
Abstract
This case involved a 21-year-old male patient who was admitted due to having a lump behind the left ear that had been present for 2 years and had gradually increased in size for over a year. This was accompanied by palpable hard masses on the same side of the neck. Laboratory tests indicated an elevated eosinophil count, and magnetic resonance imaging confirmed the “string-of-beads” sign in the left cervical lymph nodes. Fine-needle aspiration cytology prior to surgery revealed reactive lymphoid hyperplasia with eosinophils. Ultimately, surgical excision confirmed the diagnosis of Kimura’s disease. Following glucocorticoid treatment, the patient was monitored, and no new masses were detected during 7-months follow-up period.
Introduction
Kimura’s disease (KD) is a rare and chronic inflammatory disorder that predominantly affects young males and is characterized by lymphadenopathy. 2 The diagnosis of KD involves clinical and histopathological features, including peripheral blood eosinophilia and elevated levels of immunoglobulin E (IgE). 5 Treatment options include glucocorticoids, immunosuppressants, radiotherapy and surgery. 10 Glucocorticoids primarily target autoimmunity, while immunosuppressants modulate specific pathways. Radiotherapy is recommended for specific cases, while surgery is effective for localized lesions. A combined treatment approach may reduce relapse rates and improve patient outcomes. 14
Case Summary
General Information
A 21-year-old male patient was admitted to our hospital due to the presence of a lump behind the left ear for 2 years, which had gradually increased in size over the past year. The patient reported that approximately 2 years ago, he discovered a lump behind his left ear by chance, which was approximately 1 cm in diameter and round in shape. A local county hospital diagnosed this lump as a lipoma, but no treatment was administered. Over the past year, the patient noted that the lump had progressively increased in size and currently measured approximately 4 cm in diameter, maintaining a round shape, with no tenderness. The overlying skin showed no redness, ulceration or discharge. The patient denied experiencing any fever, cough, sputum production, oral ulcers, dry eyes, dry mouth, photosensitivity, joint pain, or lower limb edema. The patient was admitted for a definitive diagnosis. The past medical history, personal history, and family history were unremarkable. Written informed consent was obtained from the patient for the publication of this case report.
Examination
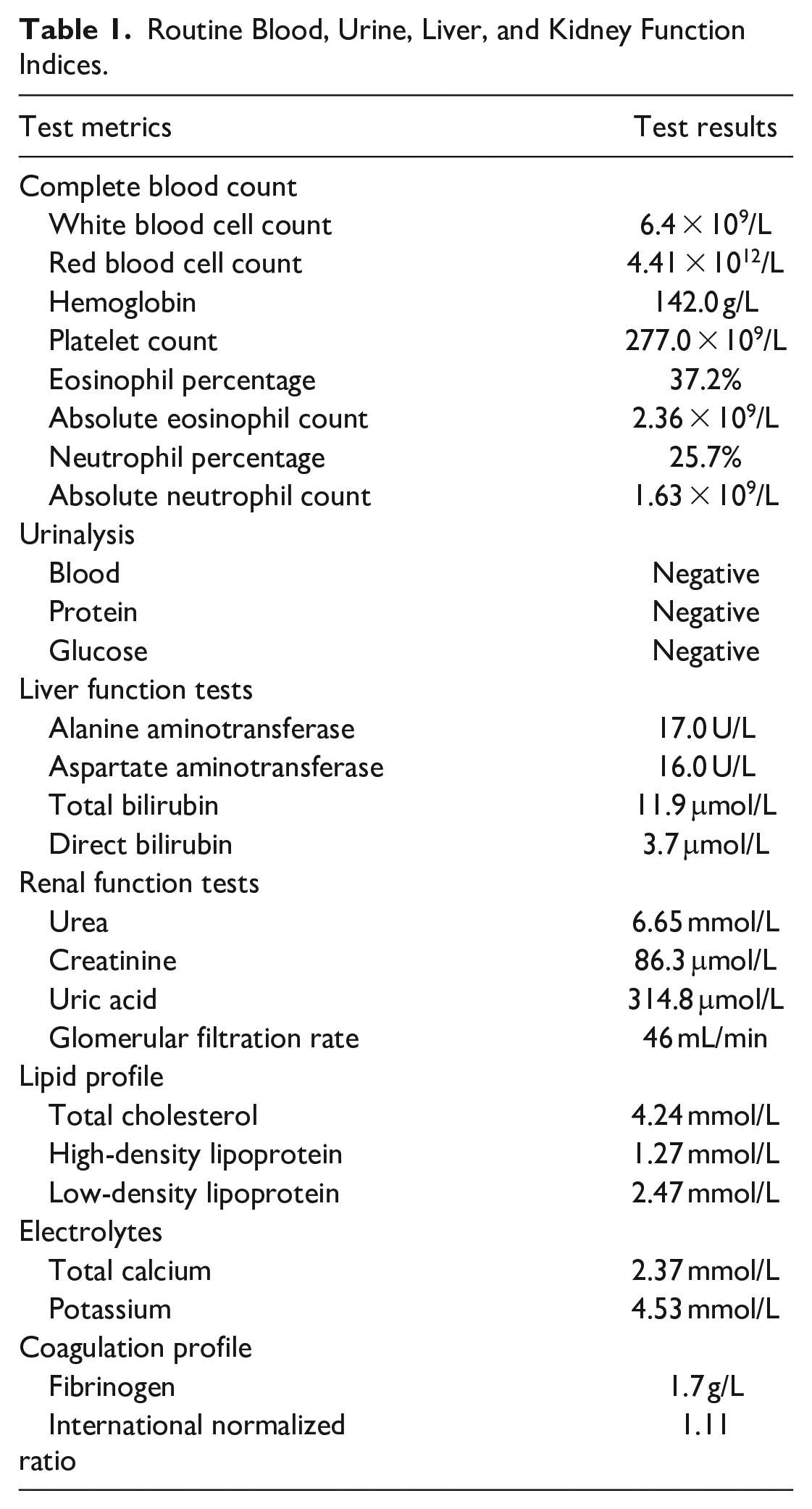
