
Abstract
Background:
The management of subglottic stenosis (SGS) in granulomatosis patients with polyangiitis (GPA) has no clear guidelines. This systematic review aimed to identify different surgical techniques and evaluate the outcomes of applied procedures.
Methods:
An electronic search was performed using 3 major databases, CINAHL, PubMed, and Clinical key, to include relevant studies published from the databases from inception through January 2017. All primary studies reporting treatment of SGS in cases with GPA were included. Articles were excluded if not relevant to the research topic or if they were duplicates, review articles, editorials, short comments, unpublished data, conference abstracts, case reports, animal studies, or non-English studies.
Results:
Thirteen papers were included in our systematic review with a total of 267 cases for the qualitative review Endoscopic approaches showed favorable outcomes with the need to use multiple procedures to achieve remission. The open transcervical approach showed excellent results mainly after failure of other endoscopic techniques. Tracheostomy was necessary for severe respiratory obstruction symptoms. Medical treatment was essential for stabilizing the active disease and therefore may enhance the success rate postoperatively.
Conclusion:
Subglottic stenosis in patients with GPA requires a multidisciplinary approach to provide optimal management regarding disease activity, grade of stenosis, and severity of symptoms.
Introduction
Granulomatosis with polyangiitis (GPA) is a multi-organ disorder that is characterized by necrotizing granuloma and vasculitis that affect the upper respiratory passages, lungs, and kidneys. 1 Granulomatosis with polyangiitis is diagnosed by the presence of necrotizing granulomatous inflammation of the upper respiratory tract and small to medium size vessel vasculitis upon pathology or antineutrophil cytoplasmic antibody (ANCA) testing. 2
The American College of Rheumatology has set number of diagnostic criteria for GPA with 2 or more being suggestive of GPA. Their criteria entail nose ulceration or discharge, lung infiltrates or cavities, kidney involvement, and granulomatous formation as evident on biopsy. 3 Although cardiac involvement in GPA is quite rare, head and neck manifestations are common in GPA with variable clinical manifestations ranging from mild to potentially life-threatening. 4,5
Subglottic stenosis (SGS) has been estimated to present in approximately 16% to 23% of patients with GPA. 5 Stenosis mainly affects the subglottic or proximal trachea but may extend into the distal trachea and bronchi. 6 There are several options for the management of SGS with different approaches and variable outcomes. Subglottic stenosis can be managed with endoscopic techniques, and this includes balloon dilation, corticosteroid injection, and laser debridement. Additionally, open airway surgery with resection or reconstruction of the airway is another surgical option. 7 The optimal modality of management of SGS in GPA patients remains unclear and challenging in the absence of standard guidelines. Therefore, the aim of this systematic review was to identify different surgical techniques for the treatment of SGS in patients with GPA and evaluate the outcomes of applied procedures.
Methods
Study Design and Search Strategy
A systematic review of the literature has been carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. In February 2021, a systematic electronic search was conducted using 3 major databases, CINAHL, PubMed, and Clinical Key, to identify relevant articles. The following search strategy/Boolean operators were used: “Granulomatosis with polyangiitis,” (OR) “(GPA),” (OR) “Wegeners’s granulomatosis,” (OR) “Wegner granulomatosis,” (OR) “Wegener granulomatosis” (AND) “acquired subglottic stenosis,” (OR) “subglottic stenosis.” A medical subjective headings search with the term “Granulomatosis with polyangiitis/Surgery” was applied.
Selection Criteria and Screening Process
Two independent reviewers independently screened the articles against the inclusion criteria based on their titles and abstracts. Discrepancies between reviewers’ selections were resolved through interactive discussions. Inclusion criteria entailed all primary studies reporting the treatment of SGS in cases with GPA with no restriction on age and ethnicity. Articles were excluded if not relevant to the research topic or if they were duplicates, review articles, editorials, short comments, unpublished data, conference abstracts, case reports, animal studies, or non-English studies. All full-text articles that met the eligibility criteria were obtained and considered for full-text screening.
Data Extraction and Result Analysis
Two authors independently extracted the data from the included studies using a standardized data extraction form. The form contained baseline data, such as authors, country, year of publication, sample size, duration of follow-up, gender, and age. Additionally, information about the presenting symptoms of GPA including ANCA positivity and different organ involvement were extracted. Management plans and outcomes of different interventions were also reported.
