
Abstract
Mid-glottic webs are a rare pathology of the vocal folds, with cases only documented within the last decade. The pathophysiology behind the location of this vocal fold lesion may be attributed to the mid-vocal fold being the site of maximal mechanical stress during phonation. While anterior glottic webs and posterior glottic stenosis are well-described vocal fold pathologies, only 4 cases of mid-membranous webs have been reported to date. We present the first case of a mid-glottic web not attributable to smoking, radiation, or intubation, in a 45-year-old female teacher who developed chronic dysphonia in the setting of occupational voice use and prior upper respiratory tract infection. She was treated surgically with cold instrument lysis of the adhesion via microdirect laryngoscopy. Her dysphonia improved without residual web at her 4-month postoperative visit, but she did develop vocal fold nodules. A thorough evaluation of acute dysphonia and dyspnea in heavy voice users should include a workup for this rare laryngeal pathology, particularly given its significant negative impact on the ability of occupational voice users to work, followed by proper postoperative voice therapy and vocal hygiene.
Introduction
Glottic webs are usually found anteriorly, known as anterior glottic webs, and can be congenital or acquired. 1 Another well-documented acquired vocal fold pathology is posterior glottic scarring, known as posterior glottic stenosis. 2 In contrast, mid-membranous vocal fold webs are exceedingly rare, with only 4 cases currently reported. 3 The first documented case of an acquired laryngeal web was in 1921 in a 56-year-old male who underwent surgical excision of a left vocal fold carcinoma. 4 Since then, most anterior glottic webs have been iatrogenic from surgery or intubation, with some acquired from laryngopharyngeal reflux, autoimmune diseases, or chemoradiation. 1 While posterior glottic stenosis is most commonly due to prolonged intubation, there is no established etiology for mid-membranous webs.2,3 Dominguez et al hypothesized that a traumatic event leads to mid-vocal fold mucosa denudation and subsequent granuloma formation. 3 We report an acquired mid-glottic web in a patient with occupational voice use and upper respiratory infection (URI), which is the first known case in a patient without smoking, radiation, or recent intubation history.
Case Presentation
A 45-year-old female teacher with a URI and cough presented to a community provider with sudden-onset dysphonia, incited by reading a book to her kindergarten students. She was prescribed 3 days of vocal rest and referred to an outside otolaryngologist, who treated her for presumed reflux. Dysphonia and dyspnea persisted, so she was referred to our tertiary medical center 9 months later, where she was found to have a mid-vocal fold web. She did not have a history of laryngeal surgery, trauma, recent intubations, or rheumatologic conditions. Laryngostroboscopy revealed a broad, thin web between the mid-membranous true folds with a normal anterior commissure and posterior glottis (Figures 1A and 2A and B). She underwent surgical excision with microdirect laryngoscopy and cold instrumentation lysis of the adhesion, followed by injection of 40 mg/mL of triamcinolone acetonide (Figure 1B). At her 3-week postoperative visit, her vocal folds were well-healed with trace scarring on the right vocal fold without residual web or adhesion (Figure 2C), and she was referred to voice therapy. At her 4-month postoperative visit, she had normal vocal fold mobility without residual webbing but had not undergone voice therapy and developed bilateral vocal fold nodules. She was re-referred to voice therapy and counseled on proper vocal hygiene, including voice rest when feasible.