Upon physical examination, the patient’s temperature was 36°C, the pulse was 86 beats/minute, the respiratory rate was 20 breaths/minute, and the blood pressure was 120/78 mmHg (1 mmHg = 0.133 kPa). The patient was alert, with a normal appearance, and the skin and sclera showed no evidence of jaundice. Multiple palpable soft masses were noted behind the left ear, with the largest diameter approximately 4 cm; these masses were well-defined, round, firm in consistency, and nontender. The overlying skin exhibited no redness, ulceration, or exudation. Upon examination of the left cervical region, multiple enlarged lymph nodes of varying sizes were palpated along the posterior border of the sternocleidomastoid muscle in the left neck, exhibiting a string-of-beads sign, with the largest node measuring approximately 3 cm in diameter; this node was well-defined, firm, mobile, and nontender. There was no pitting edema in either lower limb. Routine indicators for blood, urine, and liver/kidney function are shown in Table 1. We found a significant increase in both the absolute eosinophil count (2.36 × 109/L) and the percentage of eosinophils (25.7%). The urinary protein content was negative, and the urine was negative for red blood cells. Serum creatinine levels were within the normal range (Creatinine: 86.3 μmol/L). This led us to understand that the localized lymphadenopathy might be due to an immune-mediated chronic inflammatory disease, with no current impairment of kidney function, raising our suspicion for KD. Subsequently, we performed further magnetic resonance imaging (MRI) examinations and pathological biopsy.
Routine Blood, Urine, Liver, and Kidney Function Indices.
MRI revealed a mass of approximately 28 × 12 × 11 mm with heterogeneous long T1 and T2 signals behind the left ear, and an increased number of enlarged lymph nodes in the left cervical region (Figure 1A-D). Lymph node biopsy revealed reactive lymphoid hyperplasia with eosinophilic infiltration and reactive lymphoid hyperplasia with an increased proportion of eosinophils (Figure 1E,F). Postoperative pathology revealed a left postauricular mass. Lymphoid follicle hyperplasia was also observed, with local accumulation of salivary gland tissue (Figure 1G). With regards to the left cervical lymph nodes, lymphoid follicle hyperplasia was noted, with the formation of eosinophilic “micro-abscesses” accompanied by hyperplasia of high endothelial venules. These findings were consistent with the pathological features of KD, leading to a diagnosis of KD (Figure 1H,I).