Results
Search Results
The electronic search retrieved 209 papers after removing duplications by using EndNote (Figure 1). Afterward, 139 were excluded based on title and abstract screening, and 70 papers were assigned for further full-text screening. Finally, only 13 papers were included in our systematic review for qualitative analysis.
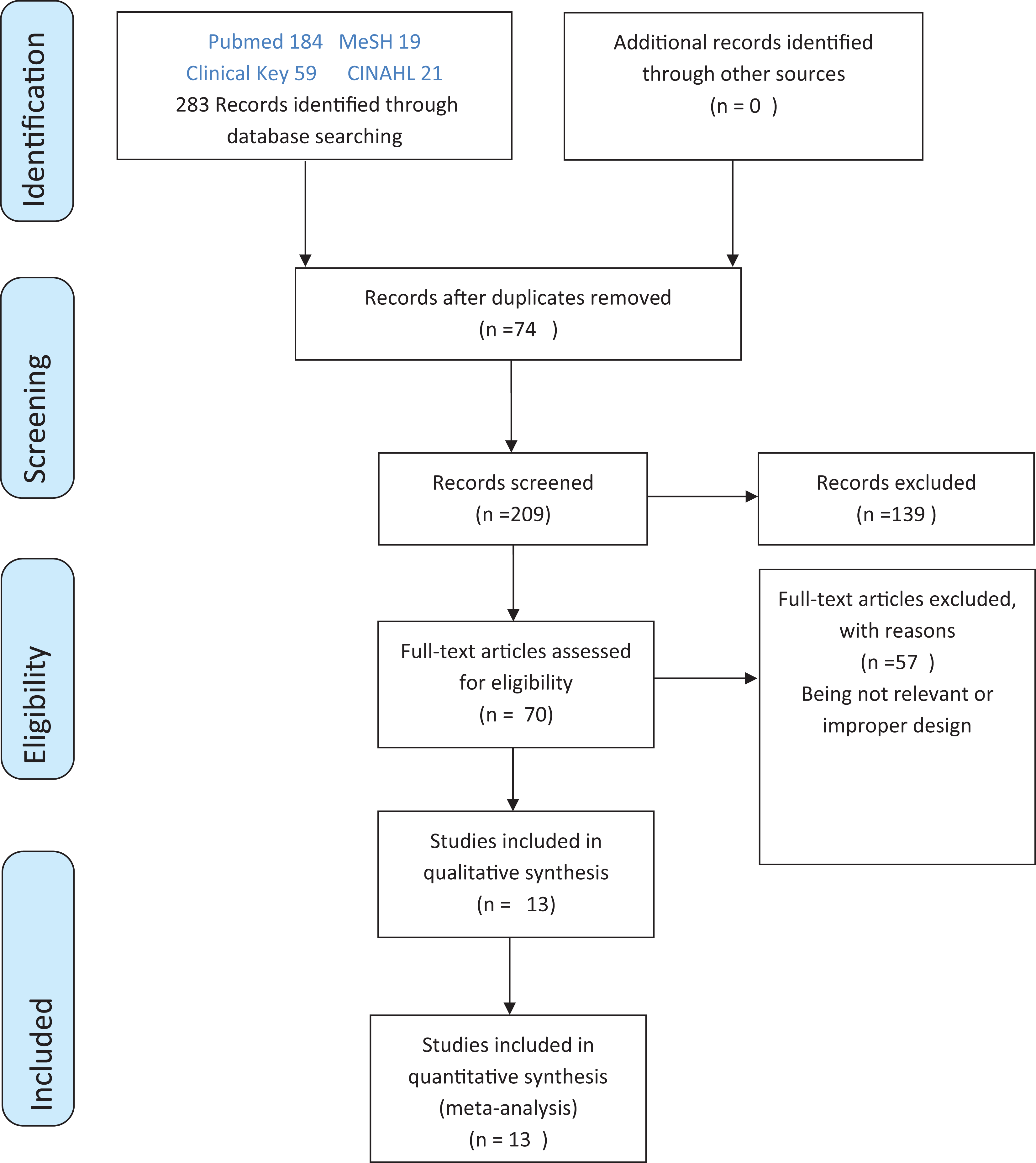
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of study selection and screening.
Baseline Demographic Data of Enrolled Studies
A total of 224 cases were included in our review, and the ages of patients ranged from 16 to 81 years. The number of male patients was only 65 (29.5%). Preoperative immunosuppression administration was reported in 53 (24%) patients. The most common upper airway symptoms were dyspnea, stridor, hoarseness of voice, and cough. Table 1 summarizes the baseline characteristics of our included patient.
