
Abstract
A myopericytoma in the auricle is rare. If an auricle contains a large, firm, red-brown mass, excision should be considered because the mass may be a myopericytoma. After excision, histopathological and immunohistochemical diagnoses are essential to rule out malignancy. Long-term follow-up is required because the tumor is slow-growing.
A 60-year-old woman visited our Department of Otorhinolaryngology complaining of a slow-growing, left auricular mass. She did not exhibit otalgia or hearing loss. On physical examination, a firm, reddish, non-tender large mass was observed in the left auricle, originating from the antitragus (Figure 1). Neck computed tomography revealed a slightly enhanced, soft tissue-density solid mass, 3 × 2.5 × 2 cm in size, in the left antitragus (Figure 2). The patient requested removal for cosmetic reasons; surgical excision of the suspected vascular tumor was planned.

A firm, reddish, non-tender large mass is observed in the left auricle, originating from the antitragus.
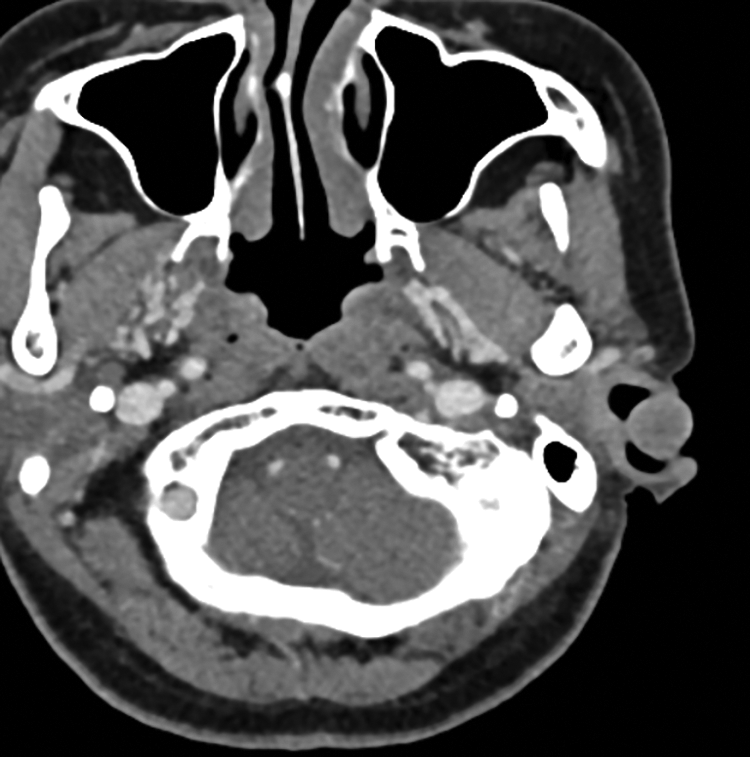
Neck computed tomography reveals a slightly enhanced, soft tissue-density solid mass, 3 × 2.5 × 2 cm in size, in the left antitragus.
With the patient under local anesthesia, the tumor was partially removed with microscope. Histopathological examination of a frozen section revealed a spindle cell neoplasm. The mass was then completely removed. The wound healed well. No recurrence was noted after 9 months.
Microscopically, the tumor was composed of uniform, bland, ovoid-to-plump short spindle cells in the dermis and subcutaneous tissue; the tumor was relatively well demarcated. Characteristic multilayered, concentric perivascular growth was noted. However, no prominent nuclear atypia, overt mitosis, or necrosis were found. Immunohistochemical staining results were positive for smooth muscle actin (SMA) and vimentin; negative for desmin, S100, human melanoma black (HMB) 45, Melan A, cluster of differentiation (CD) 31, CD34, signal transducer and activator of transcription 6, pan-cytokeratin, and epithelial membrane antigen. The histopathological findings and immunohistochemical staining pattern were those of a myopericytoma (Figure 3).
