both rheumatology and ENT.
At her most recent visit, 18 months after initial presentation, the patient remained clinically stable and in remission from GPA, with only mild sinusitis and no new complaints. Her nasal examination revealed the following (Figures 2 and 3).
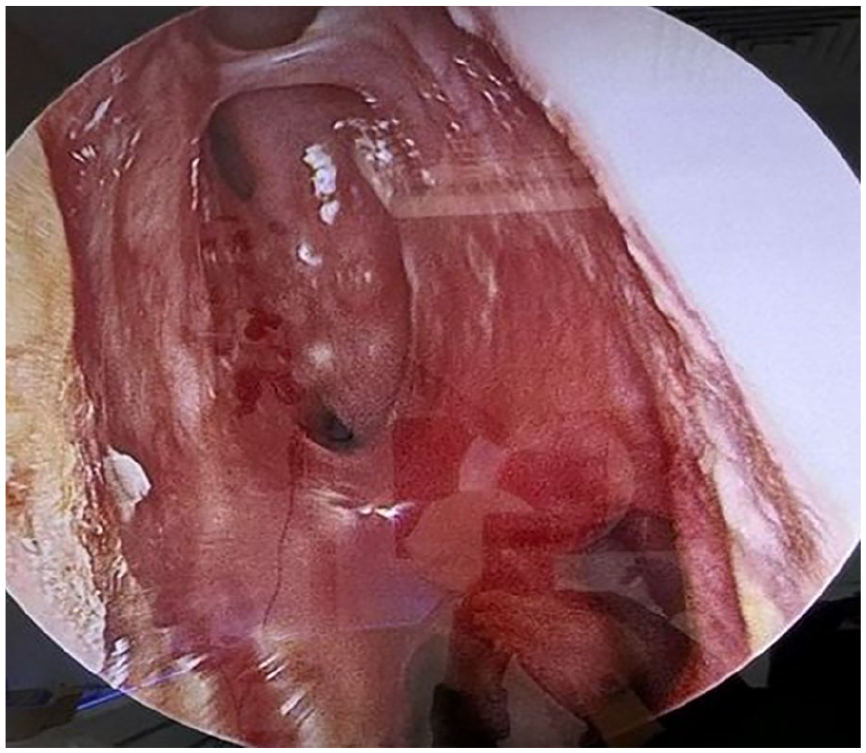
The left nasal cavity shows crusting and thick scarring involving both the superior and inferior aspects between the inferior turbinate and the nasal septum. The mucosa appears healthy, with no evidence of laceration or bleeding.
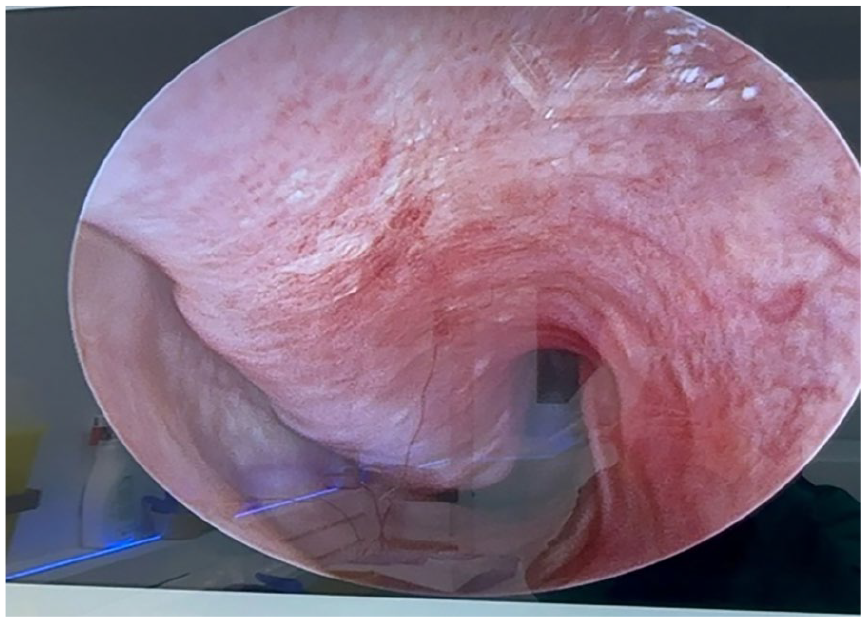
The right nasal cavity shows healthy mucosa with a thick, extensive adhesion between the inferior turbinate and the nasal septum, with no evidence of laceration.
And during the follow-up, patient education was provided regarding her condition, treatment plan, and follow-up needs.