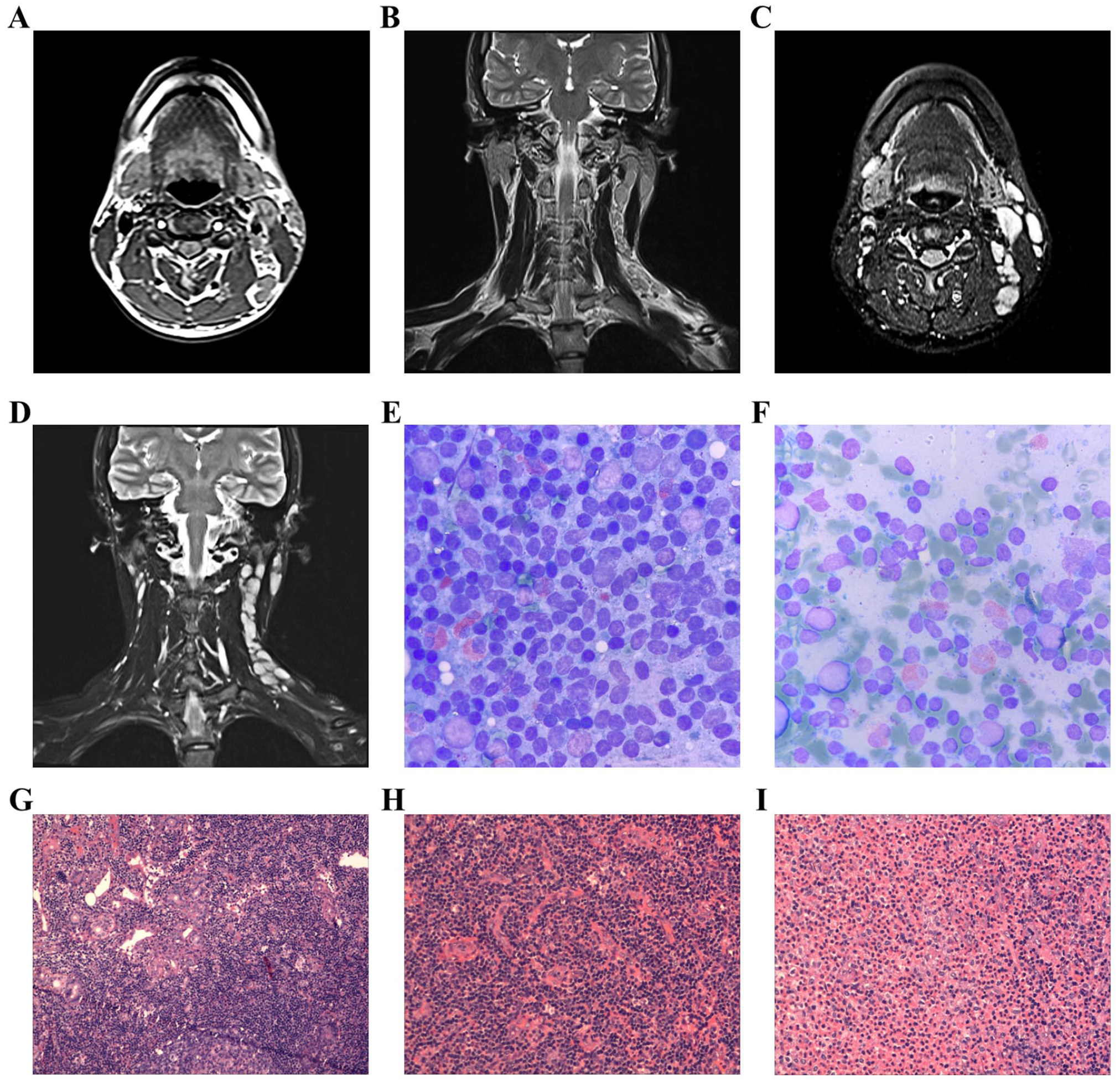
MRI and pathological examination of a 21-year-old male with KD. (A) T1 signal on MRI; (B) T1 long signal on MRI; (C) T2 signal on MRI; (D) T2 long signal on MRI; (E) Biopsy of the left cervical lymph node (Wright–Giemsa stain, 10×100 magnification); (F) Biopsy of the lump behind the left ear (Wright–Giemsa stain, 10×100 magnification); (G) Postauricular mass showing lymphoid tissue in a fibro-fatty tissue, with lymphoid follicle hyperplasia and the local involvement of the salivary gland (HE, ×100); (H) Lymph node removed the neck showing lymph node tissue, high endothelial venules hyperplasia in lymph node tissue (HE, ×200); (I) Lymph nodes removed from the neck showing lymph node tissue, lymphoid follicle hyperplasia, and the formation of small abscesses with eosinophils (HE, ×200). HE, hematoxylin and eosin; KD, Kimura’s disease; MRI, magnetic resonance imaging.
