
Abstract
This report describes an atypical presentation of Kimura’s disease (KD) in a 73 year-old male with painless left mandibular masses, localized swelling, and pruritus. Distinct from classic KD manifestations, the patient was an elderly male exhibited no significant serum eosinophilia, while imaging demonstrated inflammatory changes in the submandibular tissues and cervical lymph nodes. Histopathologic and immunohistochemical analyses confirmed KD with IgG4-positive plasmacytosis. This case highlights the importance of considering KD in the differential diagnosis of head and neck tumors, particularly in elderly patients lacking classic biomarkers. Notably, the marked infiltration of IgG4-positive plasma cells in the affected tissue further suggests a potential overlap between KD and IgG4-related disease mechanisms. These findings emphasize the relevance of incorporating atypical cases in the current body of knowledge.
Introduction
Kimura’s disease (KD), also known as eosinophilic lymphogranuloma, is a rare chronic inflammatory disease. Its etiology and pathophysiologic are unknown, and it may be related to allergic reactions caused by parasitic, viral, and fungal infections and insect bites. 1 Clinical symptoms of KD are atypical, presenting as painless subcutaneous nodules on the head and neck. 2 They typically occur in young Asian individuals, but can also affect the elderly. It is typically accompanied with serum eosinophilia and high IgE levels. 3 Biopsy remains the gold standard for diagnosis. Despite being a benign lesion, if ignored, it can be recurrent and locally aggressive. Its inflammatory tendencies and immunologic abnormalities can also be linked to nephrotic syndrome or other systemic comorbidities. Therefore, adequate recognition and proper management of KD are usually required.
Case Report