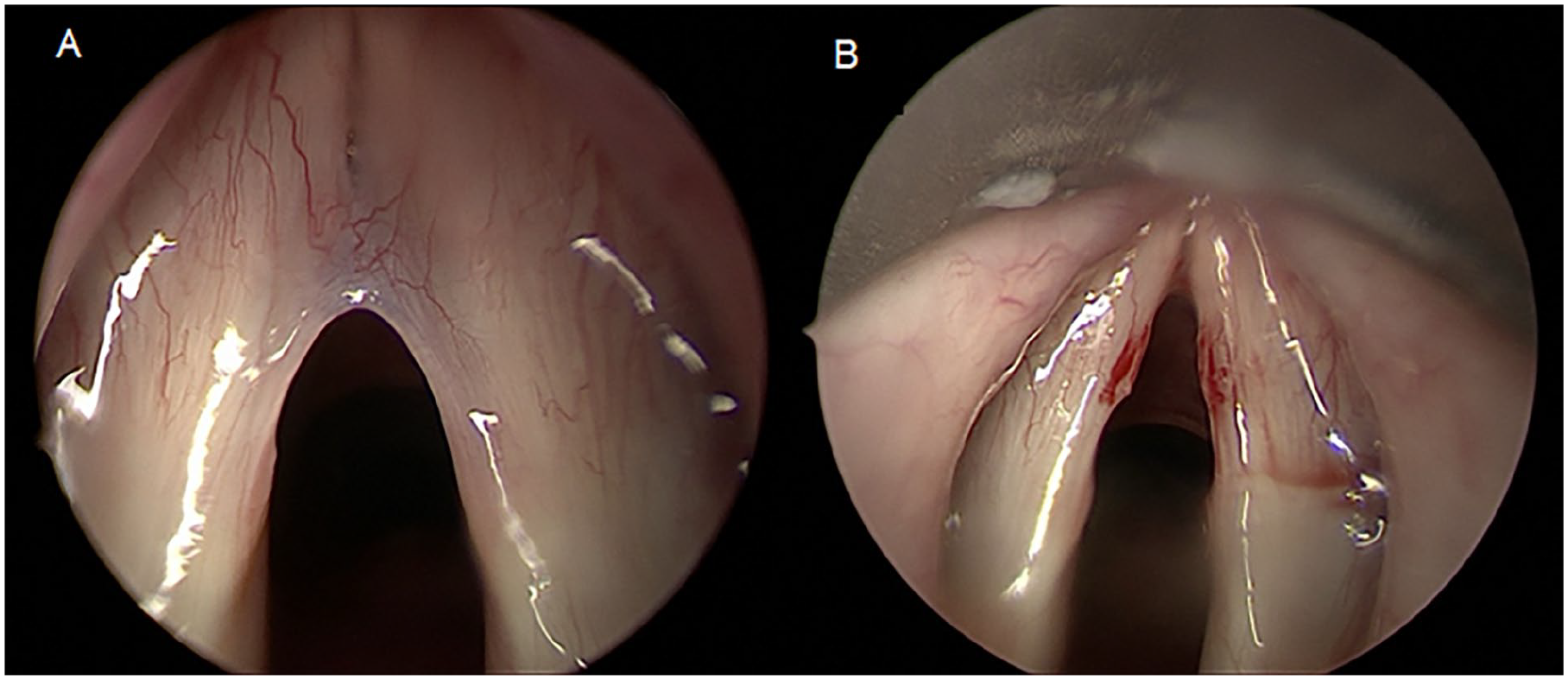
Intraoperative view of mid-membranous glottic web (A) and after cold instrumentation lysis (B).
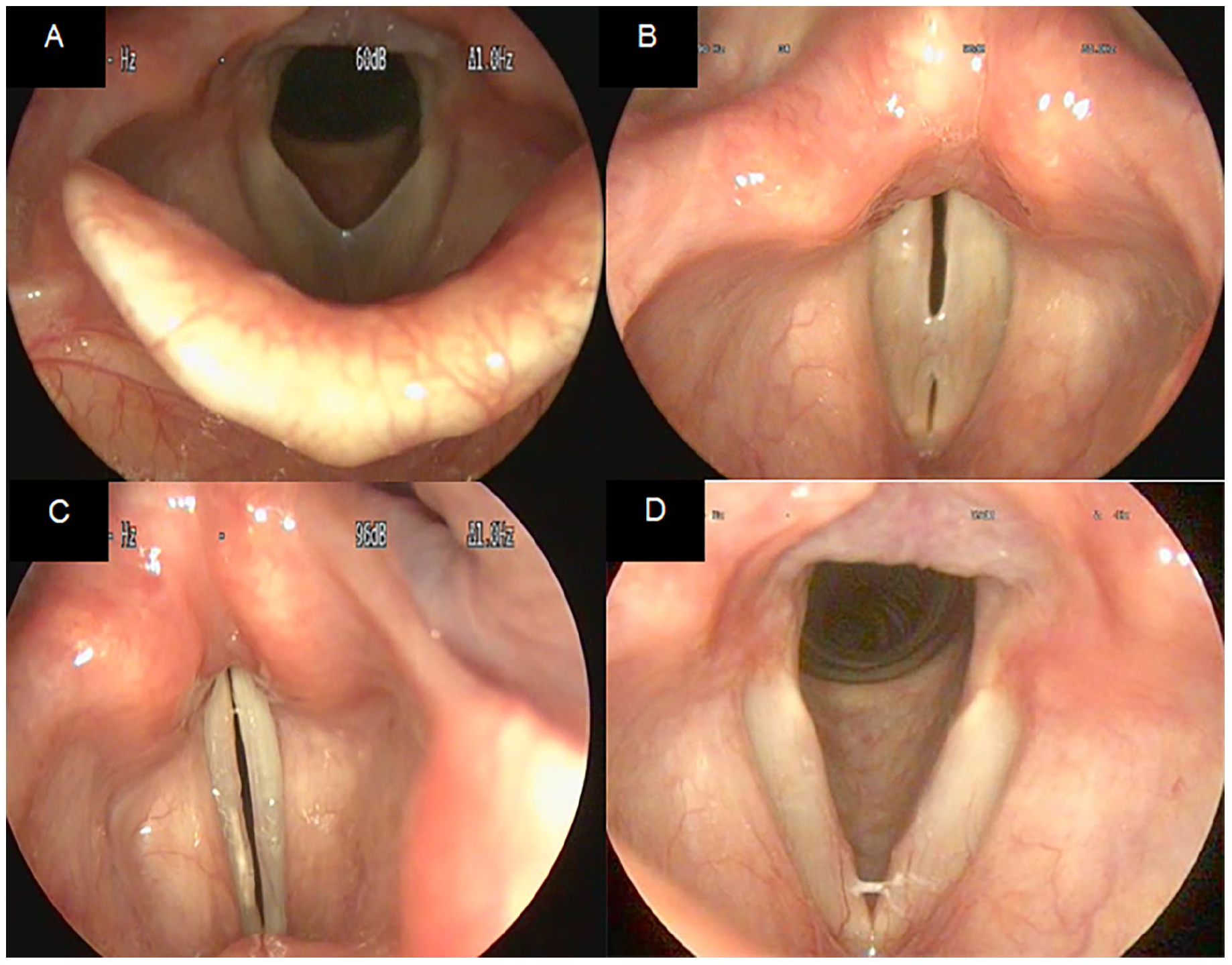
In-clinic views of glottic web with vocal folds with respiration (A) and phonation (B) prior to intervention, in-clinic 3-week postoperative view of vocal folds without residual web or adhesion (C), and in-clinic 4-month postoperative view of vocal folds with bilateral nodules (D).
Discussion
A glottic web is an abnormal scar band of mucosal tissue involving the vocal folds as anterior commissure webs or posterior commissure scarring, leading to dyspnea and dysphonia. Our unique case highlights a mid-vocal fold web arising from phonotrauma in the setting of occupational voice use and URI, where coughing secondary to infection was likely a risk factor. Emmet et al reported a case of dysphonia and an acquired anterior glottic web in a 3-year-old female following severe coughing with pneumonia that they attributed to phonotrauma. 5 Dominguez et al found mid-membranous webs in patients with prolonged intubation, neck radiation, or chronic cough following URI in a heavy smoker. 3 In contrast, our patient, a nonsmoker without radiation or iatrogenic trauma, presented with sudden-onset dysphonia secondary to a mid-glottic web with a normal anterior commissure. The combination of occupational voice use and coughing with inflammation from URI likely caused phonotrauma and the formation of a glottic web at the very site of maximum vocal fold mechanical stress, the mid-membranous vocal fold. The development of vocal fold nodules after she had healed from surgery further suggests poor vocal hygiene as the inciting factor.
