
Abstract
Lemierre’s syndrome (LS) is a rare and potentially life-threatening condition characterized by septic thrombophlebitis within the head and neck region. The lack of a standardized definition in the literature contributes to its limited evidence base. LS presents with various clinical manifestations, often showing atypical features across different age groups. Early diagnosis of LS is challenging due to its nonspecific nature. Recent evidence highlights significant short- and long-term morbidity risks. Successful management requires a multidisciplinary approach and appropriate antibiotic therapy. While LS is commonly associated with oropharyngeal infections, it can also arise from non-oropharyngeal sources, complicating diagnosis and management. We present a case of LS secondary to acute isolated sphenoid sinusitis in an 86-year-old woman. Imaging revealed multiple metastatic septic thrombophlebitis, including bilateral cavernous, inferior petrosal, right transverse and sigmoid sinuses, and internal jugular veins. Blood cultures grew Streptococcus intermedius, and endoscopic sphenoidotomy identified a fungus ball, with cultures confirming Streptococcus anginosus and Aspergillus fumigatus. The patient demonstrated significant recovery with no complications at follow-up. This case illustrates a complex, multifocal pattern of septic thrombophlebitis, extending to multiple venous structures, highlighting the need for comprehensive imaging and a multidisciplinary approach in diagnosing and managing this rare complication. Early recognition of LS, even in the context of non-oropharyngeal infections, is crucial for optimal treatment and improved outcomes.
Introduction
Lemierre’s syndrome (LS) is characterized by a history of recent oropharyngeal infection, clinical or radiological evidence of internal jugular vein thrombosis, and the isolation of anaerobic pathogens, predominantly Fusobacterium necrophorum.1-3 Although there is widespread consensus on the primary features of LS, its exact definition is still debated. Some authors limit the primary infection to the oropharynx, while others include any head and neck infection.1-4 Lemierre noted that the abdomen and pelvis could serve as primary sites of infection, though some authors exclude these from consideration.1-4
Isolated sphenoid sinusitis is a rare and often elusive condition, accounting for just 1% to 2.7% of all paranasal sinus infections. 5 Headache is the most prevalent symptom, occurring in 50% to 98% of cases, though it is often diffuse and lacks a specific location.5-7 Due to its subtle and nonspecific symptoms and deep anatomical location adjacent to critical structures, including the optic nerve, internal carotid artery, and cavernous sinus, early diagnosis is challenging, and the risk of severe complications is significant.5-7
There is now broad agreement that radiologic demonstration of a thrombus in the internal jugular vein is not required for the diagnosis of LS, as such clots may be easily overlooked and do not necessarily persist throughout the clinical course.1-4 Similarly, isolation of Fusobacterium spp. is no longer mandatory, as this organism is challenging to culture, results may be negative due to prior empiric antibiotic therapy, and other bacterial pathogens, including Streptococci, Eikenella corrodens, and Staphylococcus aureus, are also implicated in LS.1-4 Consequently, LS is increasingly regarded as a specific presentation within the broader spectrum of bacterial thrombophlebitis, encompassing conditions linked to various primary infections caused by diverse microbial agents.
Case Report
An 86-year-old woman presented to the emergency department with a 4-day history of progressively worsening headache, severe anterior neck pain, nausea, and vomiting. Her past medical history was significant for hypertension and 2 prior malignancies: invasive ductal carcinoma of the right breast and clear cell adenocarcinoma of the endometrium, both in remission. On examination, the patient appeared uncomfortable but afebrile. Laboratory investigations revealed a marked inflammatory response, characterized by leukocytosis of 29 × 109/L and an elevated C-reactive protein level of 421 mg/L (reference: <5 mg/L).
Contrast-enhanced computed tomography (CT) and magnetic resonance imaging (Figure 1) revealed complete opacification of both sphenoid sinuses alongside widespread venous thromboses. Bilateral cavernous sinus thrombosis was identified, extending anteriorly to involve the superior ophthalmic veins and causing intraconal fat hemorrhage. Inferiorly, the thrombosis spread to both inferior petrosal sinuses, the right superior petrosal sinus, and further involved the right transverse and sigmoid sinuses. An additional extension was noted into both internal jugular veins and adjacent venous structures. On the right side, internal jugular vein thrombosis was diffuse, while on the left, a focal thrombus was observed in the proximal segment. Blood cultures obtained on admission grew Streptococcus intermedius, confirming bacteremia.