A 73 year-old Chinese man had a 1 month history of several steadily growing, increasingly pruritic, painless masses in his left submandibular region. The patient denied experiencing any recent infections, night sweats, fever or chills, earache, trauma, and breathing or swallowing difficulties. He had received antibiotics for 10 days at a local hospital, but the mass had not significantly changed. The patient also had no history of asthma, and atopic or other allergic diseases. On physical examination, multiple masses were palpable in the patient’s left submandibular area, the largest being approximately 2 × 3 cm, non-tender, firm, and mobile, with significant swelling of the surrounding tissues.
Computed tomography showed that the left submandibular gland was larger than the contralateral side, with uneven enhancement. Multiple clumped soft-tissue density shadows on the left neck, which were considered as enlarged lymph nodes, and edematous soft tissue changes in the neck’s left and anterior sides (Figure 1a and b). Furthermore, the left submandibular region mass was observed as a high-intensity signal on T1-weighted and T2-weighted images (Figure 1c–f). T-cell spot test for tuberculosis infection was negative. And laboratory markers including blood counts, IgE level, erythrocyte sedimentation rate, and ultrasensitive C-reactive protein were within their respective normal ranges. Inflammatory disease was initially considered. After extended surgical resection, the pathologic diagnosis was KD (Figure 2). At the 1st year postoperative telephone follow-up, the patient had no localized skin itching and no increased mass in the left submandibular region.
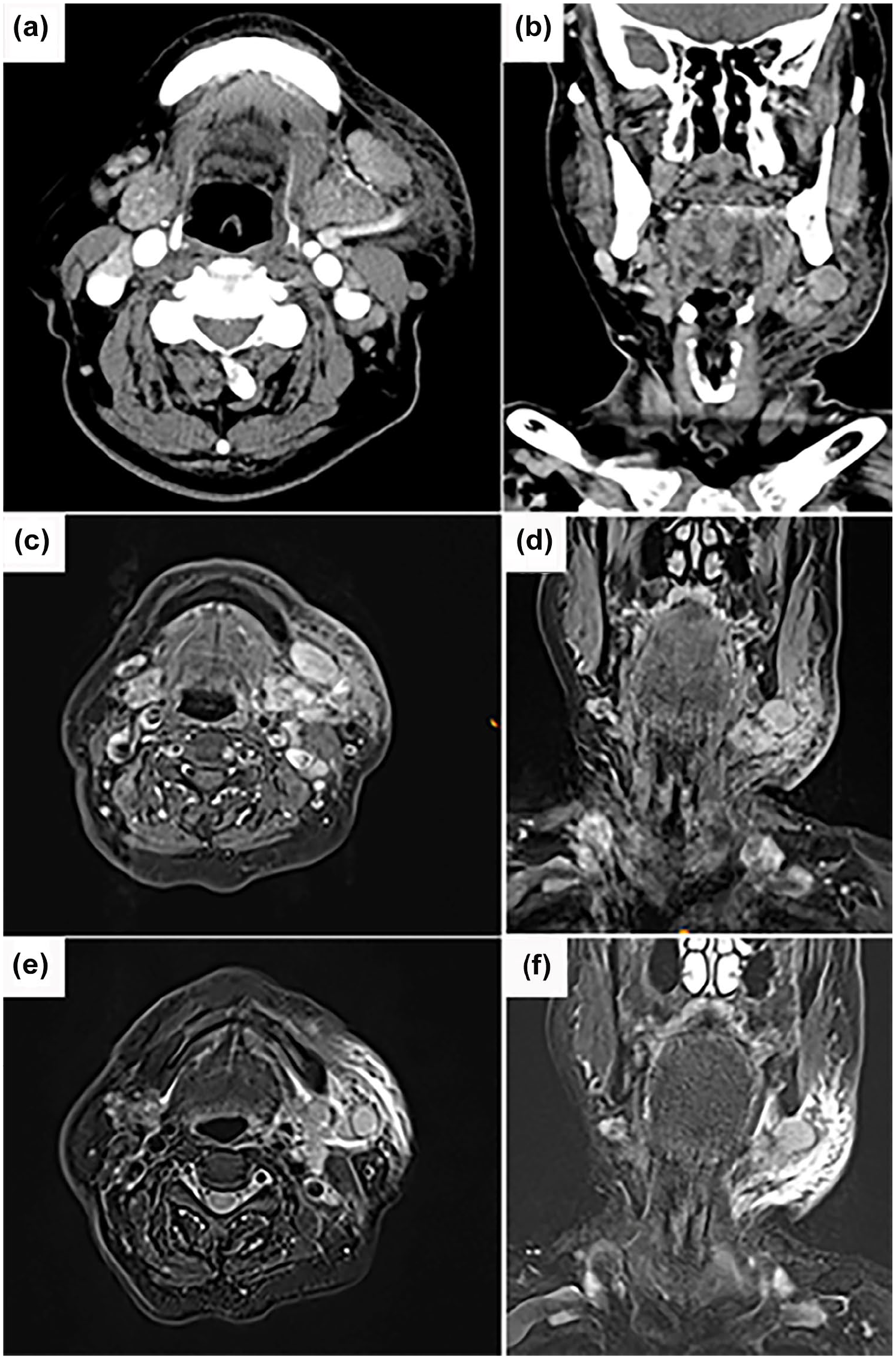
Enhanced CT images show heterogeneous enhancement of the left submandibular region mass with surrounding soft tissue density shadows in axial (a) and coronal positions (b). T1-weighted images (c, d) and T2-weighted images (e, f) show high intensity signal.
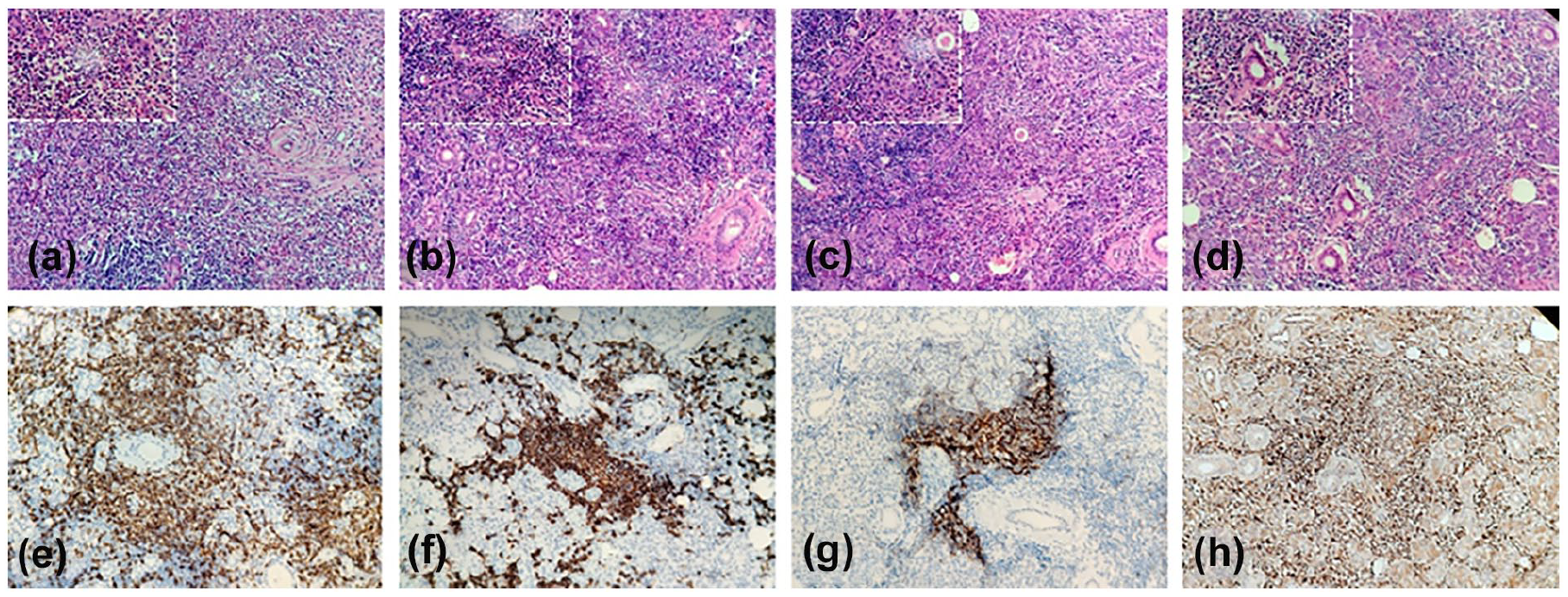
Hematoxylin and eosin staining showing lymphoid follicular hyperplasia with enlarged germinal centers, eosinophilic infiltration in the interfollicular zone, and formation of an eosinophilic abscess (a–d), with a partial enlargement in the upper left corner. The immunohistochemical staining was positivity for CD3 (e), CD20 (f), CD21 (g), and IgG (h). Magnification: 200×.