Treatment
The patient was young, with a large area of involvement and multiple foci. Complete surgical excision would have resulted in substantial trauma and could have led to dysfunction in neck mobility. If treated solely with corticosteroids, there would have been a high likelihood of recurrence. Therefore, the selected approach was a combination of surgical treatment and postoperative corticosteroid therapy. During surgery, a localized mass was found in the left postauricular mastoid region, with some adhesion to the inferior margin of the parotid gland. Adhesions were also noted in the midsection of the left sternocleidomastoid muscle, and enlarged lymph nodes adhered to its medial side. An ultrasonic knife was used to excise some isolated, minimally infiltrating, and function-preserving diseased tissue during the procedure; thus, ensuring that the normal structure and appearance of the neck were maintained. Postoperatively, the patient received a sodium piperacillin 4 g IV drip (bid) for infection control and dexamethasone sodium phosphate 10 mg/day via IV drip for 5 days, followed by a gradual tapering off to prevent enlargement of the residual lesions or the emergence of new tumors. We recommended that the patient should receive combined radiotherapy and immunosuppressive therapy at a higher-level hospital. Subsequently, a follow-up phone call revealed that the patient had not undergone the recommended postoperative radiotherapy or immunotherapy for unknown reasons. Currently, the patient’s condition is stable, with no new tumors and no enlargement of the residual mass.
Discussion
KD is a chronic inflammatory disease of unknown etiology that typically affects young males and is characterized by lymphadenopathy. While most reported cases are from Asian populations, sporadic cases have also been reported in non-Asian populations. 1 KD typically presents as asymptomatic unilateral soft tissue masses in the head and neck region, often involving the subcutaneous tissues, major salivary glands, and lymph nodes, 2 with reported involvement of the orbit and inguinal region. 3 This disease is predominant in males 20 to 30 years-of-age, and the head and neck are the most commonly affected sites (63% of all patients); only 13% of patients present with inguinal lymphadenopathy. 4 In addition, KD usually involves the kidneys and the skin and usually manifests as nephrotic syndrome, pruritus, or rash, respectively. 5 Our patient presented within the typical age range for KD onset. Hepatic and renal functions were normal, with no significant pruritus or rash. However, a unique presentation was observed: multiple enlarged lymph nodes of varying sizes were palpated along the posterior border of the left sternocleidomastoid muscle in a beaded pattern.
Previous studies have demonstrated that the levels of numerous factors, including granulocyte-macrophage colony-stimulating factor, tumor necrosis factor-alpha, and soluble interleukin-2 receptor, are significantly increased in patients with KD, thus suggesting a potential role for helper T cells in the pathogenesis of KD. 6 Previous statistical studies have found that although KD predominantly affects males, the male-to-female ratio gradually declines with age. Furthermore, pruritus is more commonly observed in older patients, and the diagnosis of KD in elderly patients often takes longer due to the lack of characteristic presentations in this age group. 7 The diagnosis of KD is primarily based on clinical and histopathological features, including eosinophilia in the peripheral blood, elevated serum levels of IgE, and lymphoid hyperplasia with eosinophilic infiltration observed by microscopy. 5 The imaging manifestations of KD appear as regular or irregular nodules or masses with uniform density. MRI shows iso-intensity on T1-weighted imaging and slightly high or high intensity on T2-weighted imaging and proton density-weighted imaging. 8 Our case was previously diagnosed with a lipoma at another hospital. After admission at our hospital, we found a significant increase in both absolute eosinophil count and percentage of eosinophils, and suspected KD in combination with other clinical features; ultimately, a definitive diagnosis was achieved by MRI examination and histopathological findings.