Baseline Demographic Data of Included Studies.
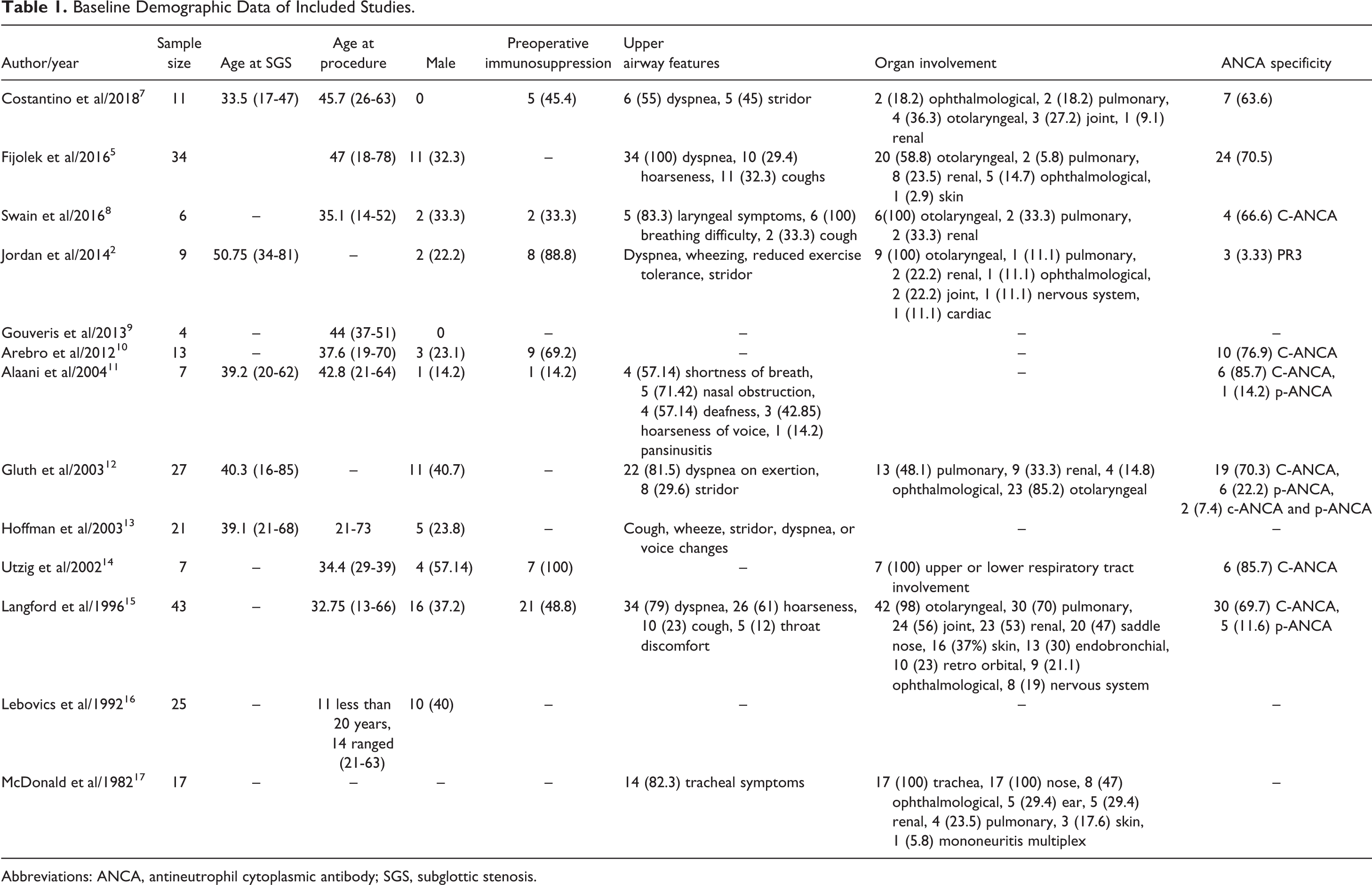
Abbreviations: ANCA, antineutrophil cytoplasmic antibody; SGS, subglottic stenosis.