Discussion
KD is a rare disease with no standardized diagnostic criteria. After reviewing the previous literature,1,3-5 we summarized the following clinical features of KD: high prevalence in Asian males aged 30 to 50 years, lesions presenting as painless subcutaneous masses in the head and neck, increased serum IgE and peripheral eosinophilia, and a limited role of imaging in KD diagnosis. Histopathology can clarify the diagnosis, which typically shows vascularization, necrosis, protein deposition, and eosinophilic microcysts. KD has historically been misdiagnosed as angiolymphoid hyperplasia with eosinophilia. However, we describe a case of KD whose specifics differ significantly from the traditional description.
Generally, KD predominantly affects young men. However, it has also been documented in individuals beyond the age of 60, and elderly patients are more likely to be female. 6 It is noteworthy that pruritus increases with age, which may be related to the deficiencies in humoral and cellular immune function that we present in elderly patients, as in the case we present. 7 Furthermore, it was demonstrated that there were no appreciable variations between age groups in terms of symptom frequency, anatomical distribution, laterality, complications, multiplicity, maximum size, serum eosinophil count, serum IgE level, initial treatment, or recurrence. 7 Thus, the complexity of influencing factors with advancing age may contribute to an atypical course of the disease.
Furthermore, recent studies highlight that type 2 inflammation is a key factor in the development of KD, driven by Th2 cytokines that activate eosinophils and lead to excessive IgE production. Histologically, KD is defined by intact lymph node structure accompanied by eosinophilic microabscesses and infiltration of germinal centers. These observations collectively indicate that eosinophils likely contribute significantly to KD pathogenesis. 8 But not all patients exhibit eosinophilia. Our case, for instance, was not eosinophilic. Zhang et al analyzed the laboratory results of 20 Chinese patients with KD and discovered that 25% had no high peripheral blood eosinophils. 9 And it has been found that infiltrating eosinophils were activated in KD patients, leading to the release of eosinophil cationic protein (ECP). The detection of ECP suggests that it can be used as another parameter of disease activity. Nevertheless, this study found no link between ECP levels and eosinophil count. This suggests that eosinophil count may fluctuate with disease fluctuations. 8 Consequently, normal eosinophil levels in laboratory tests do not exclude KD, and biopsy of the lesion site is the definitive way to determine the nature of the lesion.
Another puzzling point is our case exhibited characteristics of IgG4-related disease (IgG4-RD) on histological investigation. Since Tsubouchi et al discovered abundant IgG4-positive plasma cells in lung biopsy specimens of KD patients, a link between KD and IgG4-RD has been proposed not only in otolaryngology but also in other fields including skin and orbital lesions. 10 Meanwhile, KD characteristics have also been noted in IgG4-RD. 11 Based on these results, can it be assumed that KD and IgG4-RD belong to the same class of related disorders? Liu et al postulated that IgG4-RD may represent an epiphenomenon of KD, and IgG4-RD clinical symptoms may be brought on by a sequence of immunological responses brought on by long-term exposure to allergens in KD patients. 12 Therefore, it is challenging to categorize them as entirely-distinct illnesses. IgG4 and KD could be seen as components of a clinical spectrum of aberrant immune responses. 5
Although KD is a benign condition, it is prone to recurrence. 13 Available clinical treatments include surgical resection, radiotherapy, oral corticosteroids, cyclosporine, targeted therapy, and systemic immunosuppression.2,13 Notably, recent advances in biologic therapies, such as anti-IL-5 agents like mepolizumab, show promise for refractory KD by targeting eosinophil-mediated inflammation. In terms of outcomes, the overall recurrence rate for surgical resection was 30.5%, which decreased to 26.94% with adjuvant therapy. 2 Nevertheless, surgery remains the initial choice and is essential to the pathological diagnosis of KD. But the operative boundaries were sometimes unclear for wide excision, especially in infiltrative lesions. Positive margins were shown to be one of the hazards associated with a high recurrence rate. To further address the issue, a meta-analysis revealed that disease duration, definition of lesion boundaries, blood eosinophil count, IgE level, presence of single or multiple lesions, and lesion size were associated with KD recurrence. 2 Then, adjuvant therapy should intervene to reinforce the control of recurrence.
Conclusion
KD is an uncommon chronic inflammatory disease that usually occurs in young adults but also affects the elderly. In addition to malignancy, KD should be considered when evaluating head and neck masses in elderly patients, especially in the presence of eosinophilia and elevated IgE levels. Confirmation of the diagnosis depends on biopsy, and attention should be paid to aggregates of IgG4-positive plasma cells, which may require IgG4-RD screening. Surgery is the mainstay of treatment, often combined with hormonal or radiation therapy to minimize recurrence.
Footnotes
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.