Our patient presented with lymphadenopathy without systemic manifestations but with normal levels of serum creatinine and urine protein levels. However, as this disease progresses, it may damage the kidney, with membranous glomerulonephritis being the most common histopathological pattern. 9 Due to the lack of large-scale systemic clinical trials, no consensus has been established regarding the optimal treatment for KD. 4
Various treatment options have been proposed for KD, including glucocorticoids, immunosuppressants, radiotherapy, and surgery. 10 Glucocorticoids play an important role in the treatment of KD because they are associated with autoimmunity. Some patients may benefit from oral or local glucocorticoid therapy to reduce lymphadenopathy and inflammation. However, reliance solely on corticosteroid therapy may result in relapse upon discontinuation. 11 Immunosuppressants can also be administered for some patients. Radiotherapy has been shown to be suitable for patients with incomplete resection, recurrence, steroid-resistant lesions, or lesions that are too large or difficult to remove surgically. Several studies have reported that patients receiving radiotherapy show a higher relapse rate compared to those treated with glucocorticoids alone. 9 Surgery is a simple and effective treatment option for patients with localized lesions measuring <3 cm in diameter. Surgery can be considered for lesions that severely affect a patient’s quality-of-life or tend to be malignant. However, extensive or infiltrative lesions may be incompletely excised, and aggressive resection without considering specific consequences may influence a patient’s appearance and physiological functionality. 6 Patients who cannot undergo excision or have positive margins, as well as those with risk factors for recurrence, may require postoperative radiotherapy and systemic immunosuppressive therapy. 10 The combination of surgery and radiotherapy leads to a lower rate of relapse compared with surgical excision alone or surgical excision followed by oral corticosteroids. 12
Previous researchers have suggested that treatment with dupilumab, with an initial dose of 600 mg followed by 300 mg every 2 weeks, results in good efficacy and tolerance. In one study, all patients achieved significant therapeutic effects after treatment, with no relapses during a mean follow-up period of 10.4 months. 13 Individualized treatment, incorporating different modalities, appears to be the optimal approach for managing KD. In a previous meta-analysis of 31 studies, the independent relapse rates for surgery, medical therapy, and the combination of surgery with postoperative adjuvant therapy, were 30.5%, 45%, and 26.94%, respectively. 14 In our case, we employed a combination of surgical treatment and postoperative corticosteroid therapy. At follow-up, the patient showed no new tumors and no enlargement of the residual mass.
KD is a chronic disease with a long course and high recurrence rate. The rareness and atypical presentations of KD make early diagnosis and treatment difficult. Our unique case may provide further clinical guidance to clinicians. In the future, multidisciplinary teams should pay more attention to collecting clinical data to study the precise etiology of KD.
Conclusion
In our patient, the surgical excision of a biopsy specimen played a vital role in confirming the diagnosis of KD. In this case, the lymphoid tissue was extensively involved, and there were severe adhesions. The treatment consisted of a combination of surgery and hormone therapy. Surgical excision was performed to remove some isolated, superficially infiltrating lymphoid tissue while preserving normal anatomical structure and function. The residual lesions were subsequently treated with corticosteroids, resulting in a good prognosis, with no enlargement of the residual lesions and no new tumors developed.
Footnotes
Acknowledgements
None.
Author Contributions
Y.G. wrote the draft of the manuscript, Y.G. and H.Y. contributed to the examination and treatment, Y.Z. reviewed the manuscript, all authors approved the final version of the manuscript.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Ethical approval to report this case was obtained from the Ethics committee of People’s Hospital of jingshan (2024034).
Informed Consent/Patient Consent
Written informed consent was obtained from the individual.
Trial Registration Number
Not applicable.
Grant Number
Not applicable.