Open transcervical approach
Open laryngotracheal reconstruction with graft
Based on the included studies, the most common open airway surgery for GPA SGS was laryngotracheal reconstruction (LTR). 2,7,12,16 The majority used costal cartilage for the graft except in one case in which they used pinna cartilage instead. 2 However, not all the studies mentioned their graft type. 16 Moreover, 2 cases underwent LTR with microvascular flap of a rib graft with its intercostal arteries, and they had a good outcome. 16 However, 2 cases underwent LTR and submucosal excision of scar tissue only with no graft. 2 The outcome was favorable in most of the cases with no gross complications. Only one case had an anterior displacement of the graft, which needed an endoscopic intervention. 12 Almost all were performed as a double-stage surgery except 3 cases, which did not need prophylactic tracheostomy 2,7,12,16 (Table 2 ).
Summary of the Outcome of Each Approach.
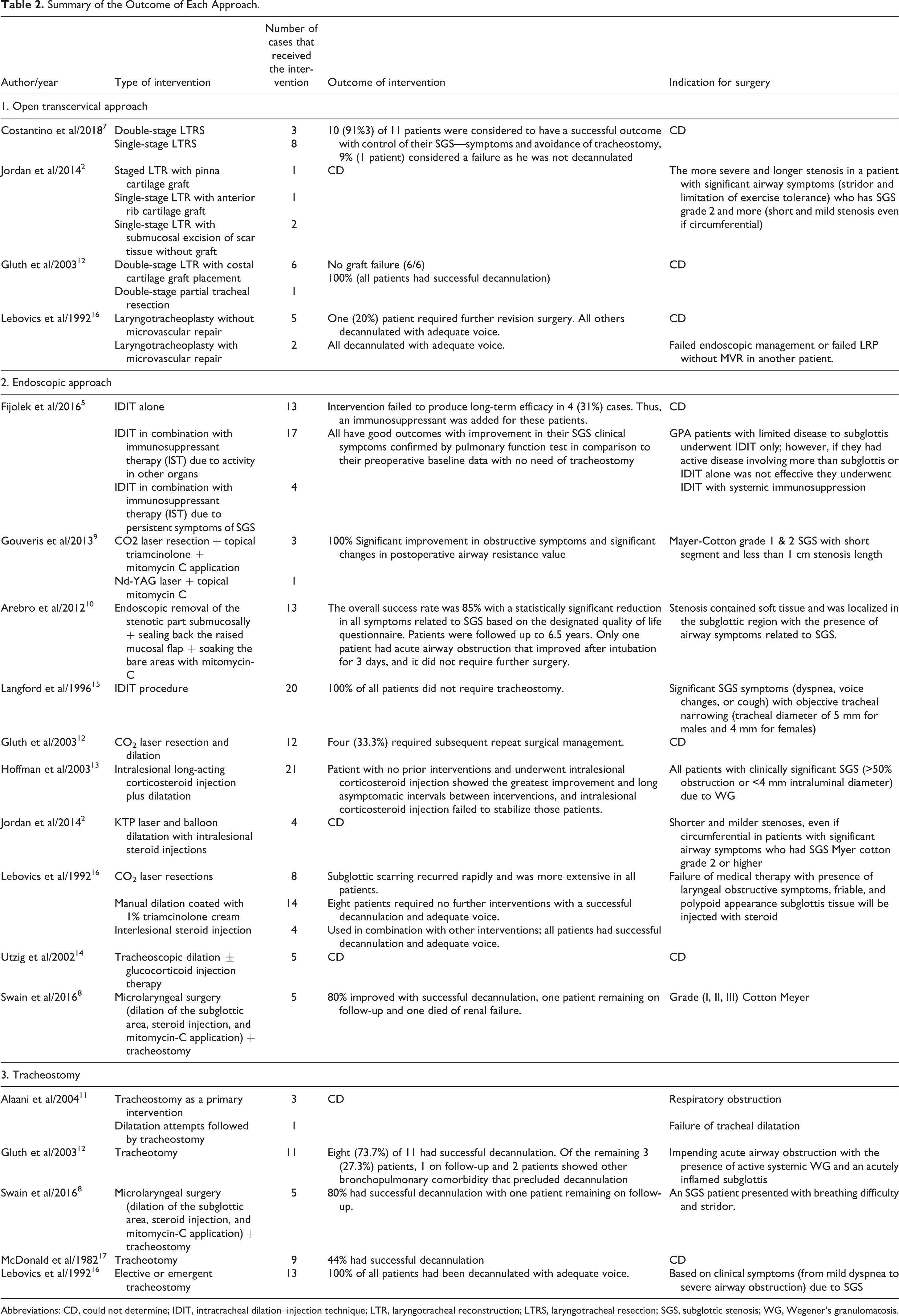
Abbreviations: CD, could not determine; IDIT, intratracheal dilation–injection technique; LTR, laryngotracheal reconstruction; LTRS, laryngotracheal resection; SGS, subglottic stenosis; WG, Wegener’s granulomatosis.