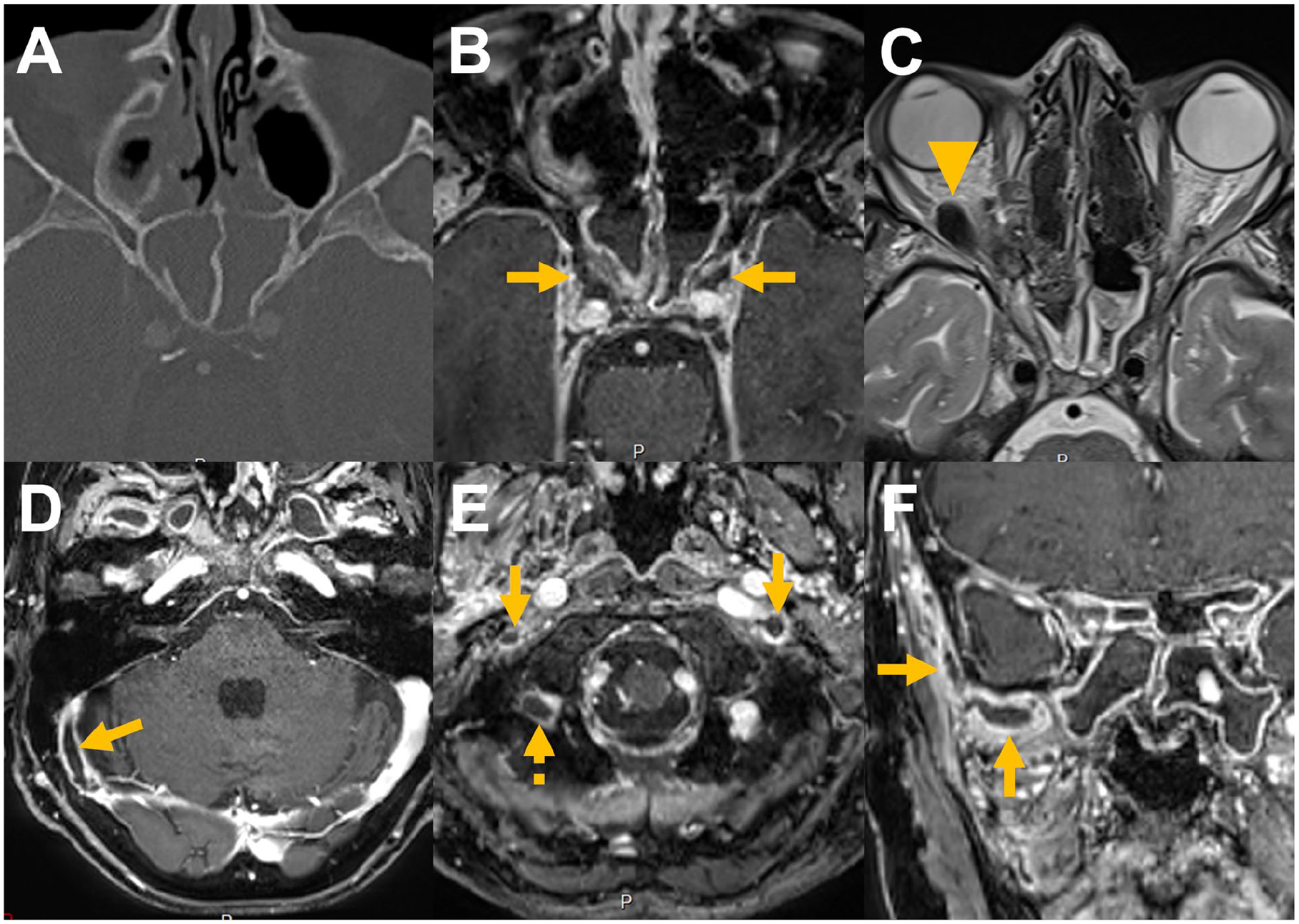
CT and MRI images on admission. (A) CT image on admission shows opacification of both sphenoid sinuses with no bone erosion. (B) MRI reveals bilateral cavernous sinus thrombosis (arrows). (C) Anterior extension of the thrombosis involves the superior ophthalmic veins, causing intraconal hemorrhage in the right orbit along the lateral rectus muscle (arrowhead). (D) Inferior extension includes thrombosis of the inferior petrosal sinuses (not shown), right superior petrosal sinus, and right transverse-sigmoid junction (arrow). (E) Thrombosis extends to the proximal internal jugular veins bilaterally (arrows) and the right occipital vein (dashed arrow). (F) Additional involvement of the right pterygoid venous plexus and superficial temporal vein is observed (arrows). CT, computed tomography; MRI, magnetic resonance imaging.
Urgent endoscopic sphenoidotomy revealed a large amount of purulent material and a fungus ball within the left sphenoid sinus, both of which were evacuated. Samples from the sinus were sent for microbiological and pathological analyses. Cultures identified Streptococcus anginosus and Aspergillus fumigatus, while histopathology confirmed a fungus ball without evidence of mucosal or bony invasion.
Postoperatively, the patient was treated with intravenous co-amoxicillin and voriconazole, which were later transitioned to oral formulations. Anticoagulation with unfractionated heparin was initiated and subsequently switched to oral apixaban for a planned 3-month course, considering the extent of thrombosis. During hospitalization, the patient’s symptoms improved significantly, with resolution of the inflammatory markers. However, she experienced transient binocular diplopia, attributed to retro-orbital hemorrhage secondary to thrombosis of the right superior ophthalmic vein, which resolved gradually. She demonstrated a favorable clinical response and was discharged with plans for ongoing follow-up. During the 3-month follow-up, no new neurological issues emerged, and anticoagulation was appropriately discontinued as planned.