Discussion
GPA is a systemic necrotizing vasculitis that can present itself in a variety of clinical presentations and can change the course of the illness. A young female patient arrived with protracted severe facial pain associated with nasal congestion, crustation, and anosmia: first suggestive of limited GPA based on biopsy results; finally diagnosed as limited GPA based on highly positive c-ANCA and PR3 titers. The patient’s symptoms were initially suggestive of chronic rhinosinusitis. Its restricted but refractory nature, the absence of systemic organ involvement, and the development of bilateral nasal synechiae were the primary clinical challenges that this case presented. This highlights the diagnostic and therapy issues that are associated with a limited GPA presentation.
When it comes to GPA, ENT involvement is the most common manifestation, and it can occur in as many as 100% of patients when they are diagnosed. 9 In other cases, it is the only symptom or the predominant symptom as well. Even though systematic GPA typically reveals the involvement of the kidneys or lungs, the confined phenotype that this patient displays may lead to an incorrect diagnosis or the patient’s condition being handled conservatively for extended periods due to its nonspecific and slow progression. When dealing with atypical or recurrent sinonasal pathology, this highlights the importance of immediately referring the patient to a rheumatologist and conducting a comprehensive evaluation.
This case illustrates the challenges in diagnosing GPA, particularly when serological and histopathological findings are incongruent. The patient exhibited standard upper respiratory tract symptoms and significantly elevated c-ANCA and PR3 titers; nevertheless, nasal biopsies were uninformative, revealing mainly chronic inflammation and inflammatory polyps, devoid of any granulomatous features. This scenario parallels the findings of Teames et al, 13 wherein 3 of 26 seronegative individuals exhibited positive biopsies. This indicates a distinction between biopsy and serology in localized GPA. The extensive cohort analysis revealed that 16% of patients with restricted GPA exhibited both negative serology and biopsy results, yet were ultimately diagnosed through clinical suspicion and responded to immunosuppressive therapy. These findings illustrate the constraints of current diagnostic methods in identifying early or isolated GPA and underscore the significance of clinical judgment. Despite initial varied or negative test findings, GPA should be taken into account when patients exhibit persistent ENT symptoms such as ulcers, crusting, or synechiae.
This case is unique in several significant aspects, including the onset of sinonasal symptoms following the administration of the COVID-19 immunization and the presence of protracted severe facial pain, nasal ulceration without systemic dissemination, and the development of considerable nasal synechiae, which is a rather uncommon but significant complication in GPA. New data on autoimmune events that are temporally related to vaccines begs for additional research to be conducted, even though a direct causal link between COVID-19 immunization and the beginning of GPA has not yet been established. Furthermore, the patient’s cutaneously limited allergic reaction to RTX, which was treated with antihistamines and steroids, highlights the necessity of appropriate care during the infusion of RTX as well as the viability of continuing treatment under altered circumstances.
Concerning treatment, the patient exhibited a partial response to MTX and achieved sustained remission after receiving RTX induction. This is consistent with the findings of the RAVE study, which showed that RTX was not inferior to cyclophosphamide and likely offered a potential advantage in the treatment of recurrent sickness. 12 Furthermore, RTX was found to be an effective drug for remission induction and maintenance therapy, despite the use of lower doses of glucocorticoids and RTX than in previous studies. 14 RTX appears to be effective for the induction and maintenance of stable remission off glucocorticoids in patients with GPA who failed to respond to cyclophosphamide or have contraindications for cyclophosphamide. RTX was well tolerated in these patients, and the short-term safety profile is encouraging. 15 This instance highlights the clinical value of RTX in managing restricted and refractory GPA, as well as its acceptable safety profile when given under appropriate monitoring. Initial concerns regarding RTX-related hypersensitivity are there; however, the fact that RTX induction was completed without any more incidents suggests that pre-medication techniques and modest infusion rates are effective means of minimizing the likelihood of such risks occurring.
Although the patient’s outcome was favorable, this case had several limitations. Although the noninvasive data confirmed the diagnosis according to the Chapel Hill criteria, like other studies, there was no evidence of granulomatous inflammation in the histological examination. It is still necessary to conduct long-term follow-up investigations to assess the possibility of systemic progression, relapse, or treatment-related complications. These limitations bring to light potential areas of investigation for future study, particularly concerning prognostic markers of disease development in limited GPA and the value of early biologic therapy in influencing long-term outcomes.
And there are also other studies that are similar to our case and are presented in the Table 1 for comparison.
Several Studies That Have Isolated Granulomatosis With Polyangiitis.