Open laryngotracheal resection without graft
Laryngotracheal resection with primary anastomosis was the surgical modality in 13 of 29 patients who underwent open airway surgery. 7,12 Most of the cases were performed as single-stage surgery except for 3 cases in which the airway edema was anticipated at the level of anastomosis or at the glottis. 7 In all the cases, there were no major complications or deaths; however, 2 patients were reintubated due to airway edema, one patient developed pneumothorax and required thoracotomy, one patient required granulation tissue debridement by bronchoscopy, and one patient developed surgical site infection that required incision and drainage 7 (Table 2 ).
Tracheostomy
Tracheostomy placement alone or combined with other procedures is frequently reported in SGS management. Further details on the results are shown in Table 2 .
Endoscopic approaches to SGS in patients with GPA
Of the 10 studies that addressed the endoscopic interventions of SGS in GPA, dilatation of the subglottic region was the most common approach used; 9 studies utilized the endoscopic balloon for dilatation, and only one study used dilatation tracheostomy for management. 14 Concurrent interlesional steroid injection was applied in all the cases; however, an additional application of mitomycin-C was used in only one study. 8
Resection of the SGS segment with laser surgery combined with topical medication administration was demonstrated in 4 studies, and the most common lasers used included CO2, KTP, and nd-YAG lasers. 2,9,12,16
Endoscopic techniques showed immediate improvement with no requirement for tracheostomy in all the studies. Only a few complications were documented in regard to endoscopic surgeries: cracking in the tracheal mucosa in 2 cases and the pneumothorax in 1 patient. 5,15 In Table 2, we summarize the indication and success rate of all surgical approaches.
Medical Management of SGS in Patients With GPA
Administration of immunosuppressive therapy or cytotoxic drugs is an option for specific cases with or without surgical procedures. Table 3 summarizes the outcomes of therapy and indications of treatment.
Medical Management Applied in the Included studies.
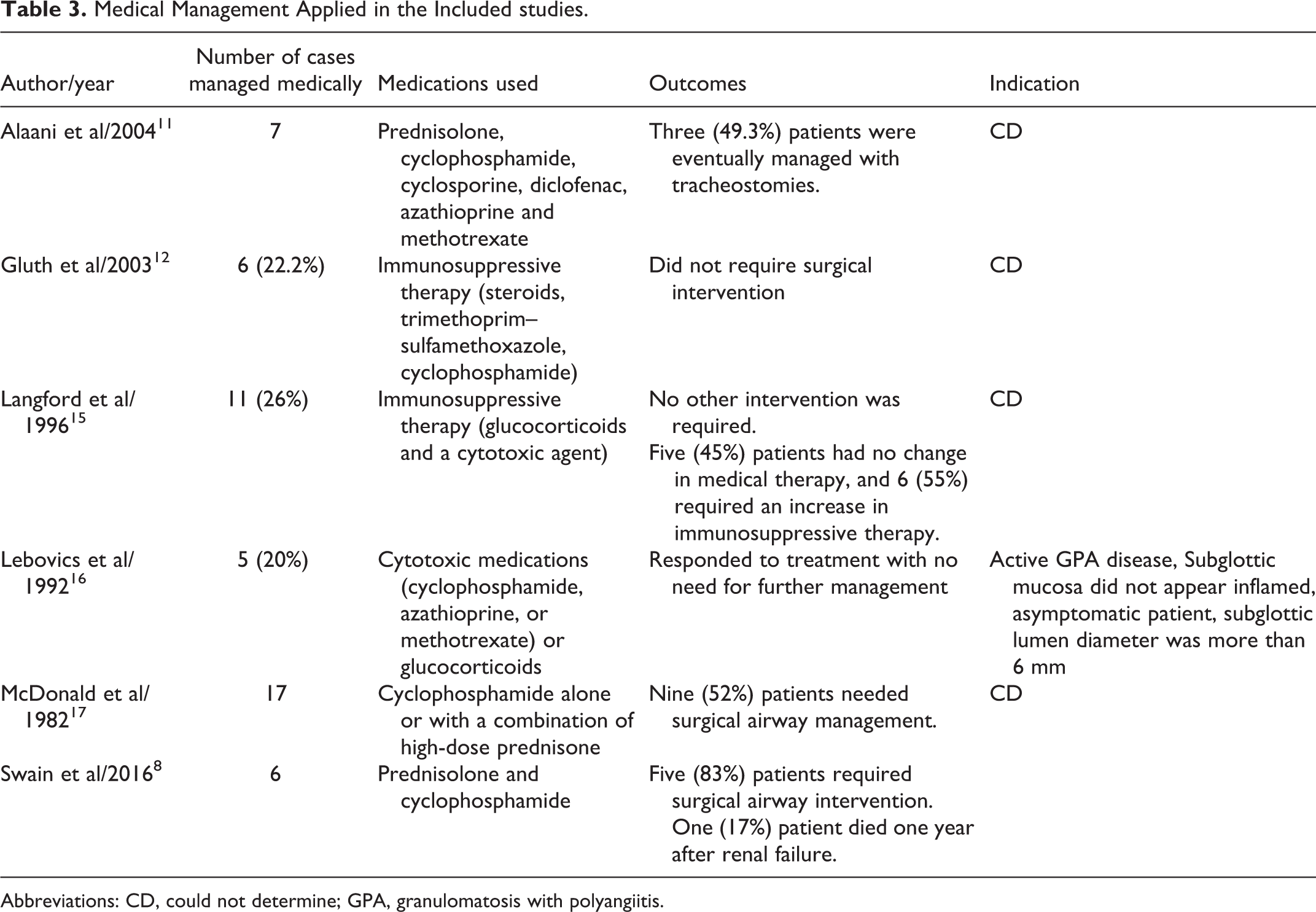
Abbreviations: CD, could not determine; GPA, granulomatosis with polyangiitis.
Discussion
Airway involvement, specifically subglottic lumen, is considered rare but significant complication of GPA. There are different management options that can be offered for each patient depending on the factors as outlined in this review.
Open Airway Surgery