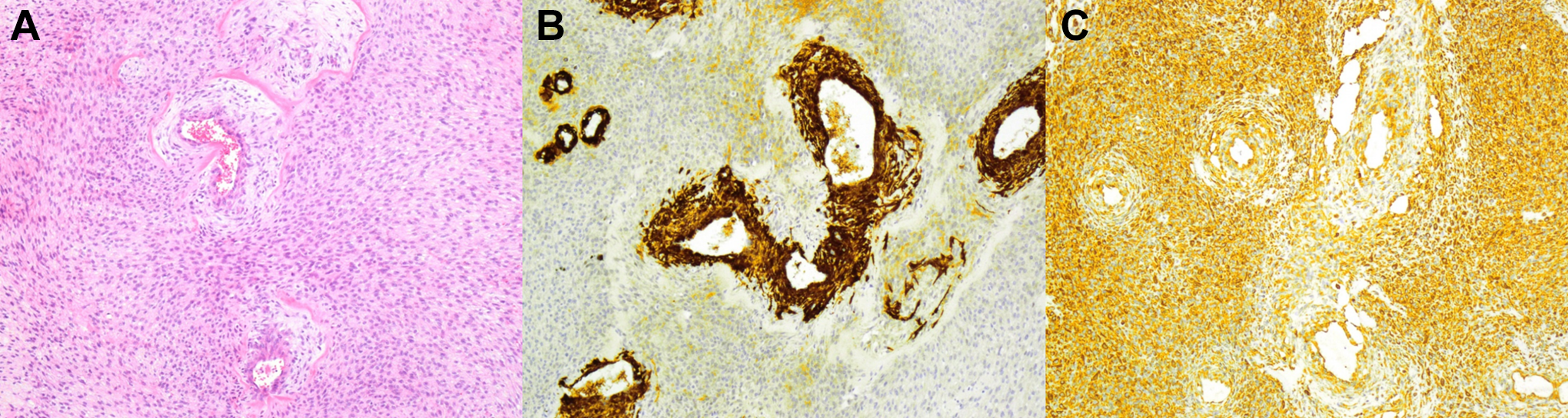
Histopathologic imaging shows that the tumor is composed of homogenous, bland, ovoid-to-round, short spindle cells that exhibit remarkable, multilayered, concentric perivascular growth (hematoxylin–eosin, ×100) (A). Immunohistochemical staining shows that tumor cells are positive for smooth muscle actin (SMA) predominantly in the perivascular area (×200) (B) and diffusely strongly positive for vimentin (×200) (C).
A myopericytoma is a rare, benign, soft tissue neoplasm that exhibits perivascular myoid differentiation.1,2 The tumor typically originates in cutaneous or subcutaneous tissue.1-3 In 2002, the World Health Organization recognized myopericytomas as a subset of perivascular tumors.2-5 Most myopericytomas develop in the lower extremities, followed by the upper extremities; head-and-neck tumors are rare.2-4,6
Myopericytoma was first described by Granter et al in 1998.2,3,5,7 Pericytes, first described by Zimmermann in 1923, 8 are pluripotent cells that differentiate into smooth muscle cells, adipocytes, and osteoblasts.2-4,6 Myopericytes, first described by Dictor et al in 1992, 9 are intermediates between pericytes and vascular smooth muscle cells.4,6 Myopericytomas originate from perivascular myoid cells and exhibit features of smooth muscle and glomus cells.3,4 Myopericytomas are closely related to tumors that exhibit perivascular myoid differentiation, including adult myofibromatoses and glomangiopericytomas.4,6,7
To the best of our knowledge, only 1 myopericytoma originating in the external ear (including the external auditory canal and auricle) has been reported. This is the first report of myopericytoma in the antitragus of the auricle to appear in the English-language literature.
A myopericytoma is a benign slow-growing tumor with a good prognosis. 4 The tumor exhibits a gray/white nodular appearance, is firm, and features red-brown hemorrhagic lesions.3,6 Myopericytoma exhibits male predominance.1-4,6 Mentzel et al analyzed 54 myopericytomas in patients aged 13 to 87 (median, 52 years) years. 6 Most patients lacked symptoms; however, pain, neurological deficits, and motor deficits were reported. 2
Histopathologically, a myopericytoma is characterized by proliferation of round-to-ovoid spindle-shaped cells with eosinophilic cytoplasm in a perivascular concentric pattern.2-4,6-7,10 It shows hemangiopericytoma-like vascular pattern.3,6,7 Immunohistochemically, a myopericytoma is positive for SMA, h-caldesmon, and vimentin; it is typically negative for desmin, CD34, CD68, and S100.2-4,6
Differential diagnosis of myopericytoma, myofibroma, angioleiomyoma, and glomus tumor is important. The histopathological features and immunohistochemical staining pattern of a myopericytoma are helpful. Most myofibromas exhibit a hemangiopericytoma-like vascular pattern. A myofibroma commonly exhibits a biphasic zonation pattern and is often negative for h-caldesmon.3,4,6 An angioleiomyoma is positive for desmin. A glomus tumor usually lacks spindle-shaped cells and typical spinning-off of cells from the vessel.4,6
The treatment of choice is surgical excision; this relieves symptoms and ensures cosmesis. 2 A myopericytoma generally follows a benign clinical course if surgical excision is complete.3,4,6 The recurrence rate is 10% to 20%, presumably attributable to cord extension beyond the principal lesion when the tumor is not encapsulated, multifocal disease and development of a new lesion, or the impossibility of wide excision because of critical structure proximity.2,3
Although most reported patients have exhibited benign disease, a few instances of malignant disease have been described.1-6,10 A malignant myopericytoma exhibits high cellularity, high mitotic index, pleomorphism, and necrosis.1-3,10 Histopathological and immunohistochemical diagnoses are thus mandatory after excision, as is long-term follow-up.
A myopericytoma in the auricle is rare. We completely excised the mass and have noted no recurrence. If an auricle contains a large, firm, red-brown mass, excision should be considered because the mass may be a myopericytoma. After excision, histopathological and immunohistochemical diagnoses are essential to rule out malignancy. Long-term follow-up is required because the tumor is slow-growing.
Footnotes
Authors’ Note
The Institutional Review Board of the National Health Insurance Service Ilsan Hospital exempted the review of this study (NHIMC 2020-06-014).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.