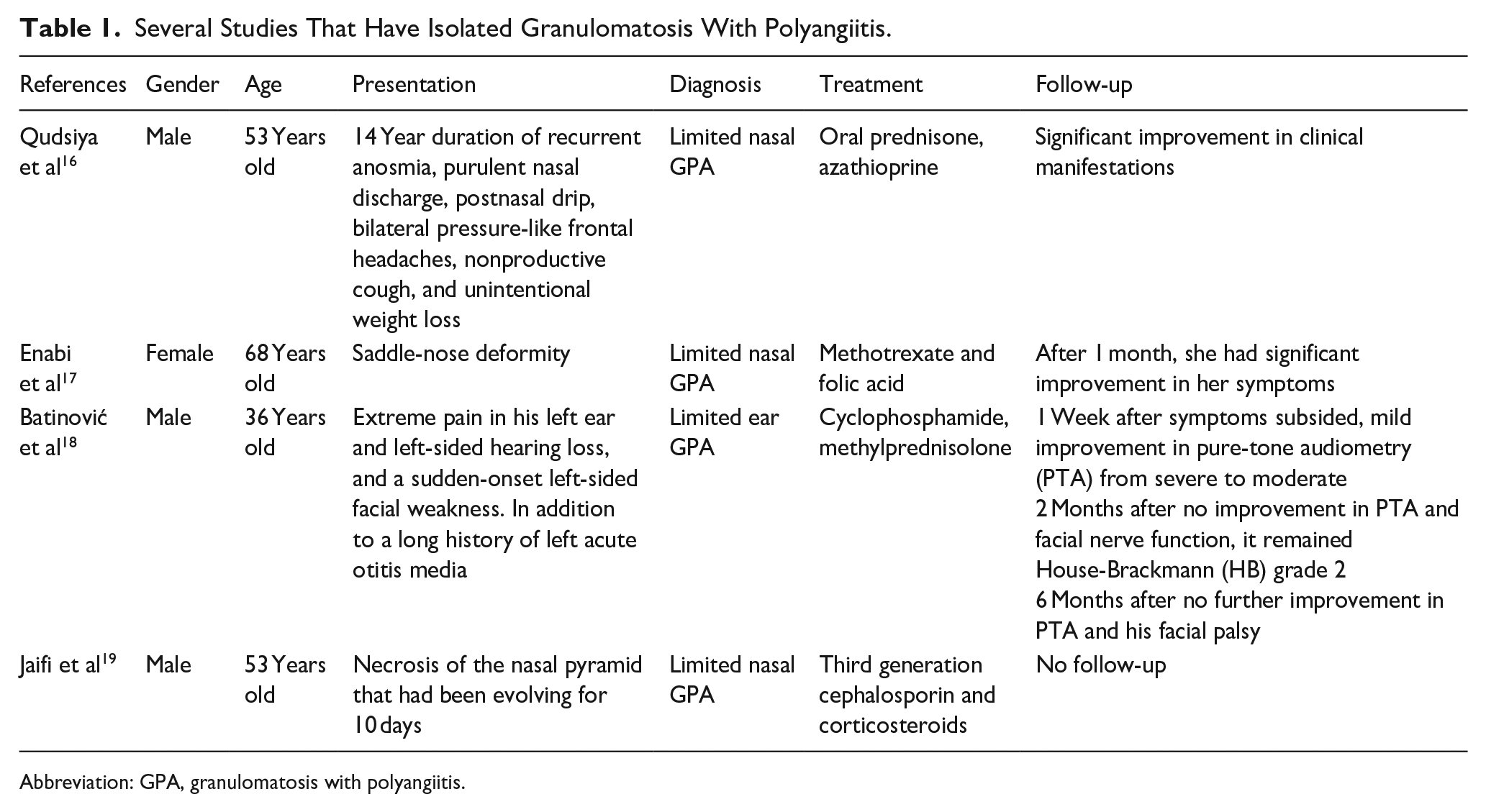
Abbreviation: GPA, granulomatosis with polyangiitis.
Conclusion
To conclude, this illustration demonstrates that a restricted GPA may continue to be resistant to conventional immunosuppression. Early detection, multidisciplinary management, and individualized immunotherapy can prevent further complications of the disease and are the primary factors that determine whether remission can be achieved and whether quality of life can be preserved. Clinicians need to maintain a high index of suspicion for vasculitis, particularly in patients who have severe facial pain associated with recurrent nasal ulceration and crustation. When positive ANCA serology is taken into consideration, this is especially true. During the early stages of refractory localized disease, RTX is a therapeutic option that is both safe and effective, even in individuals who have a moderate level of hypersensitivity. It is necessary to conduct additional studies to clarify the various triggers of GPA initiation and to investigate the long-term implications of early RTX consumption, particularly the role that COVID-19 vaccination plays in the activation of the autoimmune system.
Footnotes
Ethical Considerations
Ethical approval was obtained from the King Saud University IRB office, and all methods followed relevant guidelines and regulations.
Consent to Participate
Informed consent was waived due to the retrospective nature of the study, as approved by the Institutional Review Board. In addition, our center presents each patient with a paper declaring their approval for the use of their data for research purposes early in their admission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to [e.g., privacy/ethical/commercial restrictions]. Still, they are available from the corresponding author on reasonable request.