Among the studies, the most frequently mentioned indication is to choose an open surgical approach over other options, which fails for multiple endoscopic dilations. None of the studies mentioned a specific number or description for the number of prior interventions. One study described that their chosen patient should have grade 2 or more in the Cotton-Myer system. 2 Thus, for this management option, the literature is lacking a clear indication to proceed with open surgery in SGS patients.
Open airway surgery has been mentioned to different extents based on the stenosis art of the airway. One study described the removal of the anterior and lateral cricoid cartilage. 7 Another suggested making a cricoid split anteriorly and posteriorly. 16 Further resection of the diseased part in the trachea in the thyroid cartilage was performed in 2 another studies. 2,7 Gluth et al showed a good outcome in a cartilage graft even after reactivation of the disease. 12 One study mentioned 2 patients who underwent LTR with microvascular graft with good outcomes. 16
Open airway surgery carries the risk of airway edema after surgery. Thus, every surgeon should anticipate and plan prior to the procedure to avoid and prevent this complication. 7 Costantino et al reported that 3 patients were reintubated due to airway-transient swelling from a single-staged procedure. 7 Additionally, they reported performing staged surgeries and protecting the airway with tracheostomy in another 3 (27%) patients to avoid airway narrowing. Jordan et al were more conservative against staged surgeries by keeping all patients intubated for 5 days. 2 Based on these, we could not judge whether the outcomes were better with single-stage or double-stage surgeries.
Despite the chronic usage of immunosuppressant medications in GPA patients, postoperative microbial infection has been reported only in 1 (3%) case of a total 29 patients who underwent open airway surgery according to this review. 7 Although this may be limited by the small number of cases, these data suggest that an immunosuppression condition in GPA is not a factor that increases the infection rate postoperatively.
Among the 29 reported procedures for open airway surgery listed in this review, the definition of a successful outcome was either permanent tracheostomy tube decannulation or avoidance of tracheostomy during the follow-up period. Only 2 (7%) patients of 29 reported failure of the open surgical intervention; one patient required revision of the LTR with microvascular flap, and the other patient could not be decannulated. 7,16 Upon comparison of these results with LTR (with and without graft) that were performed due to other pathologies (trauma, intubation, or idiopathic) mentioned in a recent systematic review, we can conclude that GPA will result in a better outcome after surgery, taking into consideration the low number of GPA cases found for our review.