Our patient’s glottic web was treated with cold instrumentation lysis and corticosteroid injection. Common approaches for anterior webs include the endoscopic flap technique for small anterior glottic webs and placement of a keel for larger webs. 1 For posterior glottic stenosis, techniques range from endoscopic lysis and balloon dilation to flaps and graduated arytenoidectomies to enhance mobilization. 2 In this case, the patient’s glottic web did not require a keel or flap, as it did not involve the anterior commissure, similar to the 4 cases of mid-membranous webs treated with sharp dissection. 3 Once lysed, the mid-cord location made the distance between healing surfaces sufficient to avoid a high risk of reformation.
Conclusion
In conclusion, we report the fifth case of a mid-membranous glottic web, a very rare and only recently described laryngeal pathology. This is the first attributed to occupational voice use with concomitant URI. It underscores the importance of a thorough evaluation of persistent dysphonia and dyspnea in patients with heavy voice use, as it can lead to uncommon laryngeal pathologies at points of maximum contact during phonation. Long-term monitoring, voice therapy, and vocal hygiene are important for preventing recurrence.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual case reports.
Consent for Publication
Written permission was obtained from the patient for the publication of this case report.
Author Contributions
C.N.: drafting and revision of manuscript, interpretation of data, and final approval. S.C.: design of the work, interpretation of data, revision of the manuscript, and final approval. T.L.S.: concept of the work, acquisition and interpretation of data, revision of the manuscript, and final approval.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are archived in the electronic medical record (EMR) system and are not publicly available as this would breach HIPAA, which protects patient privacy.