Discussion
LS was common before antibiotics, but its incidence declined following their introduction for oropharyngeal infections, earning it the label “forgotten disease” in the 1990s.1-4 Retrospective analyses of microbiology laboratory data estimate the annual incidence of LS at 0.8 to 3.6 cases/million population.1-4,8 However, the condition predominantly affects adolescents and young adults, with higher incidence rates reported in these groups: 14.4 cases/million among individuals aged 14 to 25 years in Denmark (1998-2001) and 16 cases/million among those aged 15 to 19 years in Sweden (2017), compared to 1.4 cases/million annually in those over 40 years.1-4,8,9
LS of oropharyngeal origin predominantly affects young adults.1-4 Otomastoiditis as the source is more common in children, while extracranial F. necrophorum infections typically occur in middle-aged adults.1-4 A review of the literature and experimental data suggests a potential association between Epstein-Barr virus infectious mononucleosis and LS, emphasizing the need for heightened clinical awareness of this rare but significant link. 10
Mortality from LS was high in the pre-antibiotic era, with 90% of cases in Lemierre’s original series being fatal.1-4 In the 21st century, mortality rates are lower, around 2% to 4%, but may increase with delayed antibiotic treatment.1-4 A systematic review identified the tonsils, pharynx, and chest as the primary sources of infection, with the larynx and middle ear less commonly involved. 1 The most frequent initial presentation was sore throat, followed by neck mass and neck pain. 1
LS typically progresses in 2 stages. The first stage is the primary infection, often presenting as acute pharyngitis with sore throat, sometimes accompanied by fever. A systematic review found that 73% of patients had recent acute oropharyngeal symptoms, though infections from other sites, such as the ear and lower respiratory tract, were also noted. 3 The second stage involves internal jugular vein thrombophlebitis and sepsis, usually occurring days after the primary infection. Sepsis or septic shock may obscure the primary infection, complicating early diagnosis.
Metastatic lesions (ascending or descending septic emboli) to organs such as the lungs, joints, brain, and liver are common, with the lungs being most frequently affected, leading to pneumonia, abscesses, or pulmonary emboli.1-4 Rarely, the central nervous system is affected, leading to high morbidity.1-4 Despite improved mortality post-antibiotics, patients remain at risk of in-hospital morbidity and long-term sequelae, such as cranial nerve palsy and paralysis.1-4 All clinicians managing LS should remain vigilant to the potential for serious morbidity and maintain clinical awareness throughout the patient’s hospital stay.
Compared to a systematic review of LS, this report highlights an unusually extensive and multifocal thrombosis pattern, involving both cavernous, inferior, and superior petrosal and transverse and sigmoid sinuses, extending to the internal jugular veins bilaterally. 1 While thrombosis of individual sinuses or veins is noted in the literature, such widespread involvement across multiple venous structures in a single patient has not been previously reported.
LS can present diagnostic challenges in its early stages, as it frequently resembles more common etiologies of sore throat.1-4 At diagnosis, over 80% of LS patients exhibit multi-organ involvement, most commonly septic embolism affecting the lungs, musculoskeletal system, or intracranial regions.1-4,8,9 LS is often diagnosed only after the incidental isolation of Fusobacterium necrophorum, which can delay appropriate management.1-4,8,9 A high index of suspicion is crucial in primary and acute care settings to ensure timely diagnosis, particularly given the rarity, limited exposure in medical training, and variable presentation, especially from non-oropharyngeal sites.
LS management requires a multidisciplinary approach.1-4 The primary treatment involves antibiotics, typically beta-lactams or carbapenems combined with metronidazole, with adjustments based on sensitivity results.1-4 Although the optimal duration of antibiotic therapy is not standardized, studies suggest an average treatment course of 3 to 5 weeks.1-4,8,9 Surgical interventions may be necessary for metastatic lesions. Evaluation of LS includes throat and blood cultures along with imaging studies. While ultrasound can detect internal jugular vein thrombosis, the first-line imaging modality is contrast-enhanced CT of the neck.1-4 Additional CT scans may be warranted to evaluate other systems for infection or emboli.1-4 Successful treatment relies on awareness of the condition, a high index of suspicion, and a multidisciplinary team approach. 1
The role of anticoagulation in LS remains controversial. Anticoagulation therapy is often guided by personal experience or departmental protocols rather than strong evidence.1-4,11 Anticoagulation is used in 23% to 56% of cases, but evidence supporting its benefit is limited and based on retrospective studies.1-4,11 A meta-analysis showed no significant effect on vessel recanalization or mortality. 12 While anticoagulation may be considered for select cases, including cavernous sinus thrombosis, its optimal duration and choice of agents remain uncertain.11,12
Conclusion
In the present case, LS developed as a complication of acute isolated sphenoid sinusitis, leading to multiple dural sinuses and bilateral internal jugular vein thrombosis. This unique presentation demonstrates a complex multifocal pattern of septic thrombophlebitis that has not been previously described in a single patient in the literature. The case underscores the importance of maintaining a high index of suspicion for LS, even in non-oropharyngeal infections, to facilitate early diagnosis and optimal management. Furthermore, it highlights the critical role of comprehensive imaging and multidisciplinary care in diagnosing and managing such complex presentations.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from the participant included in the report.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.