Endoscopic Intervention
Regarding studies that introduced endoscopic interventions, there was dilatation and injection, laser removal of the stenotic part, and direct corticosteroid injection to the lesion. As found in the literature, patients underwent the Intratracheal dilatation–injection technique (IDIT), which was the leading intervention in several studies. 5,13,15 There was better outcomes for most of the patients in regard to long-term median survival, subsequent need for follow-up procedure, and requirement for tracheostomies, as multiple patients were able to be decannulated after using this technique 13 ; however, the best outcomes were achieved in patients who received concurrent systemic immunosuppression. 5,15 Additionally, IDIT as the first intervention without prior surgical interventions (excluding tracheostomy) resulted in better results with a mean number of procedures of 2.4 compared with patients who had previous interventions, which included laser resection or rigid bronchoscopic dilations with a mean number of procedures of 4.1. 13 Conventionally, methylprednisolone is used as a local injection, and mitomycin-C is applied over the stenotic area, and both methods have shown good outcomes. 8
To review another approach for endoscopic intervention was novel procedure was performed in which the stenotic part was removed submucosally, and then, the raised mucosal flap was sealed back with the bare areas soaked with mitomycin-C; here, there was a significant improvement in the quality of life at approximately 85% based on the designated quality of life questionnaire with standardized questions that address postintervention symptom improvement, and there was no postprocedural mortality reported. 10
The use of a CO2 laser in GPA had a vastly different utcomes with very positive results if used with mitomycin-C application. 9,12 However, earlier studies showed that stenosis reoccurred more rapidly and extensively if a laser was used. 16 This might be related to the use of laser while active inflammation is present. 18 Lastly, the indication to use endoscopic interventions has been mostly used in patients with soft SGS, patients scoring on the Cotton-Mayer scale a grade of III or less, 8 lumen obstruction in CT at 80% or less, 13 severe symptoms, or a tracheostomized patient who was to be decannulated, keeping in mind that most of the treatments for the cases were individualized.
Tracheostomy
Tracheostomy was conducted mostly in patients in these studies as a temporary method for patients who were presenting with severe stridor or impending respiratory compromise, and it was mostly done as an emergency measure or as a bridge for definitive intervention. 11,12,16,17 All of the presented patients received concurrent systemic immunosuppressive therapy. There were successful rates of decannulation afterward, which increased in patients who underwent subsequent surgeries that were either endoscopic or with an open approach. In patients who were unable to be decannulated, the disease was fulminant and severe in nature with the presence of concurrent bronchopulmonary disease. 8,11,12
Medical Management
Of note, the SGS course for GPA patients occurs independently from the systemic disease nature. 8,12,19 Some authors suggest that medical treatment alone has a limited role in the long-standing beneficial outcome for isolated SGS in GPA patients. 8,11,14,16,19 However, others have suggested that short stenosis induced by the active disease may be treated by medications. Although scarred stenosis or cases with extensive fibrosis or resistance to systemic immunosuppressive therapy necessitate surgical interventions, 19 some authors have recommended that during active disease status, to avoid airway manipulation, deferring open or endoscopic intervention until optimization of the disease status. 9,12
Finally, our systematic review was subject to several limitations. First, the presence of clinical heterogeneity within the studies in terms of clinical presentation, diagnosis, and management affected the qualitative analysis of the reported findings. The second limitation was relatively small number of included studies with the small number of patients assigned to each technique. Third, the lack of controlled groups and lack of standardized definition of success rate may affect our analyses of these studies. Also, another major limitation was the most included studies were retrospective studies or case series, understanding the rarity of the disease with small number of sample size was also expected. Last but not least, not all the studies showed long-term outcomes with rigorously long follow-up periods.
Conclusion
Although surgery is the mainstay of treatment for GPA-SGS, immunosuppressant therapy plays a role in stabilizing the active disease and thus could enhance the success rate postoperatively. Surgical intervention should be individualized however, and endoscopic balloon dilatation with administration of intralesional steroid injection and topical mitomycin C is the standard initial management for most cases. Open airway surgery has shown favorable outcomes and should be considered for severe SGS that is refractory against endoscopic interventions. Saving the airway is a priority and should be anticipated, and tracheostomy should be performed if needed.
Footnotes
Authors’ Note
All the methods were performed per the relevant approved guidelines, regulations, and declaration of Helsinki. Written informed consent was obtained from the patient to have her details and accompanying images published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.